Key Points
- ▪
Reductive procedures (direct excision with skin grafting or liposuction) alone or as an adjunct are effective in gross reduction of volume; however they carry significant morbidity.
- ▪
Direct excision with skin grafting is reserved for the most extreme cases of lymphedema in which function and activities of daily living are severely affected.
- ▪
Liposuction for reduction of excess adipose deposition requires lifelong postoperative compression garments.
- ▪
Physiologic methods (lymphovenous anastomosis (LVA) or vascularized lymph node transfer (VLNT)) tend to produce more modest reductions in volume; however, they produce less morbidity to donor and recipient sites.
- ▪
LVA seems most effective at early stages of lymphedema before the destruction of lymphatic vessel smooth muscle and the development of irreversible tissue fibrosis.
- ▪
LVA may be more effective in addressing the upper extremity versus the lower extremity lymphedema.
- ▪
Vascularized lymph nodes can be harvested from numerous locations such as the groin, axilla, supraclavicular and submental regions. They can also be transferred to proximal (groin/axilla) or distal (wrist/ankle) areas of the affected limb.
- ▪
Harvest of vascularized lymph nodes should be performed carefully to prevent donor limb lymphedema.
- ▪
VLNT should be considered in patients who are poor candidates for LVA.
Introduction
Lymphedema involves the accumulation of lymphatic fluid leading to progressive fibrosis, fat hypertrophy and destruction of the lymphatic vessels. The course of lymphedema is chronic, progressive and debilitating. Although there is no cure, the gold standard for the treatment of lymphedema is manual decongestive lymphatic therapy (MDLT) or complete decongestive therapy (CDT), which is best administered by a certified lymphedema therapist. The use of these therapies, however, is labor intensive and requires strict lifelong patient compliance with compression garments. Surgical treatment of lymphedema follows after failure of such conservative measures. The indications for surgery are to reduce the weight of the affected region, to reduce frequency of infectious/inflammatory episodes, to prevent progression of lymphedema and/or to improve cosmesis and function.
Options for surgical treatment of lymphedema can be divided into two categories: excisional and physiologic treatment. Excisional treatment usually involves reductive procedures such as liposuction and excisional debulking with skin grafting (Charles procedure). Physiological treatment is aimed at restoring or reconstructing the physiologic drainage of the lymph fluid. Several different strategies to achieve this have been proposed, such as buried flaps, direct repair of lymphatics, bypass grafting of lymphatics, lymphaticovenular anastomosis (LVA), and vascularized lymph node transfers (VLNT). The outcomes of such procedures vary. The aim of this chapter is to present the overview of therapies that have been described and tested.
Excisional Treatment
Liposuction
The accumulation of lymphatic fluid in the limb results in increased deposition and hypertrophy of the adipose tissue. Liposuction, in which a fenestrated metallic cannula connected to a vacuum suction is used to aspirate subcutaneous fat, was originally developed for body contouring but since then has been used for the treatment of lymphedema. O’Brien et al. demonstrated an average 20–23% reduction using liposuction to treat a mixed cohort of patients who had not undergone previous surgeries to treat lymphedema. Brorson and Svensson compared the combined use of liposuction and compression therapy to therapy alone in stage II patients and demonstrated a 115% reduction in volume compared to 54% of patients who had isolated compression therapy. This was maintained at four years with average reduction of 106% (66–179%).
One of the theoretical risks of liposuction is further damage to existing lymphatic vessels. Cadaveric and imaging studies have shown that performing liposuction longitudinally to the limb minimizes this damage and that further impairment to already delayed transport of lymphatic fluid does not occur. In addition to volumetric reduction, functional improvement was also reported by Qi et al. when liposuction was combined with physiological treatments. The incidence of cellulitis (6.5 ± 4.3 vs. 0.7 ± 0.8 episodes/year) was drastically improved albeit confounded by the mixture of procedures performed.
In general, treatment of lymphedema with circumferential liposuction is considered safe with quick recovery within 48 hours. Complications are few and usually limited to minor wound healing problems and paresthesias. The use of tumescent technique during liposuction and tourniquets can greatly decrease the blood loss and need for transfusions.
While liposuction can aggressively debulk hypertrophied adipose tissue in a lymphedematous limb, the primary disadvantage of liposuction is the need for continuous (24-hour) use of compression garments postoperatively to maintain the new equilibrium. In the Brorson series, patients that discontinued use of compression garments rapidly re-accumulated fluid.
Direct Excision
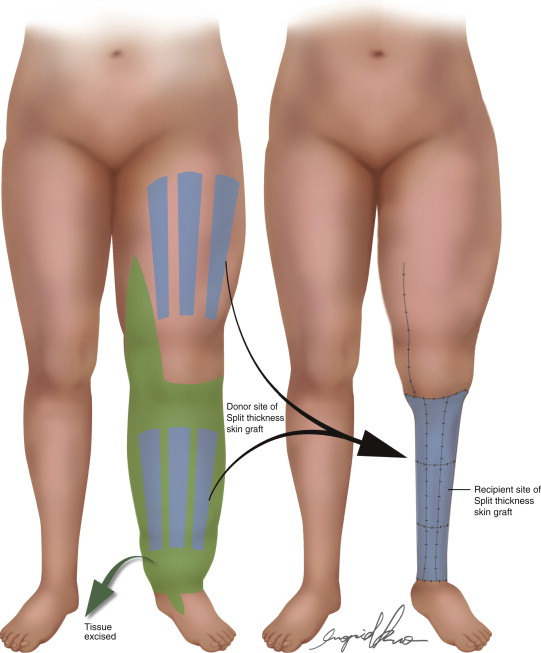
While largely of historical significance, direct excision with skin grafting is still reserved for severe cases of lymphedema. The procedure known as the ‘Charles procedure’ for treatment of lower extremity lymphedema is characterized by complete removal of skin and subcutaneous tissue with preservation of the deep fascia and sole of the foot, covered by skin graft harvested from the resected specimen ( Figure 10.1 ). While commonly credited to Charles, his original 1912 chapter on the treatment of scrotal lymphedema did not actually include any lower extremity cases. It was not until Macey and Poth that actual reports on treatment of the lower extremity with skin graft harvested from the specimen were described.
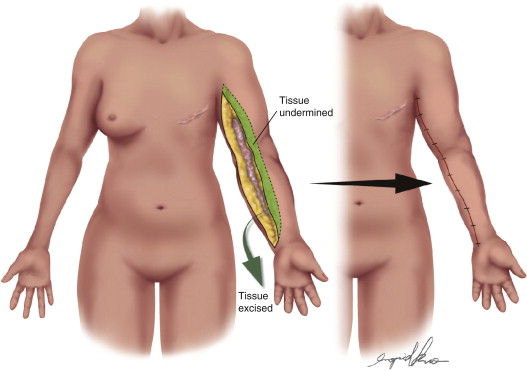
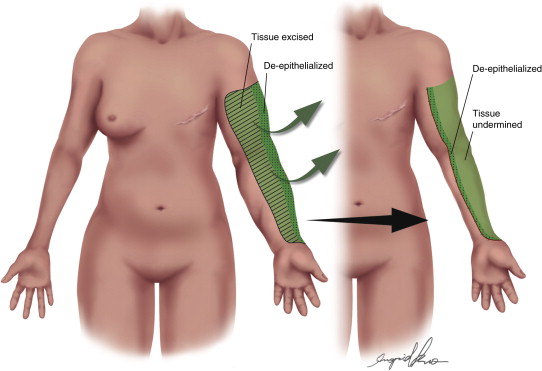
Subsequently, Sistrunk and Thompson sought to establish new pathways between the deep and superficial system. Sistrunk removed skin and soft tissue through an elliptical incision along the medial arm and wide excision of the deep fascia ( Figure 10.2 ). Thompson expanded this procedure by embedding the de-epithelialized skin flaps from the entire length of the elliptical incision along the neurovascular bundle ( Figure 10.3 ). The theory was based on spontaneous lymphangiogenesis from the superficial system to the deep system in order to provide shunting of lymph fluid. Although some have reported favorable results with these methods, there have been no objective data that demonstrates lymphangiogenesis via this approach.
Although some have advocated for the abandonment of such procedures, there are some cases of severe refractory lymphedema that have been successfully treated with radical excision and skin grafting. Undoubtedly, while this can be an effective way of reducing bulk and allowing function of some extremities, there are also significant risks. In addition to contour irregularities, scar, chronic foot infection and poor cosmesis, there are acute risks of infection, hematoma, blood loss requiring transfusions, and possible loss of skin grafts resulting in more surgery. Alternatively, staged elliptical excision of skin and subcutaneous tissue can also be performed to minimize morbidity or to address specific pockets of tissue. For some patients suffering with severe impairment of their activities of daily living (ADLs), recurrent infections, skin ulcerations, chronic pain and poor quality of life, radical excision may be their only, and possibly best, option for returning to function.
Physiological Treatment
Flap Interposition
The basis behind flap interposition is to place functioning lymphatic vessels contained within a segment of vascularized tissue into an affected area to siphon or bypass excess lymph fluid. In 1935, Gilles and Fraser were the first to treat lower extremity lymphedema by attaching a flap of skin and subcutaneous tissue from the arm to the leg and keeping the arm by the patient’s side. In the second stage, the flap was divided and the flap was transferred to the trunk. The theory was to use the flap from the arm to re-establish lymphatic flow and then to eventually bypass the groin region and restore lymphatic flow to the trunk.
Goldsmith et al. reported the use of greater omentum flaps to upper and lower extremity lymphedema. The greater omentum was pedicled off the ipsilateral gastroepiploic vessel and transferred to the extremity via a subcutaneous tunnel. The excess lymph fluid in the extremity was expected to drain into the abdominal lymphatic system through the rich network of lymph vessels in the greater omentum. In the series of 22 patients, 38% of lower extremity and 56% of upper extremity experienced good results. Despite this moderate improvement, the operation did not gain popularity due to the high incidence of complications including bowel obstruction, pulmonary embolus, and hernia.
Since then other authors reported small series using a variety of pedicled and free muscle and myocutaneous flaps (tensor fascia lata, deltopectoral, latissimus, serratus) for the treatment of extremity and head and neck lymphedema. No prospective or long-term studies have demonstrated the efficacy of these procedures and they remain anecdotal for the most part.
Lymphatic Bypass
Lymphatic-Lymphatic Bypass
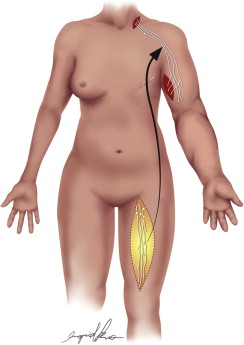
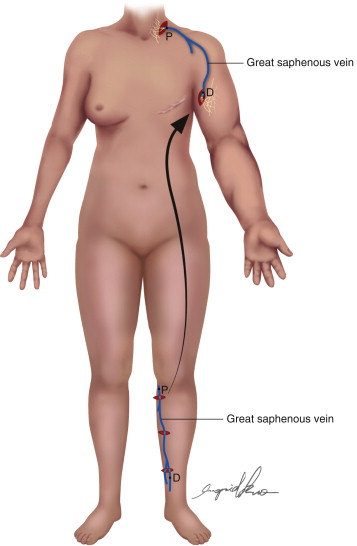
Some investigators have attempted to bypass fibrosed lymphatics by using lymphatic or vein grafts to link distal lymphatics to more proximal lymphatic channels. Baumeister and Suida attempted to bridge areas of stenosed lymphatic vessels with autologous lymphatic grafts in the upper and lower extremities. For the upper extremity, healthy lymphatic vessels from the medial thigh are harvested as a composite graft, and buried in a subcutaneous tunnel between the supraclavicular shoulder region and the upper arm ( Figure 10.4 ). The lymphatic vessels at either end are microscopically identified and anastomosed to the recipient lymphatics. To treat unilateral lower extremity lymphedema, the lymphatics of the graft spans across the affected thigh and the contralateral groin region. In 55 patients tested, there was an 80% reduction of volume at a three-year follow-up. The patency of the lymphatic grafts were tested with lymphoscintigraphy and demonstrated new lymphatic drainage patterns and 30% faster clearance of radioisotope than in preoperative images. Ho and colleagues performed similar procedures and noted that the microlymphatic bypass must be carried out before the lymphatics were permanently damaged by back pressure and recurrent infection. In addition to the drawback of long incisions at donor and recipient sites, the harvest of lymphatics from a functional extremity may predispose the donor extremity to lymphedema.
Alternatively, vein grafts have been used to perform distal to proximal lymphatic bypass. Campisi et al. reported a series of 39 patients using lymphatic-venous-lymphatic bypass in upper and lower extremities when lymphovenous bypass could not be performed. In their procedure, multiple distal lymphatic channels are sutured into the cut distal end of an autologous vein graft that provide a conduit to more proximal lymph vessels inserted into the other end of the vein graft ( Figure 10.5 ). Patients were followed for as long as five years demonstrating improvement in edema and function.
Lymphovenous Bypass (LVB) & Lymphovenous Anastomosis (LVA)
The final destination of lymphatic fluid in the lymph vessels is return to the venous system by way of the thoracic ducts. Lymphovenous bypass (LVB) attempts to return the lymphatic fluid to the venous system earlier along the pathway. A lymphovenous shunt was first described by Jacobson in 1962 in a canine model. This was followed by Yamada who first experimented in dogs before applying the technique in a series of patients with lower extremity lymphedema. In cases involving filariasis, Sedlacek described the use of end-to-side lymphovenous bypass using saphenous vein. While others also used the saphenous vein, concern over venous hypertension in larger caliber vessels resulted in attempts to bypass to venules. Yamada was the first to describe end-to-end anastomosis between a lymphatic and venule, hence lymphaticovenular anastomosis (LVA). The use of ‘supermicrosurgery’ to anastomose vessels less than 0.8 mm in diameter has recently gained popularity around the world.
Results of LVB have been favorable but measurements of outcomes have been difficult to standardize. In 1990, O’Brien et al. reported long-term follow-up on 90 patients some of whom received LVB-only and others who had LVB with adjunctive reductive procedures. In the cohort that received LVB-only, subjective improvement occurred in 73% of patients and objective improvement was documented in 42% of patients with an average 44% reduction in volume. At a four-year follow-up, 74% of patients were able to discontinue conservative treatment completely and the incidence of cellulitis decreased by 58%. Results with LVA operations have likewise been difficult to generalize with a wide range of results, differing follow-up times, variable postoperative therapy protocols, nonstandard volumetric measurements, and no metrics on patient outcomes. Subjective measures of improvement have ranged from 95% to 50% of patients. Variable volumetric improvements have ranged from a 75% decrease in 73% of patients to no change in 50% of patients, with an average reduction in volume of 55%. In the few studies that included incidence of cellulitis, most demonstrated a significant decrease after LVA/LVB. Finally, a portion of patients were able to completely discontinue use of compression garments even over long-term follow-up.
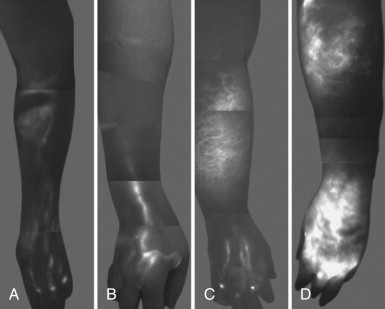
Recent technological advancements with fluorescence lymphography have provided surgeons with a much better ability to perform real-time identification and evaluation of existing lymphatics. Injection of indocyanine green (ICG) dye into the dermis and evaluation with near-infrared fluorescence lymphography immediately displays the severity of the process and location of vessels if present. Patients with early stage lymphedema have easily identifiable discrete lymphatic channels compared to patients with late stage lymphedema, which appears as a blush of dermal backflow ( Figure 10.6 ). Veins are identified as dark segments crossing over the visualized lymphatics which can then be marked and used to guide the LVB procedure. This improves operative efficiency and allows for limited dissection and morbidity to the patient, as well as a quicker recovery. The surgery is then performed using short horizontal incisions at the marked locations along the length of the extremity ( Figure 10.7 ). Dissection is performed at the superficial subcutaneous plane to locate a venule and lymphatic channel, confirmed with isosulfan blue or ICG lymphangiography, and the LVA is performed. After completion of the anastomosis, patency can be confirmed with isosulfan blue passing from the lymphatic to the venule, or with ICG lymphography ( Figure 10.8 ) ![]() ( ).
( ).
Related posts:
 An Introduction to Principles and Practice of Lymphedema Surgery
An Introduction to Principles and Practice of Lymphedema Surgery
 Clinical Evaluation of Lymphedema
Clinical Evaluation of Lymphedema
 Laboratory Study of Lymphedema
Laboratory Study of Lymphedema
 Recipient Site Selection in Vascularized Lymph Node Flap Transfer
Recipient Site Selection in Vascularized Lymph Node Flap Transfer
 Future Perspectives in Lymphatic Microsurgery
Future Perspectives in Lymphatic Microsurgery
 Microsurgical Procedures: Lymphovenous Anastomosis Techniques
Microsurgical Procedures: Lymphovenous Anastomosis Techniques
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


