Parasite Infestations in Cutaneous Infections
J. Olufemi Ogunbiyi
Alejandro A. Gru
SCHISTOSOMIASIS
Definition and Epidemiology
Schistosomiasis is the most important trematode as a cause of dermatologic manifestations. It is also known as bilharzia or “snail fever,” as the parasite is carried by freshwater snails.1,2,3,4,5 It is caused by the human flukes Schistosoma haematobium (urogenital diseases), Schistosoma mansoni, and Schistosoma japonicum (gastrointestinal (GI) and liver disease), which are released by their snail intermediate hosts into freshwater. Humans get infected after recreational or occupational contact with freshwater that has free-swimming cercariae. The main types of exposure to infected water are connected to agricultural, fishing, domestic, and recreational activities.6
Etiology
S. haematobium and S. mansoni are endemic in Africa, Middle East, and Latin America, whereas S. japonicum is endemic in East Asia. S. intercalatum is found in parts of west and central Africa. In endemic areas, about 60% to 80% of cases are seen in children. It affects more than 200 million people worldwide.2,3,5 All species are acquired by swimming and bathing in waters inhabited by schistosomes. The larvae emerge from the snails and swim in the water until they come in contact with an individual and penetrate the skin. Once inside the body, the larvae develop into adult male and female worms, which pair up and live together in the blood vessels from years, particularly in the venous system of the rectum and bladder. Female worms release thousands of eggs, which travel to the bladder and intestines, and are subsequently passed in the feces and urine. The eggs hatch and release the miracidia that swims in search of a member of the snail species that is specific for each schistosome species. The snail is an intermediary host, and within it, the cercariae develop into its infective form. The definitive hosts that are responsible for the disease are mammals or birds, where the cercariae complete their life cycle.
Clinical Presentation
Schistosomes produce cutaneous lesions at the site of skin penetration of the schistosomule (cercariae).4,6,7,8,9,10,11 The typical lesion is referred to as the “swimmer’s itch” (cercarial dermatitis)4 and results from a cutaneous deposition of ova or hypersensitivity to the cercaria or ova of the parasite, leading to an urticarial reaction. Cercarial dermatitis is an acute itchy erythematous popular or urticarial rash that occurs within hours of cercarial penetration into the skin and it is usually followed by fever, headache, diarrhea, etc (also known as “Katayama fever”).
Clinically, the most commonly affected areas include the genital and perineal sites forming multiple papular and nodular lesions (infrequently extragenital cutaneous depositions may be seen in children).10,11,12 Widespread dissemination of the cercariae and/or ova could lead to an urticarial reaction to the parasite.
Histologic Findings
The histologic findings of cercarial dermatitis include the presence of a dermal suppurative acute inflammatory process with infiltration by neutrophils and a large proportion of eosinophils.5,6,13 The ova of Schistosoma are usually seen
in the dermis stimulating a granulomatous inflammation with variable eosinophilic infiltrates. In some occasions, eosinophilic flame figures can be present. Foreign body-type giant cells are seen attempting to ingest the ova. In older lesions, there is calcification of the ova. Species identification can be determined by the location of a spine or knob (terminal/apical spine for S. haematobium, a lateral spine for S. mansoni and a knob for S. japonicum)6 (Figure 21-1).
in the dermis stimulating a granulomatous inflammation with variable eosinophilic infiltrates. In some occasions, eosinophilic flame figures can be present. Foreign body-type giant cells are seen attempting to ingest the ova. In older lesions, there is calcification of the ova. Species identification can be determined by the location of a spine or knob (terminal/apical spine for S. haematobium, a lateral spine for S. mansoni and a knob for S. japonicum)6 (Figure 21-1).
The basic lesions of Schistosomiasis include (1) a circumscribed granuloma around eggs or (2) a diffuse cellular infiltrate around eggs. Eosinophils and neutrophils usually predominate in the diffuse dermal infiltrate, but plasma cells, lymphocytes, macrophages, and giant cells can also be present.6 The circumoval granulomas, also called pseudotubercles, are primarily reactions of delayed hypersensitivity, but the immunologic mechanisms of the diffuse reactions are not known. The only pathognomonic finding is the presence of schistosomal eggs. Sometimes, the eggs can be surrounded by a layer of eosinophilic material, the so-called Splendore-Hoeppli phenomenon. Pseudoepitheliomatous changes can also be present (Figure 21-2).
CAPSULE SUMMARY
SCHISTOSOMIASIS
Schistosomiasis is the most important trematode that causes dermatological manifestations and is caused by the human flukes S. haematobium (urogenital diseases), S. mansoni, and S. japonicum (GI and liver disease). Schistosomes produce cutaneous lesions at the site of skin penetration of the schistosomule (cercariae) which is referred to as swimmer’s itch, cutaneous deposition of ova or hypersensitivity to the schistosomule or ova of the parasite. Histopathologically, in cercarial dermatitis there is area of suppuration with collection of eosinophils and features of acute inflammation. The ova of Schistosoma are usually seen in the dermis with stimulation of granulomatous inflammation with variable eosinophilic infiltrates. Foreign body type giant cells are seen attempting to ingest the ova.
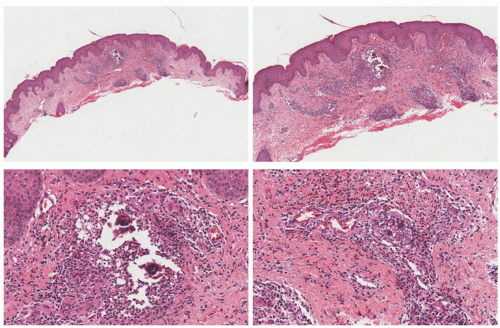 FIGURE 21-1. Histology of schistosomiasis. Digital slides courtesy of Path Presenter.com. |
CYSTICERCOSIS
Definition and Epidemiology
Cysticercosis is the result of the infection with the larval stage (cysticercosis cellulosae) of the human pork tapeworm, Tinea solium, which results in the infection of multiple organ sites, but particularly the central nervous system (CNS) (neurocysticercosis).14,15,16 The latter continues to be one of
the most important causes of seizures in the world.16 The disease is found in Eastern Europe, India, Pakistan, China, sub-Saharan Africa, South and Central America. It is usually more prevalent in low socioeconomic areas with poor hygiene and in areas where people live in proximity to pigs. It is not common in the United States, although it has been reported in immigrants.
the most important causes of seizures in the world.16 The disease is found in Eastern Europe, India, Pakistan, China, sub-Saharan Africa, South and Central America. It is usually more prevalent in low socioeconomic areas with poor hygiene and in areas where people live in proximity to pigs. It is not common in the United States, although it has been reported in immigrants.
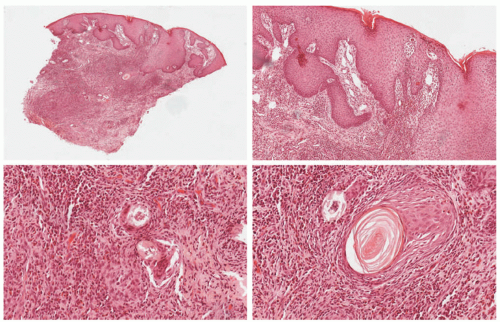 FIGURE 21-2. Chronic granulomatous inflammation with pseudoepitheliomatous changes in association with schistosomiasis. Digital slides courtesy of Path Presenter.com. |
Etiology
Cysticercosis results from a contamination of infected food and water, especially vegetables, with feces containing the eggs of the human pork tapeworm.15,16,17,18,19,20,21 The parasite has a life cycle that includes two hosts: humans and pigs. Humans are the only host of the adult tapeworm, whereas humans and pigs can be intermediate hosts for the larval form, the cysticercus. Autoinoculation also occurs from dirty contaminated hands. The coat of the eggs is digested in the stomach and oncospheres are liberated. The oncospheres invade the intestinal wall and enter the blood stream after which they migrate and get lodged in various organs, particularly the eyes, skeletal muscle, subcutaneous tissue, and CNS where they mature to become a cysticercus. Eating food contaminated by human feces then infects pigs. In the pig, the embryo penetrates the intestinal wall, and via the bloodstream, reaches the skeletal muscle to become a cysticercus. When humans ingest undercooked pork meat, the cycle is completed. If human ingests organisms (not eggs), the adult tapeworm develops into T. solium, which can measure up to 2 to 4 m in length.
Clinical Presentation
Cysticercosis has a peak incidence between the ages of 20 and 50. The cutaneous manifestations are characterized by the presence of subcutaneous nodules (cysticercosis cellulosae cutis), which are usually less than 2 cm in diameter (Figures 21-3 and 21-4).18,22,23,24 Cystic lesions of most tapeworms do not evoke an immunologic response when the cyst is alive. The nodules are usually painless, firm, and round. There may be few or up to a hundred in the same individual. The nodules may remain unchanged for years. The skin nodules should prompt for the evaluation of involvement of other organ sites. Cutaneous cysticercosis is more common in Asia than in the Americas or Africa. In approximately 50% of patients the lesions have been present for a month. The remaining 50% can have lesions for several years. The lesions can also affect mucosal areas, such as the tongue. Approximately 20% of patients have an isolated skin lesion, and 70% have less than 10 lesions. The typically affected cutaneous sites include the trunk, scalp, eyelids, face, tongue, neck, breasts, upper limbs, and thighs. In some occasions, the patients might experience a “popping” sensation in the lesion than can correlate with a rupture of the cyst. Muscle pain is also frequent and 10% can show calcifications by xray. A diagnosis can be established by the biopsy of one of the nodules.
 FIGURE 21-3. Photograph showing well-defined swelling in the right infraclavicular region. Obtained with permission from Chauhan S, Singh G, Khan I. Cysticercosis of the pectoralis major: a case report and review of literature. Am J Dermatopathol. 2017;39(3):e34-e37. |
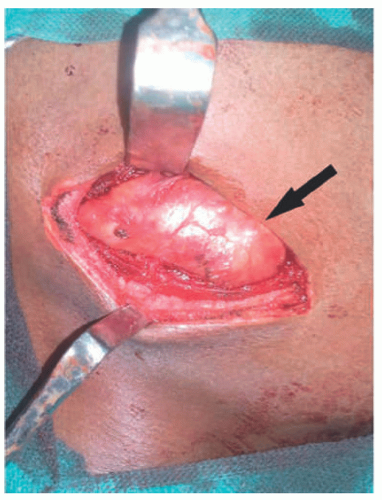 FIGURE 21-4. Intraoperative photograph showing a smoothwalled cyst within the muscle belly. Obtained with permission from Chauhan S, Singh G, Khan I. Cysticercosis of the pectoralis major: a case report and review of literature. Am J Dermatopathol. 2017;39(3):e34-e37. |
Histologic Findings
Viable cysticerci may be seen in tissue, compressing adjacent structures, but causing virtually no inflammatory response. When the whole larva is present, it is seen as a cystic structure surrounded by a vesicular wall. The lumen is folded and ribbon-like and contains the invaginated scolex. Occasionally, sucking discs and hooklets can be seen. Hooklets have a distinctive histologic appearance, as they appear as brown, refractile, sickle-shaped structures. However, when cysticerci degenerate, they elicit an inflammatory reaction with infiltration by neutrophils, histiocytes, and eosinophils. (Figures 21-5 and 21-6) A granulomatous reaction eventually develops, characterized by the presence of histiocytes, epithelioid cells, and foreign body giant cells. Ultimately, this leads to fibrosis and calcification.17,23,25,26
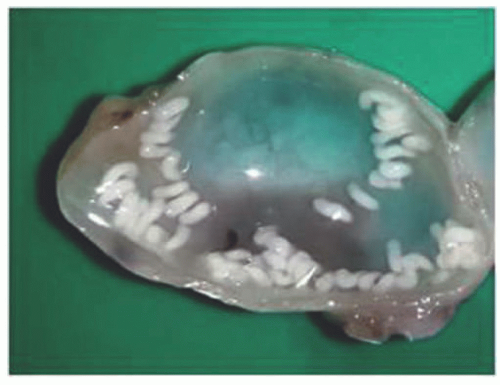 FIGURE 21-5. Cysticercal larva. |
CAPSULE SUMMARY
CYSTICERCOSIS
Infection with the larval stage (cystercicosis cellulosae) of the human pork tapeworm, T. solium, results in the infection of multiple organ sites, but particularly the central nervous system. Cystercicosis results from contamination of infected food and water, especially vegetables, with feces containing the eggs of the human pork tapeworm. Autoinoculation also occurs from dirty contaminated hands. The oncospheres invade the intestinal wall and enter the blood stream after which they migrate and get lodged in various organs, particularly the eyes, skeletal muscle, subcutaneous tissue, and central nervous system.
ONCHOCERCIASIS
Definition and Epidemiology
Onchocerciasis is a filarial infection caused by the worm Onchocerca volvulus, leading to a variety of skin manifestation and blindness. It is endemic in some parts of sub-Saharan Africa especially West Africa, Yemen, Central, and South
America. It is estimated that 18 million people are living with onchocerciasis and 99% of these reside in Africa.27,28,29,30,31
America. It is estimated that 18 million people are living with onchocerciasis and 99% of these reside in Africa.27,28,29,30,31
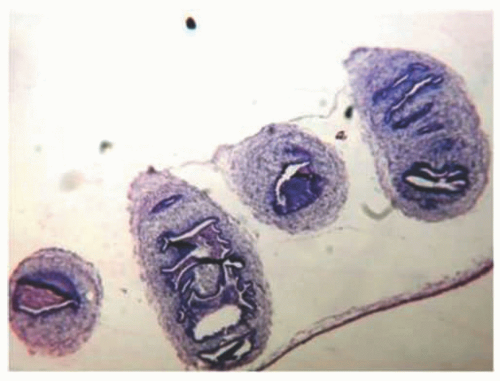 FIGURE 21-6. Histology of cysticercosis. |
Onchocerciasis does not have any racial predilection, but it has been observed that the cutaneous findings are more common in the forested areas, whereas blindness is more common in the Savannah areas, possibly resulting from some type of genetic predisposition.32
Etiology
The vector of the disease is the Simulium (black fly), which is found around flowing water; hence Onchocerciasis is also known as “river blindness.” Simulium damnosum is a species complex of 55 named cytoforms (cytospecies and cytotypes) and constitute the largest known species complex of any vector. It is distributed throughout sub-Saharan Africa and the Arabian Peninsula but is limited to being an onchocerciasis vector distributed in Uganda, Benin, Burkina Faso, Cameroon, Central African Republic, Ghana, Guinea, Guinea-Bissau, Ivory Coast, Liberia, Mali, Niger, Nigeria, Senegal, Sierra Leone, Sudan, and Togo.30,31
The Simulium fly takes a blood meal from an infected individual containing the microfilaria of Onchocerca volvulus. The microfilaria matures in the mouthparts of the fly to produce the larval stage. The larvae are introduced back into the humans by the bite of the Simulium fly. The larvae migrate to different parts of the body, but especially to the dermis, where adult Onchocerca volvulus worms develop (male and female). The worms reside in nodules known as Onchocercomata. The female and male worms mate and the fertilized female then produces microfilariae which move to different parts of the body, especially to the eyes and skin. They can also be eaten by the Simulium fly again.
Clinical Presentation
The cutaneous findings of onchocerciasis are variable.33,34 Factors that affect the clinical features include the age, geographical location, and immunity of the patient toward the microfilaria. Other factors include the duration of infection and the number of infecting organisms. The commonest symptom is pruritus that may be localized or generalized. However, microfilaria in the skin may be asymptomatic. Cutaneous findings of onchocerciasis include onchocercal dermatitis and skin nodules. Infected individuals may also become blind, especially when cutaneous findings occur on the head.
The clinical features can be different in accordance with the duration of the infection.28,29,34,35 The acute findings include pruritus and inflammation of skin with edema, causing obliteration of the skin creases (the creases become less obvious). This presentation is more frequent in children. Vesicles and papules may be present. Nodules termed onchocercoma may be present at any stage especially on bony prominences. Patients with chronic disease have more papules, excoriation, lichenification, and postinflammatory hyperpigmentation. These are common on the covered areas, especially the trunk and buttocks. A distinct chronic form of the disease (with similar lichenification and postinflammatory dyspigmentation) with no skip areas affects the limb or contiguous sites and is also known as Swoda in Arabic-speaking countries. Enlarged regional lymphadenopathy may also be present, giving the hanging groin sign when the inguinal region is affected. Atrophy of the skin and hypopigmentation are also seen in long-standing cases, especially on the shins, even in the absence of microfilaria (Figure 21-7).
Diagnosis can be made clinically and confirmed by examination of skin snips or biopsy of nodules, which may reveal active microfilaria. ELISA can also be performed as an ancillary technique when it is difficult to demonstrate the organisms.
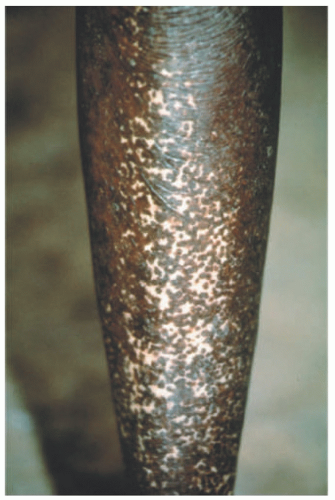 FIGURE 21-7. Skin in onchocerciasis (clinical). |
Histologic Findings
Onchocercal nodules usually contain several adult worms in the dermis surrounded by an inflammatory reaction that varies from suppurative to granulomatous, with fibrosis36 (Figures 21-8 and 21-9). The organizing inflammatory process can also be associated with calcification and ossification. A layer of fibrinoid material may be seen covering the worms. The overlying epidermis shows hyperpigmentation with acanthosis and melanin pigment incontinence.
Dermal changes are minimal in the early stage and are characterized by edema and the presence of a chronic inflammatory infiltrate with scattered lymphocytes, histiocytes, plasma cells, and eosinophils around vessels and skin appendages.
It is the degenerating microfilaria that tends to provoke a granulomatous reaction and a rich infiltrate of eosinophils. Proliferating fibroblasts and mast cells may be seen, but neutrophils are typically absent. Microfilariae are most numerous in the upper dermis; they may be scant or abundant and are sometimes present within dermal lymphatics. In more advanced lesions, acanthosis, hyperkeratosis, focal parakeratosis, and melanophages are noted in the upper dermis, with dilated lymphatics, tortuous dermal vessels, and interstitial dermal mucin seen between dermal collagen fibers (which can be proven by a colloidal iron and alcian blue stains). The advanced fibrosis leads to a concentric layering of collagen around dermal vessels.
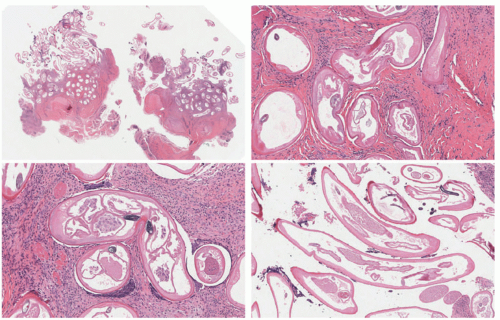 FIGURE 21-8. Histology of the skin in onchocerciasis. The transverse sections of the onchocerca demonstrate a prominent cuticle. Digital slides courtesy of Path Presenter.com. |
In onchocerciasis, fibrosis begins early in the disease, is persistent and, ultimately, fibrous tissue replaces the specialized structures of the skin. The papules of gale filarienne are intraepidermal abscesses, which contain microfilariae. These are also called craw craw. There are, sometimes, subcutaneous fibrous nodules containing microfilaria or adult worms in a background of a mixed population of inflammatory cells that include eosinophils, lymphocytes, and giant cells. The microfilaria may be gravid.
CAPSULE SUMMARY
ONCHOCERCIASIS
Onchocerciasis is a filarial infection caused by the worm Onchocerca volvulus, leading to a variety of skin manifestation and blindness. It is endemic in some parts of sub-Saharan Africa especially West Africa, Yemen, Central and South America. It is estimated that 18 million people are living with onchocerciasis and 99% of these reside in Africa. Cutaneous findings of onchocerciasis include onchocercal dermatitis and skin nodules. Onchocercal nodules usually contain several adult worms in the dermis surrounded by an inflammatory reaction that varies from suppurative to granulomatous, with fibrosis.
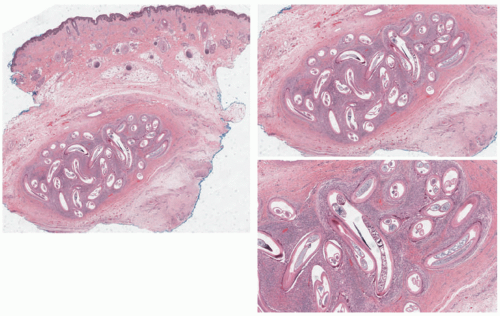 FIGURE 21-9. Histology of the skin in onchocercoma. Digital slides courtesy of Path Presenter.com. |
CUTANEOUS LARVA MIGRANS
Definition and Epidemiology
This is a cutaneous parasitic infestation, resulting from the migration of parasites through the skin. This disease occurs worldwide.37,38 However, it is seen more frequently in tropical climates where it affects children who play with soil contaminated with feces, especially on the beach, and in adults with soil-related occupations. In some areas of the world, the problem has led to the banning of pets from beaches. Cases of cutaneous larva migrans (CLM) have been reported at any age or sex.39,40,41 The prevalence and infection can be as high as 4% of adults and 15% of children. One-third of those children can develop superimposed bacterial infections. The disease is also known as “creeping eruption,” “creeping verminous dermatitis,” “sandworm eruption,” and “plumber’s itch.”
Etiology
The causative agents are larvae of nematodes, especially those of dog hookworms Ancylostoma braziliense, Ancylostoma Caninum, Uncinaria stenocephala, Bunostomum phlebotomum, and Necator americanus.36 However, the term also encompasses infections produced by other helminths, including trematodes (Fasciola) and cestodes (Spirometra). Humans are accidental hosts, so the life cycle of the worms cannot be completed in them. The eggs in the feces-contaminated soil hatch when the environment is conducive and the larvae penetrate the skin through fissures, follicles, or intact skin upon direct contact. The presence of the larvae and their products produce an immunologic response manifested by itching. In the appropriate host (animals), enzymes released by the worms enable them to penetrate into the dermis, blood vessels, and lungs, following a retrograde pathway through the trachea, larynx, and down the intestines to complete the cycle. In humans, the larvae are unable to pass through the basement membrane, and remain in the epidermis until they finally die over a period of weeks to months.
Clinical Presentation
The commonly affected sites include the hands, feet, buttocks, and trunk.38,42,43 The disease is more commonly associated with walking on a sandy beach either barefoot or in sandals. The initial penetration of the larvae may produce itching and an eczematous rash in the affected areas. The first clinical lesion is a papule, whereas the creeping aspect develops later. The larvae subsequently move in the skin, usually for short distances, producing significant itching, a serpiginous tract or tracts accompanied by erythema and vesicular eruptions, depending on the number of larvae involved.39,44 The larvae movement ranges across the different species, but it has an average of 2.7 mm/d (Figures 21-10, 21-11, 21-12, 21-13 and 21-14). Secondary lesions and bacterial overinfection (impetiginization) may occur. The lesions are usually self-limiting. The diagnosis is usually clinical and can be facilitated with the use of a dermoscope.
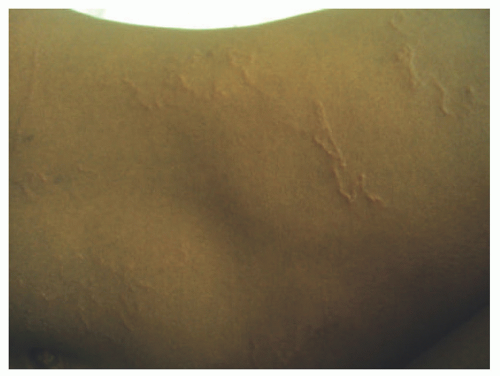 FIGURE 21-10. Clinical picture of cutaneous larva migrans. |
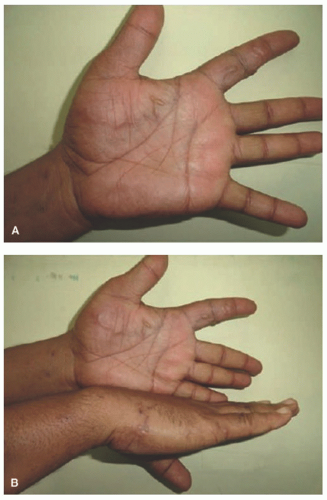 FIGURE 21-11. Multiple serpiginous tracks with a vesicle at the advancing end, one hand (A), both hands (B) in cutaneous larva migrans. Reprinted with permission from Podder I et al. Loeffler’s Syndrome Following Cutaneous Larva Migrans: An Uncommon Sequel. Indian J Dermatol. 2016;61(2):190-192. |
 FIGURE 21-12. Single erythematous, curvilinear, track over the forehead. Obtained with permission from Kaur S, Jindal N, Sahu P, Jairath V, Jain VK. Creeping eruption on the move: a case series from Northern India. Indian J Dermatol. 2015;60(4):422. |
 FIGURE 21-13. Single curvilinear track encircling the neck and sides of bilateral cheeks. Obtained with permission from Kaur S, Jindal N, Sahu P, Jairath V, Jain VK. Creeping eruption on the move: a case series from Northern India. Indian J Dermatol. 2015;60(4):422. |
Histologic findings
The diagnosis is usually based on the clinical appearance of the lesions (the presence of parasitic galleries and identification of parasites within the skin tunnels) and, therefore, biopsies are not usually taken.45 However, biopsies
may allow for differentiation from other creeping eruptions such as gnathostomiasis. Most biopsy specimens show only a sparse infiltrate of lymphocytes and eosinophils in the upper dermis and do not contain larvae. The larvae are usually present in burrows in the deeper layers of the epidermis. Biopsies taken from just beyond the leading edge of the track are the ones that most likely will reveal the larvae (Figures 21-15 and 21-16). The tracks of the larva form small epidermal cavitations and show a mixed population of inflammatory cell infiltrates
comprising eosinophils, neutrophils, lymphocytes, and plasma cells. There are intraepidermal vesicular lesions with associated eosinophilic spongiosis.
may allow for differentiation from other creeping eruptions such as gnathostomiasis. Most biopsy specimens show only a sparse infiltrate of lymphocytes and eosinophils in the upper dermis and do not contain larvae. The larvae are usually present in burrows in the deeper layers of the epidermis. Biopsies taken from just beyond the leading edge of the track are the ones that most likely will reveal the larvae (Figures 21-15 and 21-16). The tracks of the larva form small epidermal cavitations and show a mixed population of inflammatory cell infiltrates
comprising eosinophils, neutrophils, lymphocytes, and plasma cells. There are intraepidermal vesicular lesions with associated eosinophilic spongiosis.
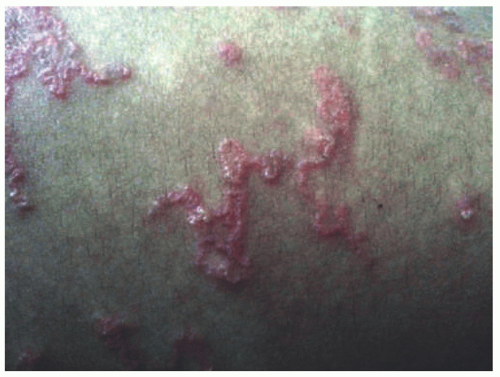 FIGURE 21-14. Multiple disseminated serpiginous tracks on the abdomen. Obtained with permission From Kaur S, Jindal N, Sahu P, Jairath V, Jain VK. Creeping eruption on the move: a case series from Northern India. Indian J Dermatol. 2015;60(4):422. |
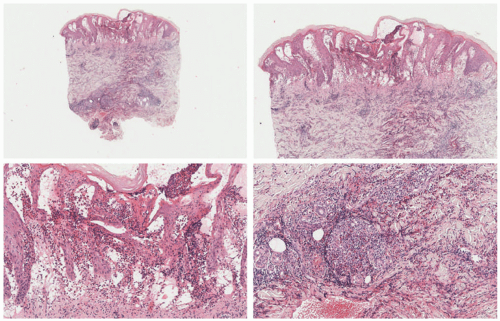 FIGURE 21-15. Cutaneous larva migrans. Marker intra- and subepidermal vesiculation is noted. A very intense eosinophilic inflammatory infiltrate is present. No larvae are seen. Digital slides courtesy of Path Presenter.com. |
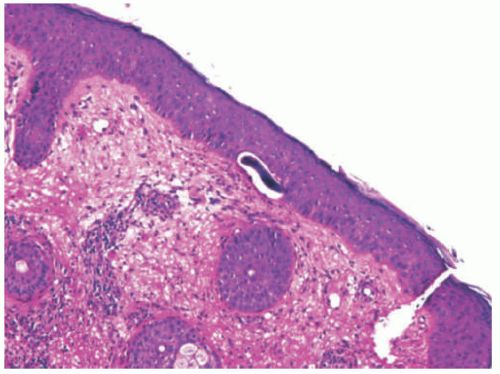 FIGURE 21-16. Cutaneous larva migrans. There is a nematode larva in the lower part of the epidermis. Obtained with permission from Mercado R, González-Chávez J, Sánchez JL, Figueroa LD. Erythematous plaque in the cheek of an HIV patient. Am J Dermatopathol. 2016;38(7):531-532. |
Identification of the species of the parasite is not readily done in tissue sections. Further penetration and invasion of the human dermis is not usually seen. The adult parasite is not seen in standard sections. The larva from hookworm-related CLM is small when compared with the larvae of Gnathostoma: the diameter of the formers is not wider than three keratinocytes, whereas Gnathostoma larvae are 0.3 mm in diameter and can be present in the dermis or subcutis. The former can be similar in size to the larvae of Strongyloides, but the latter usually presents in the dermis. Follicular localization has also been reported, and postulated as the point of entrance to the skin.
CAPSULE SUMMARY
CUTANEOUS LARVA MIGRANS
CLM is a cutaneous parasitic infestation, resulting from the migration of parasites through the skin. The disease is seen more frequently in tropical climates where is affects children who play with soil contaminated with feces, especially on the beach, and in adults with soil-related occupations. The commonly affected sites include the hands, feet, buttocks and trunk. The larvae moves within the skin, usually for short distances, producing significant itching, a serpiginous tract or tracts accompanied by erythema and vesicular eruptions, depending on the number of larvae involved. Biopsies are only rarely done.
GNATHOSTOMIASIS
Definition and Epidemiology
Gnathostomiasis is the infection produced by a larval stage of Gnanthostoma, a nematode that affects cats and dogs. It is associated with a migratory form of cellulitis or panniculitis. Several species have been identified in association with human disease. Most cases in Asia are associated with Gnathostoma spinigerum; other species include G. doloresi, G. nipponicum, and G. binucleatum (the latter responsible for the cases seen in Mexico and Ecuador).46,47,48,49
Etiology
The infection is commonly acquired after the ingestion of raw fish contaminated with the larva. All the countries with a diet rich in raw fish have a higher prevalence of this disease (Japan, Thailand, Cambodia, Laos, Myanmar, Indonesia, Philippines, Malaysia, China, Mexico, Ecuador, and Peru). In Asia, the infection is associated with the ingestion of sushi, sashimi, and eel dishes; in South America, it is associated with ceviche.47,50,51 The life cycle begins in the adult nest, located in the stomach of cats and dogs. Eggs produced by the female in the nest are expelled into the animal feces. When the feces reach the water of nearby rivers or flowing water, the eggs evolve into the first larvarial stage. The worm is ingested by a copepod, a water flea of the genus Cyclops. The evolution into the second larvarial state occurs in the second host. Large predators (fish, eels, birds, frogs, or reptiles) ingest the copepod, and it is in the second host that the larva migrates to internal organs, such as the liver or muscle, evolving into the third stage. Any mammal feeding on the contaminated second host may become infected. In the definitive host, the larva reaches the GI tract to evolve into the adult worms, completing the cycle. Humans are accidental hosts, where the larva begins by adhering into the intestinal mucosa, peritoneal cavity, and potentially the skin. In some cases, CNS involvement occurs.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


