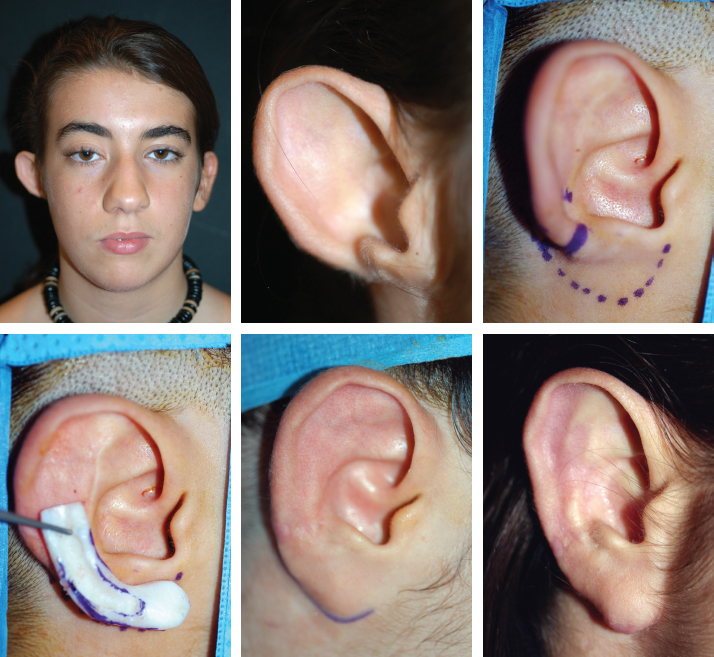
CHAPTER 15 The structure of the lobule comprises skin, fat, and fibrous septa without fibrocartilage. This is why the lobule is often reconstructed with skin flaps. In our experience skin alone cannot correctly reproduce the shape of the lobule, and flaps raised from around the lobule leave visible scars. To re-create a missing lobule, there must be an adequate support, which will be covered with local skin. Fig. 15-1 This case shows our technique of assessing skin laxity with skin hooks. Skin laxity was adequate to allow reconstruction of the lobule with fibrocartilaginous support harvested from the contralateral conchal bowl. In some cases the conchal graft is taken from the same side. The entire concha (except the root of the helix) is harvested, and because it is usually too large for just the lobule, the excess is used to reinforce the graft with one or two planes of fibrocartilage, as performed in the following case. Fig. 15-2 The redundant skin from the lobule was excised, and the incision was used as a skin approach to dissect a skin pocket for insertion of a conchal graft. The patient requested a piercing, and this was performed through the fibrocartilage. This had the additional advantage of helping to stabilize the graft. Fig. 15-3 A cleft lobule is a common anomaly, and in our experience it is best treated by transposition of the flaps. It is not a Z-plasty but an anterior transposition of a triangular flap from the cleft and is inserted into an anterior portion of the lobule. The shape of the lobule must be created by a conchal graft inserted into the skin pocket underlying the flap. Fig. 15-4 This young man presented with obvious hypertrophy and prominence of the lobule, which is evident from the frontal view. It was reduced with our typical marginal incision, and transversely with an anterior wedge to correct its projection and implantation. Fig. 15-5 The missing lobule was associated with a prominent ear mostly because of the absence of antihelix plication. It could only be reconstructed with a costal cartilage graft. This could have been done in the same stage as correction of the upper part of the ear, but the patient decided to postpone the reconstruction of the lobule. The upper part was corrected with a posterior approach and thinning the fibrocartilage to perform plication reproducing the antihelix and its two roots. The lobule was reconstructed in two stages, with a small framework of rib cartilage reproducing the missing contours inserted into a skin pocket in the first stage. A full-thickness skin graft from the contralateral sulcus was used for elevation of the lobule in the second stage. The anomalous posterior root of the antihelix lies perpendicular to the anterior root of the antihelix. Surgeons must analyze the anomaly, particularly to check if it can be reduced by a simple maneuver. We simply attempt to fold the fibrocartilage between our thumb and index finger, and based on the amount of resistance, we plan our surgical approach. During the consultation different surgical approaches are determined, depending on our ability to easily reduce the deformity.
Other Anomalies
LOBULE
Good Skin Potential

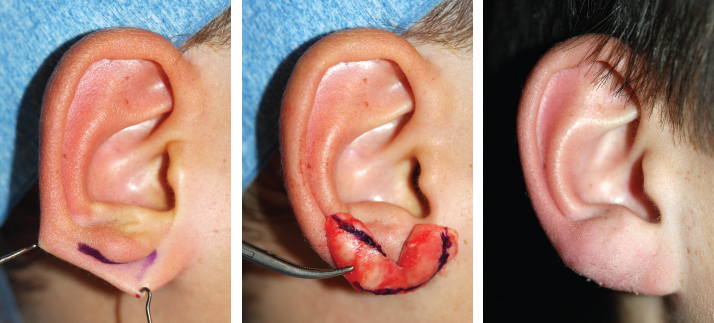
Cleft Lobule

Hypertrophic Lobule

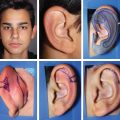
Absent Lobule Anomaly
POSTERIOR ROOT OF THE ANTIHELIX (STAHL)
Removal of the Posterior Root and Reduction of the Helix
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine