Key Points
- ▪
A vascularized lymph node flap can be transferred to virtually any location on the extremities, but is usually transferred to the axilla, elbow, wrist, groin, knee, or ankle.
- ▪
Good results have been achieved with transfer to all of these recipient sites.
- ▪
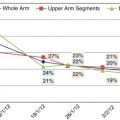
Transfer to the distal extremity (i.e., wrist or ankle) may be mechanistically advantageous and, in the case of upper limb lymphedema, has been shown to be superior to the elbow for the reduction of forearm circumference.
- ▪
Factors impacting the selection of a recipient site include relative severity of the lymphedema at various levels of the extremity, need for concomitant scar release at a given site, functional outcome, and aesthetic concerns.
- ▪
Dissection of recipient vessels in a lymphedematous limb can be extremely challenging, and meticulous technique and thorough anatomic knowledge are essential to minimize complications and optimize results.
Introduction
Vascularized lymph node flap transfer was described decades ago by a number of investigators, yet only recently has it ascended to the forefront of surgical treatments for lymphedema. As such, there are still many details of the procedure that are being and will continue to be investigated and explicated over time. Among these details is the selection of the optimal recipient site. Although data from the senior author’s group has shed some light on the question, different recipient sites continue to be utilized with success by various surgeons around the world. Fundamentally, the lymphedema surgeon must be very comfortable with the anatomy of the entire upper and lower extremity in order to apply the technique of vascularized lymph node transfer in its various forms, as indicated for a particular patient’s situation.
Concepts
Recipient Site Selection
While it would be technically feasible—and perhaps effective—to transfer a lymph node flap to virtually any location on the extremities, lymphedema surgeons typically choose from a few: axilla, elbow, wrist, groin, knee, or ankle. (Anatomic considerations for these sites will be discussed below in the Surgical Techniques section.) Why a given site is chosen may depend on several factors, including hydrostatic theory, relative severity of the lymphedema at various levels of the extremity, need for concomitant scar release at a given site, and aesthetic concerns.
Exactly how transferred lymph nodes function at the recipient site has, up to now, been poorly understood. Recently, studies from the senior author’s group have proven that the transferred nodal tissue has the ability to take up lymphatic fluid and shunt that fluid into the recipient vein. It is still not known exactly how the transferred nodal tissue takes up fluid, but it is logical to assume that the hydrostatic pressure in the interstitial space relative to the recipient venous pressure—i.e., the interstitial-venous pressure gradient—has some effect on the process. If so, it would be theoretically advantageous to transfer the nodes to the distal extremity (wrist or ankle), where gravity would create higher interstitial pressure. Published clinical data from the senior author’s group support this theory, in that outcomes of transfers to the wrist exceed those to the elbow in the treatment of postmastectomy upper limb lymphedema.
This theory notwithstanding, good results have been achieved with transfers to the proximal extremity, so clearly other factors can and should come into play when choosing a recipient site. For example, occasionally a patient will present with significant lymphedema of the upper arm but relatively mild lymphedema of the forearm and hand; in these cases it would probably be unnecessary to transfer the lymph nodes to the wrist. A more common example would be a patient who suffers from scar contracture of the axilla following axillary node dissection. These patients can benefit greatly from axillary scar release, which enhances the appeal of the axilla as a recipient site for vascularized lymph node flap transfer. In some cases, lymph nodes may be transferred conjointly with a lower abdominal flap for breast reconstruction; obviously the axilla would be the logical destination for these nodes.
Finally, aesthetic considerations may factor heavily in recipient site selection. Some patients may be displeased with the initial bulkiness of a lymph node flap at the wrist, in which case the inner elbow or axilla may be preferable. In reality, the flap can be debulked in a few months and made to be very inconspicuous, even at the wrist. Nonetheless, the patient would have to be willing to accept a temporarily awkward appearance if the wrist is chosen. Such aesthetic concerns are usually not as pressing for patients with lower limb lymphedema, typically making the ankle, with advantages both theoretic (mentioned above) and practical (discussed below), the recipient site of choice.
Patient Selection
Patient selection for lymphedema surgery is generally discussed in Chapter 10 : Overview of Surgical Techniques. Basically, the indications for vascularized lymph node flap transfer include:
- ▪
lymphedema severity of stage 2 or above on the International Society of Lymphology (ISL) scale
- ▪
total occlusion of lymphatics on lymphoscintigraphy
- ▪
partial occlusion of lymphatics on lymphoscintigraphy with poor response to physical therapy and more than two episodes of cellulitis in six months.
Contraindications include local recurrence, distant metastasis, and brachial plexus neuritis. Patients with ISL stage 3 or 4 may need adjunctive liposuction or a later debulking procedure once the fibrosis softens.
Preoperative Considerations
As with any free tissue transfer, it is important to have a reasonable assurance that the selected recipient site will have vessels suitable for microvascular anastomoses. Vascularized lymph node flaps typically contain a small volume of tissue and have a pedicle of fairly small caliber—usually 1–3 mm depending upon the site from which they are harvested, so in general the size and flow requirements of the recipient vessels are also fairly small. Extremity vessels of this caliber are sometimes not named, but rather are ‘vessels of opportunity’. Finding such vessels in an axilla or groin that has been dissected and/or radiated can be very challenging, in some cases diminishing the practicality of these recipient sites. Distally, it would obviously be important not to compromise flow to the hand or foot, but again, because the pedicle vessels are small, anastomoses are usually to small branches of the major arteries, rather than the major arteries themselves, or are end-to-side to the major arteries. This flexibility in artery selection and utilization means that preoperative arteriography is generally not needed, unless there is a unique history of trauma to the proposed site or significant peripheral vascular disease, in which case the patient may not be an acceptable candidate for the procedure. In contrast, the venous system in a lymphedematous limb can be affected by superficial or deep venous incompetency; duplex Doppler scanning can therefore be very helpful to predict and plan for this potential pitfall.
Surgical Techniques
Exposure of the various recipient vessels and related anatomic considerations will be covered in this section. (Please see Table 13.1 for a summary of the various recipient sites and their relative advantages and disadvantages.) Broadly speaking, it should be noted that vascular anatomy is often quite variable, so the surgeon must be comfortable dissecting a number of potential recipient vessels, as well as performing end-to-side anastomoses if a major artery must be used. Cutaneous nerves must be anticipated and protected throughout the dissection. Finally, in a lymphedematous limb the vascular adventitia is often thick and fibrotic, especially around the veins, so adventitiectomy should be cautiously performed to facilitate the anastomoses and optimize flow.
| Recipient Site | Potential Recipient Arteries | Potential Recipient Veins | Skin Paddle Required | Advantages | Disadvantages |
|---|---|---|---|---|---|
| Upper Limb | |||||
| Axilla | Subscapular; circumflex scapular; thoracodorsal; lateral thoracic; circumflex humeral | Comitant | No | Concomitant scar contracture release | Scarred bed |
| Elbow | Inferior ulnar collateral; anterior ulnar recurrent | Comitant; basilic | Yes | Unscarred bed | Less gravity effect |
| Wrist | Dorsal branch of radial; ulnar | Comitant; cephalic | Yes | Gravity effect | Aesthetic |
| Lower Limb | |||||
| Groin | Superficial inferior epigastric; superficial circumflex iliac; deep inferior epigastric | Comitant | No | Concomitant scar contracture release | Scarred bed |
| Knee | Medial sural; descending genicular | Comitant; great saphenous | Yes | Unscarred bed | Patient positioning; less gravity effect |
| Ankle | Anterior tibial; posterior tibial | Comitant; greater or lesser saphenous | Yes | Gravity effect | Aesthetic |
Axilla
As stated earlier, the axilla is often selected in patients who suffer from symptomatic scar contracture due to prior axillary node dissection and/or radiation. Although dissection through this scar tissue is very difficult and potentially endangers vital structures, excisional release of this scar tissue, in and of itself, can greatly benefit the patient, and also provides enough room for the flap such that a skin paddle is often not necessary (i.e., the vascularized lymph nodes can be buried). If no prior scar exists, or if it needs to be extended, a longitudinal skin incision along the inside of the anterior axillary fold is inconspicuous and does not typically cause an adduction contracture. There are several potential recipient arteries in the axillary region, and oftentimes the surgeon will encounter an artery of suitable caliber during excision of axillary scar tissue. Main branches of the distal axillary artery include the subscapular artery, which arises medially at the lateral border of the scapula, and the circumflex humeral arteries, which arise laterally near the humeral neck. The branches of the subscapular artery—the circumflex scapular and thoracodorsal arteries—are frequently targeted ( Figure 13.1 ). It is sometimes easiest to identify the thoracodorsal artery along the deep lateral margin of the latissimus muscle and trace it proximally toward the axilla. If these vessels are scarred or otherwise unsuitable, branches of the circumflex humeral arteries or the muscular branches of the proximal brachial artery can be dissected, again beginning in relatively unscarred tissue at the distal axilla and dissecting proximally. The lateral thoracic artery, passing along the lateral border of the pectoralis minor muscle, is another possibility. Suitable veins typically accompany any of these arteries, and other adequate, unnamed veins are occasionally encountered during the dissection. If dissection must proceed deep into the axilla, microvascular anastomoses can be technically awkward, and so the use of vein grafts may need to be considered.