Abstract
Periorbital rejuvenation consultation requires a detailed preoperative analysis to identify all aspects that may be contributing to periorbital aging. The surgeon should have a thorough understanding of periorbital anatomy in order to properly assess the patient. The periorbital examination should be approached in a top-down systematic method. Basic preoperative medical history and a focused ophthalmologic history should be obtained.
29 Periorbital Rejuvenation Consultation
Key Points
The periorbital region is a critical component of facial rejuvenation.
A detailed preoperative analysis is critical to identifying all aspects contributing to periorbital aging.
Thorough preoperative analysis will also help identify patients with anatomic predisposition to lower eyelid malposition or dry eyes.
29.1 Preoperative Steps
The first step in the consultation is to obtained a through medical history that includes the following:
History of hypertension, cardiac disease, bleeding or clotting disorders, diabetes, thyroid dysfunction, and autoimmune disease.
Once the medical history has been obtained, the surgeon should obtain a focused ophthalmologic history including the following:
When was the last time the patient had his or her visual acuity checked?
Does he or she use any corrective lenses or glasses?
Any prior history of facial or periorbital trauma, glaucoma, excess tearing and/or dry eyes, prior ophthalmologic/periorbital surgery, or LASIK or refractive surgery?
A systematic approach should be used for the periorbital physical examination:
The presence of the protective Bell’s phenomenon is documented, which is the upward movement of the globe with eye closure.
Forehead and brow examination:
Brow and forehead should be part of a comprehensive periorbital examination.
Presence of hyperactive frontalis and brow elevation should be noted at baseline. The patient should be asked to relax the forehead in order to determine the resting brow level.
In females, the eyebrow should be 1 cm above the supraorbital rim, and slightly peaked at the lateral third. The eyebrow may be at the level of the supraorbital rim in males without peaking laterally.
Forehead length should be documented. The normal length is 6 cm.
Fat atrophy in the supraorbital region particularly in the central, middle, and lateral temporal fat compartments should be documented.
Skeletal support:
The underlying skeletal support of the periorbita should be examined. This includes the orbital rim, zygomatic prominence at the malar eminence, and temporal bone of the forehead.
Facial aging includes a component of bone resorption, which may also contribute to some of the findings in periorbital aging.
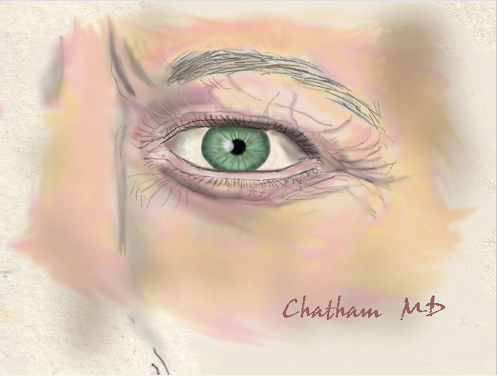
Upper eyelid skin quality and quantity (Fig. 29.1):
The upper eyelid is examined with the eyebrows at resting neutral position.
Dermatochalasis is the extent of excess upper eyelid skin.
Supratarsal fold location should be about 6 to 7 mm above the lash line. An elevation in this with eyelid ptosis is indicative of levator dehiscence.
Upper eyelid position:
The upper eyelid position is determined relative to the superior limbus.
Marginal to reflex distance 1 is the measured distance from the upper eyelid to the corneal light reflex. The normal value is 4 mm. Values less than this indicate the degree of blepharoptosis.
Levator excursion:
This is the value given to the distance the upper eyelid moves from inferior to superior gaze.
Values for normal function are between 10 and 15 mm, moderate function is 5 to 10 mm, and poor function is 0 to 5 mm.
Lower eyelid position (Fig. 29.2):
The lower eyelid should sit at the inferior corneo-scleral junction. Any scleral show between these points indicates lower eyelid ptosis secondary to one of two common causes: lateral canthal laxity or lower eyelid horizontal excess.
The lower eyelids should be examined for protuberant fat from the three compartments along with the presence of a tear trough deformity.
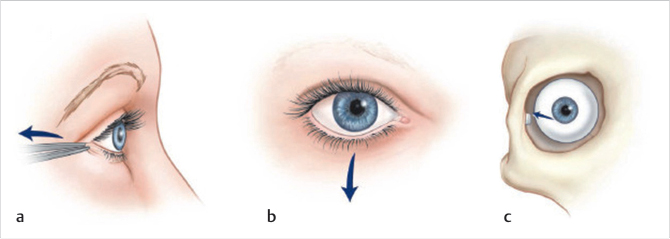
Lateral canthal position (Fig. 29.3a–c):
The lateral canthus should be 2 mm superior to the medial canthus with a positive tilt. Lack of a positive tilt indicates lateral canthal laxity.
The lateral canthal angle should be sharp. A blunted angle indicates lateral canthal laxity or a history of prior surgery.
Anterior distraction:
The lower eyelid is distracted anteriorly to the globe. A distraction of >6 mm indicates horizontal excess, best managed with a lateral tarsal strip canthoplasty.
Snapback test:
This test evaluates the lower eyelid tone. The lower eyelid is pulled inferiorly and then allowed to return to normal position without the blinking mechanism. A sluggish return to normal indicates poor tone.
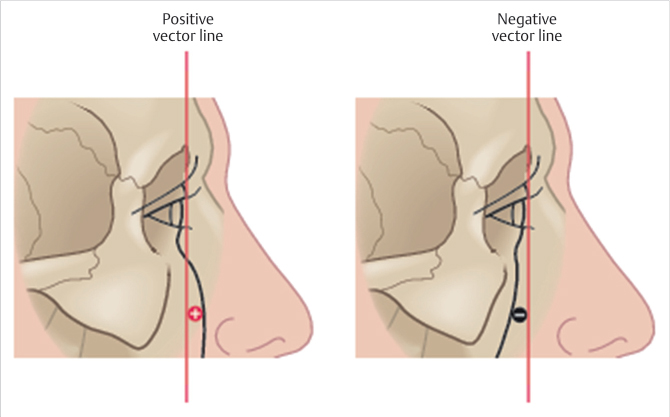
Malar eminence vector (Fig. 29.4):
A critical part of the examination is determining whether the patient has a positive or negative vector.
A positive vector is demonstrated when the malar eminence is anterior to the corneal surface of the globe on lateral view.
A negative vector is demonstrated when the malar eminence is posterior to the corneal surface of the globe.
Patients with a negative vector are at an increased risk for lower eyelid malposition after lower eyelid blepharoplasty.
Dry eye:
In patients with a history of dry eye, a Schirmer’s test is performed.
Patients who demonstrate an abnormal Schirmer’s test are referred for ophthalmologic evaluation.
(Reproduced with permission from Codner M, McCord C, eds. Eyelid & Periorbital Surgery. 2nd ed. Thieme; 2016.)
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


