Otoplasty
Charles H. Thorne
This chapter reviews otoplasty for common auricular deformities such as prominent ears, macrotia, ears with inadequate helical rim, constricted ear, Stahl’s ear, question mark ear, and cryptotia.
PROMINENT EARS
The term prominent ears refers to ears that, regardless of size, “stick out” enough to appear abnormal. When referring to the front surface of the ear, the terms front, lateral surface, and anterior surface are used interchangeably. Similarly, when referring to the back of the auricle, the terms back, medial surface, and posterior surface are used synonymously. The normal external ear is separated by less than 2 cm from, and forms an angle of less than 25° with, the side of the head. Beyond these approximate normal limits, the ear appears prominent when viewed from either the front or the back. While these measurements provide a guideline, aesthetic judgment is more important. In 25 years of dealing with auricular deformities, the author has never measured either the angle with the skull or the distance from the side of the head.
To correct prominent ears, the anatomic abnormality is determined (Figure 49.1). The three most common causes of prominent ears are the following and are usually present in combination:
Underdeveloped antihelical fold. As a result of inadequate folding of the antihelix, the scapha and helical rim protrude. This anatomic abnormality causes prominence of the upper third and, in many cases, the middle third of the ear.
Prominent concha. The concha may be excessively deep, the concha/mastoid angle may be excessive, or there may be a combination of these two factors. This anatomic abnormality causes prominence of the middle third of the auricle.
Protruding earlobe. The protruding earlobe causes prominence of the lower third of the ear.
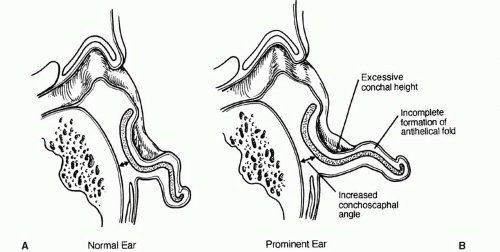
FIGURE 49.1. Comparison of normal and prominent ear anatomy. A. Normal ear. B. Components of the prominent ear. (Reproduced with permission of Charles H. Thorne, MD. Copyright Charles H. Thorne, MD.)
Although most prominent ears are otherwise normal in shape, some prominent ears have additional deformities. The conditions enumerated below are examples of abnormally shaped ears that may also be prominent. The term macrotia refers to excessively large ears that, in addition to being large, may be “prominent.” The average 10-year-old male has ears that are 6 cm in length. Most adults, men and women, have ears in the 6 to 6.5 cm range. In men, ears that are 7 cm or more will look large. In women, ears may look large even if significantly less than 7 cm. Ears with inadequate helical rims or shell ears are those with flat rather than curled helical rims. Constricted ears (Figure 49.2) are abnormally small but tend to appear “prominent” because the circumference of the helical rim is inadequate, causing the auricle to cup forward. The Stahl’s ear deformity (Figure 49.3) consists of a third crus, in addition to the normal crura of the triangular fossa, which traverses the scapha. This may give the ear a “Mr. Spock” pointed appearance in addition to being prominent. Question mark ears earn their name because deficiency of the supralobular region gives the ear the shape of a question mark. The upper portion of the auricle tends to be large and may be prominent as well. Cryptotia (Figure 49.4) describes the auricle in which the upper pole of the helix is buried beneath the temporal skin. Cryptotic ears are not prominent.
Goals of Otoplasty
The goal of otoplasty is to set back the ears in such a way that the contours appear soft and natural, there is no evidence of surgical intervention, and the setback is harmonious: that is, each portion of the ear appears in appropriate position relative to the rest of the auricle. When examined from the various angles, the corrected auricle should have the following characteristics:
1. Front view. When viewed from the front the helical rim should be visible, not set back so far that it is hidden behind the antihelical fold.
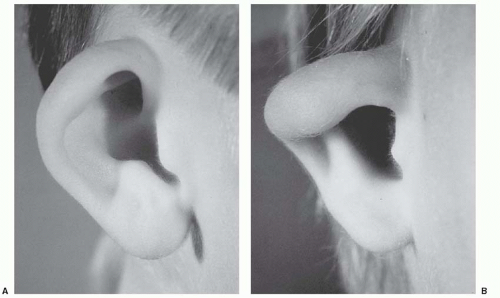
FIGURE 49.2. Constricted ear. A. Mildly constricted ear. Otoplasty requires increasing the circumference of the helical rim by advancing the crus of the helix into the helical rim (see Figure 49.7). B. Severely constricted ear. This degree of constriction can only be repaired by discarding some of the cartilage and performing an ear reconstruction as in microtia. (Courtesy of David Furnas, MD.)
Rear view. When viewed from behind, the helical rim should be straight, not bent like a “C” or a “hockey stick.” If the helical rim is straight, the setback will be harmonious; that is, the upper, middle, and lower thirds of the ear will be set back in correct proportion to each other. If, for example, the middle third is set back too much relative to the upper and lower thirds, the helical rim will form a “C” when viewed from behind, creating the so-called telephone deformity. Similarly, if the earlobe is insufficiently set back, the rear view will reveal a hockey stick appearance to the helical rim contour.
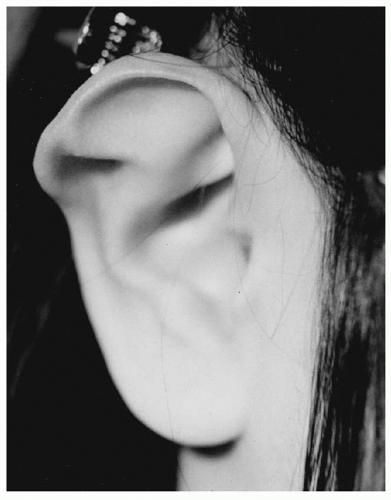
FIGURE 49.3. Stahl’s ear. Note the third crus that traverses the scapha. (Courtesy of David Furnas, MD.)
Lateral view. The contours should be soft and natural, not sharp and “human-made.”
Timing of Otoplasty
There is no absolute rule about when otoplasty should be performed. In young children with extremely prominent ears, a reasonable age is approximately 4 years. In cases of macrotia associated with prominence, the author has performed the procedure as early as age 2 years, thinking that any restriction of growth is an advantage. Regardless of the exact age, the procedure requires general anesthesia. In other cases, usually more minor, the parents may choose to wait until the child can participate in the decision. This may allow the procedure to be performed under local anesthesia, although it is a rare child that can tolerate local anesthesia before age 10 years, and many not until they are adults.
Operative Procedure
Numerous methods have been described for correcting the anatomic abnormalities described above. The techniques that have stood the test of time are the simplest, most reliable, and least likely to cause complications or an “operated” look. The techniques described below are used alone or in combination depending on the anatomic deformity and the choice of the surgeon.
Antihelical Fold Manipulation.
Suturing of cartilage. Mattress sutures are placed from the scapha to the triangular fossa or concha, as described by Mustarde,1 and are tied with sufficient tension to increase the definition of the antihelical fold, thereby setting back the helical rim and scapha (Figure 49.5).
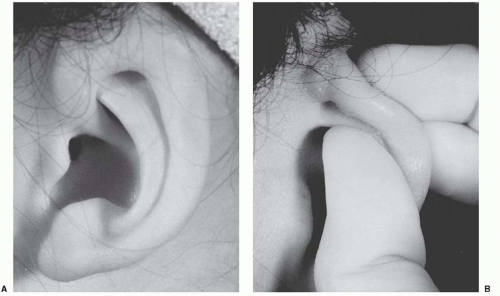
FIGURE 49.4. Cryptotia. A. Patient in whom a relatively normal helical rim is buried in the temporal soft tissues. The upper portion of the auricle can be exposed by outward traction on the ear. B. Outward traction (in a different patient) causes the upper portion of the ear to emerge from its hiding place. (Courtesy of David Furnas, MD.)
Stenstrom technique of anterior abrasion.2 The anterior surface of the antihelical fold cartilage is abraded, causing the cartilage to bend away from the abraded side (principle of Gibson) toward the side of intact perichondrium (Figure 49.6).
Full-thickness incisions. A single full-thickness incision along the desired curvature of the antihelix permits folding with slight force, creating an antihelical fold (Luckett procedure). Because the fold is sharp and unnatural appearing, this single-incision technique was modified. In the Converse/Wood-Smith technique,3 a pair of incisions is made, parallel to the desired antihelical fold, and tubing sutures are placed to create a more defined fold.
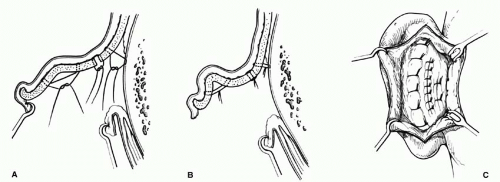
FIGURE 49.5. Otoplasty technique: The combination of a Mustarde scapha-conchal suture, conchal resection with primary closure, and a Furnas conchal-mastoid suture. Note that the conchal closure is at the junction of the floor and posterior wall of the concha. A. Sutures placed. B. Sutures tightened to create the desired contour. C. Same sutures as seen through the retroauricular incision. (Reproduced with permission of Charles H. Thorne, MD. Copyright Charles H. Thorne, MD.)Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access






