Key points
• Prosthodontics is the art and science of the aesthetic and functional restoration of the hard and soft tissues of the oral cavity.
• Osseointegration is arguably the most significant contribution to prosthetic dentistry and has become a routine consideration in any dental treatment plan that involves tooth replacement.
• Because it is rare to see the mandibular dental midline at a social distance, it is less important to have this coincide with the maxillary midline.
• Teeth with rounded incisal edges give a more youthful appearance, whereas flat incisal edges give the appearance of wear and advanced age.
• When the vertical dimension of occlusion is deficient, the mandible overcloses and rotates forward creating a “witch’s chin” and an aged appearance. An increase of occlusal vertical dimension with restored dentition will improve facial aesthetics.
• The position and angulation of the implant will determine the aesthetic outcome of the restoration.
• Osseointegrated implants will always decidedly improve the outcome of a prosthesis, whether removable or fixed, with respect to support, stability, retention, function, and aesthetics.
• A surgical guide should be used to ensure the most accurate implant placement, which, in turn, will yield the most aesthetic restoration.
Introduction
According to the Greek philosopher Plato, “beauty lies in the eye of the beholder.” Although this may be true, there are certain aspects of beauty that are universally accepted. Numerous scientific publications have addressed the topic “facial aesthetics.” Manufacturers and practitioners alike spend considerable time and money developing, advertising, and making use of products and techniques directed to this end. The public, in turn, spends considerable resources availing themselves of these—all in the pursuit of facial beauty.
There are established norms of proportion, shape, size, and orientation that guide surgeons in their pursuit of aesthetic facial outcomes, and a number of chapters of this book specifically address these from multiple perspectives. This chapter will focus on the prosthodontic consideration when utilizing osseointegration to optimize facial aesthetics.
Prosthodontics is the dental specialty pertaining to the diagnosis, treatment planning, rehabilitation, and maintenance of the oral function, comfort, appearance, and health of patients with clinical conditions associated with missing or deficient teeth and/or maxillofacial tissues with the use of biocompatible substitutes. More simply stated, it is the art and science of the aesthetic and functional restoration of the hard and soft tissues of the oral cavity. These tissues may be missing due to a congenital condition, dental caries, periodontal disease, ablative surgery, or trauma. Rehabilitation may be performed by using autogenous, allogeneic, or alloplastic materials or a combination of these. Most directly, it is the “aesthetic zone” that it impacted. This is the area of teeth, gingivae, mucosa, and lips. Outcomes in this critical region will certainly affect the entire facial appearance.
A healthy smile is an integral part of facial aesthetics. It not only affects one’s psychologic and emotional well-being but also has a functional, physical, and health-related component. To achieve success in this area, a team approach should to be employed. The aesthetics team should include a plastic and reconstructive surgeon and a prosthodontist but may also include other dental specialists, such as an orthodontist and a periodontist, to address all aesthetic concerns, such as the oral soft tissues and natural tooth alignment and position. It is also important that the patient be considered as part of the team because his or her input is valuable. Each smile and the related facial aesthetics are as unique as each individual.
Osseointegration and facial aesthetic
Osseointegration refers to a “direct structural and functional connection between ordered, living bone and the surface of a load-carrying implant.” This phenomenon was first described by Dr. P-I. Brånemark in 1985 in his landmark textbook Tissue-Integrated Prostheses. Although implants had been used in dentistry for many years, it was Brånemark’s work that brought science and evidence-based predictability to dental implantology. Since its introduction to clinical care, the use of dental implants has expanded exponentially. It is arguably the most significant contribution to the art and science of prosthetic dentistry and has become a routine consideration in any dental treatment plan that involves tooth replacement. As of January 2016, more than 100 manufacturers of dental implants exist.
The initial application of osseointegrated implants was in the anterior mandible as a way of resolving the age-old problem of an unstable removable complete denture. In short order, applications were expanded to the maxilla to address not only missing complete dentition but partially edentulous areas as well. The use of osseointegrated implants has greatly improved the ability to restore facial aesthetics and normal function in the presence of tooth loss.
Although the technical aspect of placing an implant into bone is fairly straightforward, it is the planning of the placement of the implant and its restoration that determines the aesthetic outcome. As is true of so many procedures, the care, skill, judgment, and experience of the operator are critical. Equally true of osseointegration and facial aesthetics, as of reconstructive surgery in general, the more the structures missing and needing replacement, the more challenging it is to achieve an ideal aesthetic outcome. A cardinal rule of implant placement is that there must be adequate bone volume at an edentulous site to place the implant and achieve initial stability.
The aesthetic zone
Many articles in the dental literature address tooth appearance, the smile, and the “aesthetic zone” as they relate to facial aesthetics. This zone takes into consideration the position and appearance of the maxillary anterior teeth, their periodontal hard and soft tissues, the incisal and middle thirds of the mandibular anterior teeth, and the upper and lower lip positions and contours ( Fig. 31.1 ).

When restoring the aesthetic zone to complement and enhance facial aesthetics, the following points need to be considered. The degree to which each is employed will depend on the extent of the rehabilitation that is required. All of these points contribute to an aesthetic dentition, which, in turn, affects facial aesthetics. These points related to an aesthetic smile whether restored with natural dentition or an implant prosthesis:
- 1.
The midline of the maxillary dentition
- 2.
The individual tooth characteristics: the length, size, shape, contour, position, alignment, surface texture, and color of an individual tooth
- 3.
The smile line
- 4.
The tooth and the dentogingival display at rest, while speaking, and during casual and wide smiles
- 5.
The levels of the margins of the gingival soft tissue
- 6.
The health of the periodontal tissues
- 7.
The vertical dimension of the facial height and facial profile
- 8.
Contour of the lips and adjacent perioral soft tissue
The midline of the maxillary dentition
The midline of the maxillary dentition should coincide with the midfacial plane. Because it is rare to see the mandibular dental midline at a social distance, it is less important to have this coincide with the maxillary one. In cases of facial asymmetry, either congenital or acquired, a convenient guide for establishing the midfacial plane is to use the midpoint of a horizontal line between the oral commissures during a wide smile. If the position or alignment of the nose or eyes is severely asymmetrical, then an average point for the maxillary midline may be determined by viewing the patient at a social distance.
The individual tooth characteristics
The length, size, shape, contour, position, alignment, surface texture, and color of a tooth all impact the aesthetic outcome. Everyone wants teeth that are white and straight. Of course, “white” is a relative term, but prosthetic tooth color (hue, chroma, value) should blend with the surrounding natural teeth. In addition, tooth whitening, ceramic veneers and crowns, orthodontics, and periodontal surgery may all contribute to achieving an attractive smile.
The width of the maxillary anterior teeth measured from the distal of the canines is slightly wider than the width of the alar base. The central incisors are slightly more prominent than the other anterior teeth, and their length should approximate the wet–dry line of the lower lip during a wide smile and when making fricative sounds. On a wide smile, the upper lip should approximate the gingival margin of the maxillary teeth, with only a minimal display of gingival tissue, and the incisal edges of the maxillary anterior teeth should follow the smile line that is dictated by the position of the lower lip. The “negative image” is the silhouette made by the incisal edges of the maxillary anterior teeth. This should be slightly uneven with defined incisal embrasures to individualize the appearance of teeth. Teeth with rounded incisal edges give a more youthful appearance, whereas flat incisal edges give the appearance of wear and advanced age.
Surface texture of the facial surface of a tooth adds dimensionality. The multiple planes of light reflectance makes a tooth appear more natural, whereas a flat surface gives a more artificial appearance.
The margin of the gingiva of a tooth
The margin of the gingiva of a tooth should be symmetrical and even with its counterpart on the opposite side of the midline. The gingival margins of central incisors and canines are nearly even, and those of the lateral incisors are positioned slightly more incisal. The absence of a dental papilla leaving a dark space between teeth at the gum line is not only visually distracting but may also become a food trap. In cases of trauma, tumor resection, or cleft habilitation it may be difficult to surgically establish an ideal gingival margin and an interdental papilla, and these may need to be created as part of the prosthesis. Fortunately, in many cases, the wide smile does not display these areas and expose the gingival margin irregularities.
The gingival margin follows the cementoenamel junction of the tooth, and there is a straight or slight concave surface to the tooth as it exits soft tissue and extends into the mouth. This is known as the emergence profile . This tooth contour is particularly important to mimic with an osseointegrated implant prosthesis to achieve a realistic and aesthetic appearance at the gingival margin.
The health of the periodontal tissues
The health of the periodontal tissues has an aesthetic as well as functional component. Inflammation and bleeding of gum tissues not only creates an aesthetic compromise but also is a possible indicator of more serious conditions, such as bone loss, which may affect the long-term health of a tooth. Even if an implant-supported tooth restoration blends perfectly with the adjacent dentition, inflammation of soft tissues will detract from the appearance. Good oral hygiene practices are as important for implanted teeth as for natural dentition to prevent periimplantitis and tooth or implant loss.
Shortened vertical face height
A shortened vertical face height creates a “collapsed” facial profile and an appearance of aging. In completely edentulous individuals, the mandible overcloses and rotates forward creating a “witch’s chin” and an aged appearance. An increase of occlusal vertical dimension with restored dentition will improve facial aesthetics. At the same time, this increase must not be excessive, or function and comfort will be affected.
The lips and the adjacent perioral tissues
The dentition also has an impact on the appearance of the lips and the adjacent perioral tissues. Proper lip support from the dentition should not create an overly full or “puffy” appearance around the mouth. The red portion of the upper lip should be fully visible. The presence of a high smile line will pose more of an aesthetic challenge because more of the tooth and gingiva will be displayed.
Single tooth replacement and aesthetic considerations
In situations of single tooth loss, such as tooth loss due to dental caries or periodontal disease, the aesthetic outcome is more predictable. At the time of tooth extraction, if adequate bone is present, the implant may be placed immediately. Use of a provisional or definitive tooth restoration (known as immediate loading ) may be done to shape the surrounding soft issue and guide the aesthetics as healing progresses. Placement of a restoration at this time helps guide the ultimate shape of soft tissue and the final aesthetic outcome. Alternatively, the contour and appearance of the edentulous site may preserved by grafting bone (autogenous or allogeneic) for a deferred implant placement in 4 to 6 months followed by immediate or deferred placement of the restoration. The aesthetic outcome in these situations may be well managed as the addition of bone, the position of the implant, and the preservation of the gingival margin and interdental papillae may be planned and controlled. If adjacent teeth are extracted at the same time, preservation of the alveolar ridge contour, interdental papillae, and soft tissue appearance become a greater challenge.
There is little agreement, and even less scientific evidence, with regard to the ideal source for the graft when bone grafting is required before implant placement. The literature describes both autogenous bone and allogeneic bone as graft materials for these sites. Intraoral donor sites that will yield adequate bone include the mentalis area, the ascending ramus, and the tuberosity. Common donor sites outside of the mouth are the iliac crest or the cranium. Numerous allogeneic bone products have been described for such use. These may be osteogenic, osteoinductive, or osteoconductive in nature. Some reports even describe combining these with autogenous bone.
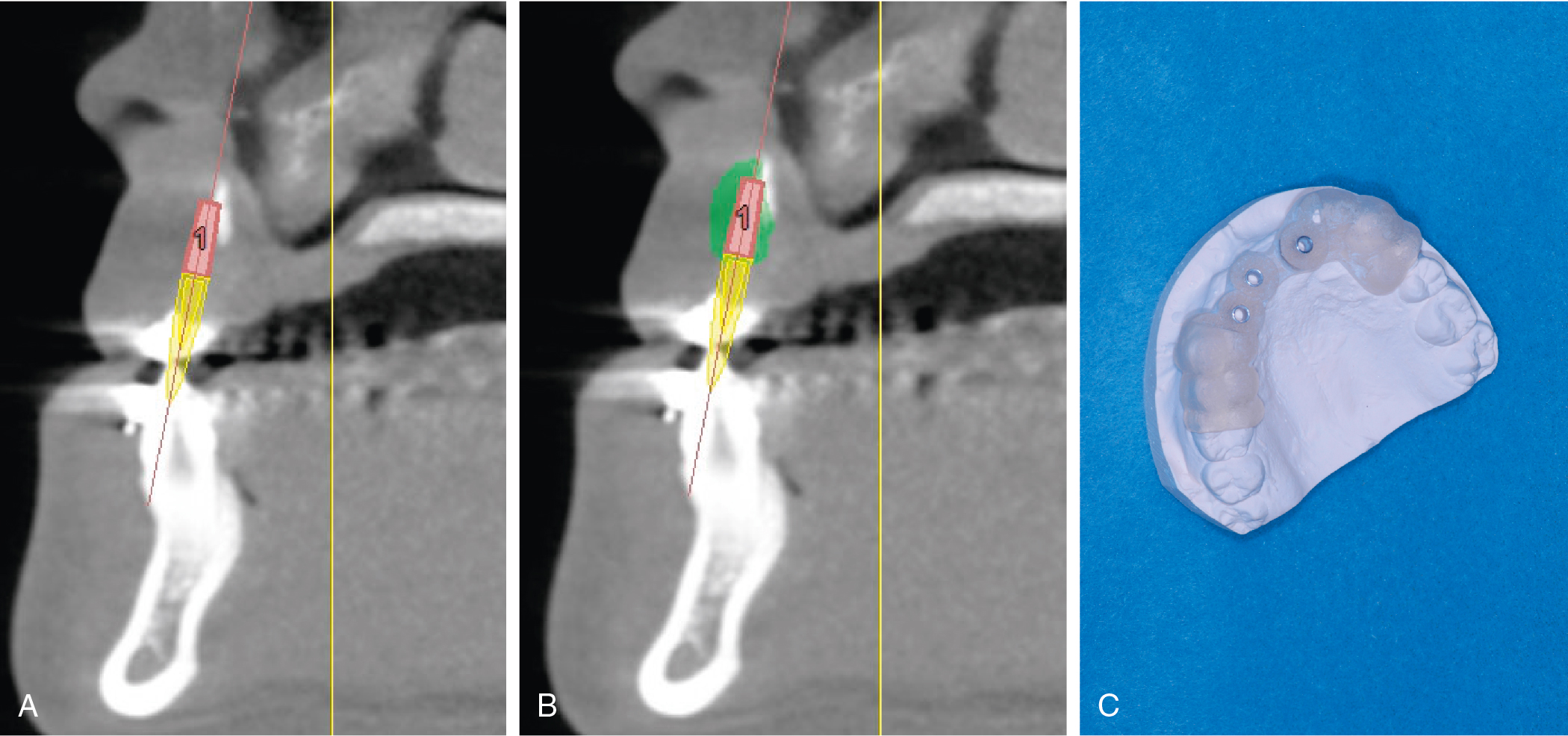
In cases of bone grafting and implant placement or implant placement alone, presurgical planning is crucial to success. The position and angulation of the implant will determine the aesthetic outcome of the restoration. The location and volume of a bone graft may be planned and verified with cone beam computed tomography (CBCT) and computer software. The position of the implant may likewise be plotted by using the same software, and a computer-generated intraoperative surgical guide for implant placement may be fabricated ( Fig. 31.2 A–C). This technique is used with placement of single or multiple implants to ensure accuracy.