Abstract
Treatment of the brow is necessary to correct lateral hooding. By lifting the brow in a superior and lateral direction, a tired and aged brow can be rejuvenated. When combined with an upper blepharoplasty, the following technique is very effective and can be performed under local anesthesia.
36 Brow and Forehead: Lateral Brow Lift
Key Points
The width of the area of lateral temporal tissue excision is based on the degree of brow ptosis, approximately a 4:1 ratio (width of tissue excision to expected lateral brow lift) is used.
Medially, the dissection is in the subperiosteal plane, protecting the supraorbital nerve.
Laterally, the dissection is deep to the superficial layer of deep temporal fascia (exposing the temporal fat pad), protecting the facial nerve.
36.1 Preoperative Steps
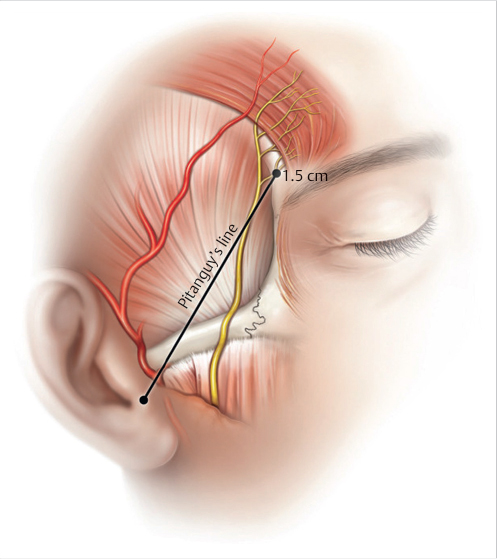
The procedure is performed via a 4 to 5 cm temporal incision parallel to the brow and 2 to 3 cm posterior to the temporal hairline.
The width of the scalp excision is planned to effect brow elevation in a 4:1 ratio. Based on this, standard upper blepharoplasty markings are made (Fig. 36.1).
Scalp incisions allow access to the zones of adhesion.
The upper eyelid approach allows access to the medial brow depressors, lateral temporal area, orbital retaining ligament, and periosteal/galeal attachments.
Medially, the dissection is in the subperiosteal plane, which protects the supraorbital nerve.
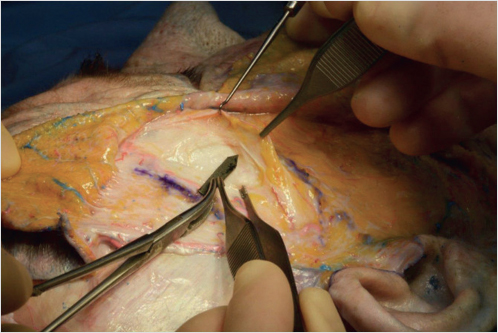
Laterally, the dissection is deep to the superficial layer of deep temporal fascia (exposing the temporal fat pad) which protects the frontal branch of the facial nerve (Fig. 36.2 and Fig. 36.3).

36.2 Operative Steps
See Video 36.1.
36.2.1 Upper Blepharoplasty Access
Local anesthesia is infiltrated in all areas of planned dissection.
The upper blepharoplasty incision is made.
Medially, the corrugator and procerus are exposed. The corrugator is found deep to the orbicularis oculi.
A Ragnell retractor can be used to protect the supraorbital artery and nerve.
The corrugator muscle is divided with fine bipolar cautery.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


