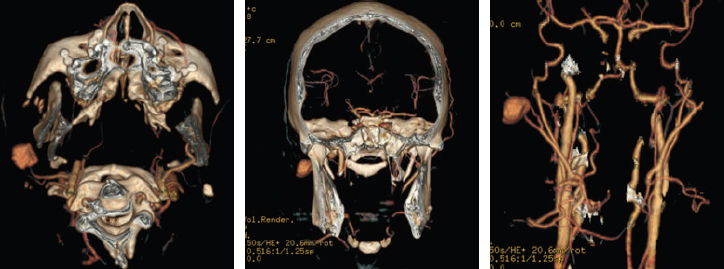
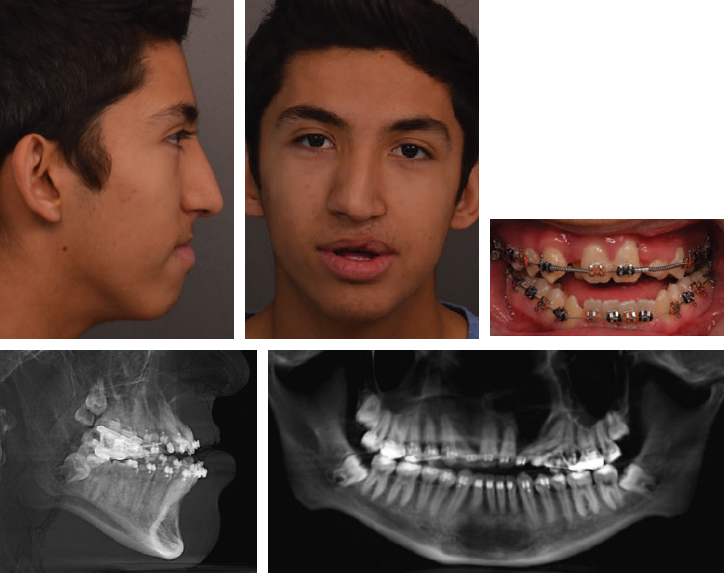
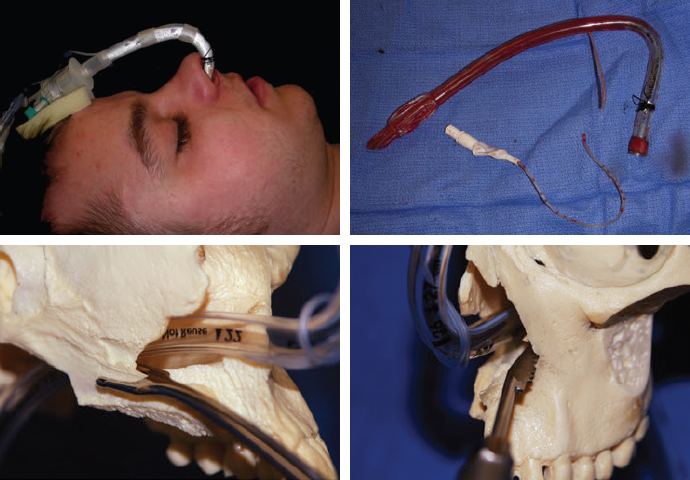
CHAPTER Orthognathic surgery involves the surgical manipulation of the elements of the facial skeleton to restore the normal anatomic and functional relationship in patients with anomalies of the dentofacial skeleton. Since its evolution from the mid-20th century with its classic procedures to the incorporation of distraction, osteogenesis has become a powerful tool in the surgeon’s armamentarium that can create dramatic changes in facial form and function that few other procedures can achieve. Achieving this desired goal involves a detailed architectural blueprint and construction details. Furthermore, it requires a close working relationship between the orthodontist and the surgeon, each manipulating their own component of the dentofacial unit in a complementary, time-specified, integrated approach. Speech and language pathologists and psychologists play an important role in guiding the treatment planning. As an elective procedure, orthognathic surgery places significant demands on patients and their families—with an overall length of treatment that spans years—in the form of financial resources and a multitude of appointments that require time off from employment and educational activities beyond the brief period of surgery and its immediate recovery. It is a significant commitment from the patient, caregivers, and professionals. Thus, practitioners must clearly define the surgical and dental goals and then concisely translate those goals to the patient and the family, including a discussion regarding why those goals may not be reached. The probable is what usually happens, but at this point the focus should be on the improbable, the unintended, and the unexpected. Thus understanding the unfavorable outcomes and surgical and orthodontic complications that can and do occur with maxillofacial skeletal procedures is the subject of this chapter. There is a relevant distinction between the “unfavorable” and the “complication.” An unfavorable outcome can occur without a specific complication, and not all complications lead to an unfavorable outcome. A perfectly well-executed orthognathic procedure from blueprint to construction without any complications can still lead to an unfavorable or unsatisfactory outcome. A face with a perfect occlusal and functional result may not be pleasing to either its owner or to the architects who designed it. Moreover, unlike many surgical procedures, the outcome depends not only on the surgical procedure itself, but also on a multitude of factors that exist long before the actual surgery, as well as on the ability to control variables long after the surgical procedure has taken place. Whether the desired long-term outcome is achieved in terms of occlusal function and aesthetics of the dental and facial form depends on whether the goals of each of the phases of treatment were achieved. Moreover, the success of each phase depends on the preceding phase of treatment. For example, inadequate incisor decompensation limits the amount of sagittal repositioning possible and compromises the final facial aesthetics. If mobilization of the maxilla at the time of surgery is inadequate and a less-than-ideal occlusal relation obtained, the postsurgical orthodontic phase is prolonged, and relapse toward the initial condition is likely to occur. Even when facial skeletal and dental goals are achieved, the functional goals may not be. Moreover, unintended consequences may occur in terms of velopharyngeal insufficiency, airway compromise, or oromotor function while optimizing facial appearance. Each orthognathic case has a stepwise sequence of diagnosis, dentosurgical treatment planning, presurgical orthodontic preparation, surgery, postsurgical orthodontic detailing, and retention. Thus, unlike many of the surgical procedures, the scale of time is not measured in weeks to months; rather, it is measured in years. The surgical component must be taken within the context of the overall treatment from diagnosis to retention. Within this lengthy time frame of a complex choreography between orthodontist and surgeon, errors occur and accumulate. The list of errors that can lead to unfavorable outcomes and complications is extensive and is well reviewed in the existing literature.1–5 A meaningful way to discuss these is to consider what can go wrong with each phase of treatment (see the Summary Box). Unfavorable outcomes occur primarily because of poor communication between the surgeon and the orthodontist and the patient6,7 (Fig. 43.1). For the vast majority, patients are referred to the surgeon by the orthodontist, whose goal is primarily to achieve occlusion that cannot be achieved without the aid of the surgeon. The surgeon assesses the patient from the perspective of optimizing the aesthetic goals of the soft tissue draping the skeletal framework within the context of achieving the orthodontist’s expected occlusion (Fig. 43.2). Each must understand the other’s objective and abilities to achieve those goals within any limitations or compromises that may occur when reaching common surgical and occlusal goals. Moreover, anatomic dentosurgical goals may negatively affect functional goals. An example is a patient with a severe class III cleft in whom a maxillary advancement procedure may put the patient at risk for velopharyngeal incompetence (VPI) while improving the anterior dental relationship, the aesthetic appearance, and speech articulation. A mandibular setback procedure used to minimize VPI may put the patient at risk for obstructive sleep apnea and a less-than-ideal facial appearance. Thus the goals of the speech and language pathologist and sleep medicine specialist may come into play. In many cleft patients, the lateral incisor is not present, and incorporating the need for either prosthodontic consideration or segmental closure with a canine-to-lateral substitution needs to be addressed from the beginning. It is more than simply filling a dental gap, because each approach will have a different outcome in perioral aesthetics of the arch form and smile. In a patient with a class II cleft in whom significant mandibular advancement would improve both aesthetic appearance and airway, the surgeon’s goal may be limited by insufficient dental decompensation that could have been achieved with mandibular first molar extractions and retraction of the anterior dentition. A bimaxillary advancement procedure could surgically compensate for improving the airway, but at the expense of the facial aesthetics. Summary Box Causes of Complications and Unfavorable Outcomes Errors in Diagnosis and Treatment Planning • Unrealistic expectations • Lack of understanding of the complexity of the procedure • Lack of teamwork between the orthodontist and the surgeon • Failure of including speech, psychology, and sleep medicine • Wrong diagnosis • Errors in diagnostic setup Errors in Preoperative Orthodontic Management • Inappropriate timing of intervention • Inadequate orthodontic setup • Insufficient decompensation • Inadequate transverse width coordination • Inadequate root divergence for segmentation • Inappropriate extraction versus nonextraction Complications in Operative Phase of Management • Errors in surgical planning • Intraoperative complications (see Box 43-1) Errors in Postoperative Orthodontic Management • Insufficient coordination of the dental arches • Inadequate postoperative posterior buccal-lingual torque • Failure of retention Unsatisfactory Outcome • Velopharyngeal insufficiency • Issues related to hardware • Chronic maxillary sinusitis • Osteotomy nonunion • Late malocclusion and relapse • Unsatisfactory facial appearance • Unacceptable nasal appearance and breathing • Unsatisfactory smile and perioral aesthetics • Issues related to temporomandibular joint Fig. 43.2 This patient was referred “ready for jaw surgery.” The patient expressed concerns to the surgeon at the initial consultation regarding the perioral aesthetics of protuberant lips. The maxillary incisors were excessively flared by the routine sequence of orthodontic arch wires. Maxillary advancement surgery would worsen the appearance, whereas mandibular setback would not alter the upper lip. However, there was no communication by the surgeon at the initial planning stage. The option of first bicuspid extraction and anterior segmental repositioning would have achieved the occlusal goal and the patient’s aesthetic goals. The outcome was compromised by a lack of communication and understanding what each can achieve. A mandibular setback was offered to achieve occlusion but at the risk of an unfavorable ramal osteotomy and poor fixation, because the third molars would have been ideally extracted 6 months before the bilateral sagittal split osteotomy procedure. From the patient’s perspective, the options available are bewildering, and the potential to negatively affect the facial appearance and function is daunting. Even when the professionals feel that the ideal occlusion and facial appearance are achieved, the patient may be unhappy with the appearance despite the often dramatic improvement in appearance. Incorporating the change within the patient’s psyche can be difficult. I have had adolescents who were not sufficiently prepared for the physical changes to return to school and older patients in the third decade and beyond who equally were unhappy with what I considered an improved appearance. In two decades of experience, I have found the involvement of a psychologist from the initial discussion for orthognathic surgery to be critical. This is especially true in adolescence, when many patients are defining their identity and facing stress at home and social and academic stress at school. Our psychologists have uncovered suicidal ideations, drug and alcohol abuse, sexual orientation, and pregnancy unknown to the orthodontist, the surgeon, and the parents. Such sensitive issues within the context of dentofacial surgery, if missed, can lead to disastrous outcomes. Understanding the patient’s motivation for surgery is an important factor in a successful outcome.8,9 Taking the time to communicate the complexity of the orthodontic and surgical treatment and their impact is critical to optimizing the outcome with the end result of a satisfied patient comfortable with his or her new appearance and functional bite. The patient must have an understanding of limitations and compromises that may occur. Orthognathic surgery, whether needed for cleft or craniofacial conditions or for the more common developmental deformities, should be approached as a multidisciplinary team perspective and not just involve the orthodontist and surgeon independently driving the entire treatment plan. In addition, we have found it enormously beneficial to establish a dedicated “jaw” clinic, in which the vast majority of the patients are at various stages of jaw treatment. We have found that patients and their families become more comfortable with surgery after talking to each other in such settings. The supportive group that naturally develops is a powerful tool in communication that leads to a successful outcome. The wrong diagnosis will lead to the wrong surgery and to an unsatisfactory or unfavorable outcome. A classic example is patients who feel that their mandible is “too prognathic.” They come to the surgeon wanting to have their mandible and chin brought back. In a true profile view this may at first seem acceptable. But many of these patients will have subtle signs of midfacial deficiency that would be missed with this treatment plan and would be better served by a maxillary advancement procedure as the primary procedure to optimize their aesthetic appearance. The surgeon and the orthodontist should note the lack of dental display, the perialar deficiency, the acute nasolabial angle, the deficient columellar projection, and the convexity of the face that may extend to the zygomatic region. These can only be assessed when seeing the patient clinically in three dimensions and are often missed in the standard orthodontic two-dimensional photographs that often accompany the patient at the time of referral. Of all the images, the three-quarter oblique view often best reveals the midfacial deficiency that is commonly missed in the true lateral profile view. Another relevant example is when patients come to the surgeon initially for a recessed chin wanting a chin augmentation. Without assessing the dental occlusion, the aesthetic outcome from symphyseal surgery, whether osseous or alloplastic, may be unsatisfactory. If the patient has a significant class II dental relation indicating a mandibular body deficiency, then a “camouflage” genioplasty may result in an unnaturally deep labial mental sulcus if advanced to the desired projection. Such patients would benefit from an orthodontic assessment and consideration for a mandibular body advancement and an osseous genioplasty. There also may be symptoms of obstructive sleep apnea (OSA) that can be missed if the surgeon focuses only on the chin projection without considering occlusion and retroglossal airway space. The origin of the occlusal discrepancy can unfavorably influence the outcome of surgery if the underlying cause is not addressed or taken into account in the treatment planning. Concerns of relapse, vascularity, and secondary impact on velopharyngeal dysfunction are greater for patients with facial clefts requiring maxillary advancement than for patients with developmental dentofacial skeletal deformities. Patients with developmental dentofacial deformities who present for correction of an anterior open bite deformity are at an increased risk of relapse if the underlying cause of tongue thrust is not managed. Patients with condylar hyperplasia who present with prognathic mandibular asymmetry and occlusal class III cross-bite may exhibit continued asymmetric growth with a resulting recurrence of the condition if the underlying pathology remains active. Patients who undergo mandibular advancement surgery may progressively relapse with time as a result of underlying temporomandibular joint (TMJ) pathology, such as juvenile rheumatoid arthritis or idiopathic progressive condylar resorption unrecognized before surgery. Optimizing the outcome demands an understanding of the underlying causes of the dentofacial skeletal deformity whether of congenital, developmental, or traumatic origin, each of which influence the outcome differently despite the similarity in surgical procedure and desired goals. Accurate records are needed for diagnosis and to detail the orthodontic and surgical treatment planning at two critical time points: (1) at the beginning before there is any intervention, a diagnostic setup, and (2) at the time of surgical planning weeks before the procedure, a surgical setup. Too often the surgeon is brought into the picture in the middle of orthodontic treatment, and the only involvement is at the time of the surgical setup (the model surgery), resulting in compromises that could have been addressed at the time of the diagnostic setup. At both junctures, the setup must be accurate to reflect the patient’s initial dentoskeletal anatomy and allow the team to predictably plan the optimal end point. Historically, the complexity of the three-dimensional facial architecture was reduced to a series of two-dimensional records captioning the soft tissue envelope using photography and the underlying skeletal framework with plain radiographs in multiple orthogonal planes. The dental models were the only component that was recorded in three dimensions, and they required using a face-bow for positioning in the three-dimensional space. However, developing an accurate three-dimensional composite model of a patient’s condition by registering each of the two-dimensional orthogonal radiographic planes (lateral cephalometric and frontal cephalometric) and the two-dimensional photographs (frontal and profile views) with the mounted three-dimensional dental models had its own difficulties. Registration errors would build with each step, and any simulation of the treatment planning (sectioning and repositioning the plaster-mounted models) would lead to uncertainty about the accuracy of transferring the surgical plan to the operating room.10,11 Beyond the laboratory technical errors is the fundamental difficulty in the consistency of the head position and in the difficulty in accurate face-bow mounting in the cases of asymmetry that would involve the ear, the skull base, the orbits, and dual-plane maxillary–mandibular asymmetry. Traditional model surgery worked well in the routine developmental dentofacial skeletal cases, in which the vast majority of patients’ problems could be captured within the two-dimensional sagittal plane. However, when the problem extends to the third dimension, where yaw, roll, and pitch of the maxilla and the mandible play a role, it becomes less reliable, and successful orthognathic surgery becomes more of an art than a series of well-defined steps to a desired outcome. In cases of asymmetry, the roll and the pitch are easier to correct, but the yaw is missed because of the inability to accurately visualize the problem in the transverse plane. Today, surgical-orthodontic management has become increasingly reliable with the ability to visualize structures using three-dimensional radiologic cone beam computed tomography (CBCT) and software that allows the surgeon to simulate surgery with three-dimensional movement of the skeletal components.12,13 The next generation of maxillofacial surgeons will be fully immersed in three-dimensional technology, allowing a virtual orthodontic and surgical simulation that is specific to the patient’s anatomy.14–16 Although the technical execution of the planning and model surgery would be expected to improve with elimination of registration errors, it is important to remember Obwegeser’s Principle Number 35,17 “The computer can show you what you can achieve with your planning but cannot plan for you.” Knowing where to position the maxillary–mandibular skeletal bases and the dental arches relative to the desired soft tissue envelope is dependent on the surgeon’s and orthodontist’s eye, experience, and intuition, which cannot be replaced by a computer.17 Accurate clinical and radiographic diagnostic assessment of the facial appearance and the underlying dentofacial skeletal structure will point to the structural regions that are malpositioned and malsized relative to the skull base and to each other. The problem is not in determining what is wrong, but determining where the skeletal elements and consequently the dental component should be positioned.18,19 The surgeon and orthodontist will each have their own notion of the normative facial structure, and the patient will likely have a differing internally biased expectation of the desired facial appearance. Orthodontists often rely on normative cephalometric numbers, which is understandable because cephalometric analysis is historically rooted in the profession. Patients typically base their expectations on what they see in the media of models and actors. The surgeon must balance the patient’s expectations with what can be realistically achieved by defining the new skeletal framework and the occlusion simultaneously. It is important to understand that no patient wishes to look “average” and that the use of normative cephalometric data should only be used as a guide.20,21 As an illustration, although a sella–nasion–A point (SNA) angle of 82 degrees is considered an average, it may be unattractive compared with an SNA angle of 84 degrees or more if this would result in an attractive facial appearance with fullness and better support of the midfacial soft tissue envelope. An SNA angle greater than 82 degrees may also have a significant favorable effect on the patient’s smile. Buccal corridors that are empty before the advancement can be better filled with the dentition from canine to canine for a more attractive, fuller smile. A lesser advancement would result in a less full smile. Because the dentition can be adjusted orthodontically and the dental arch as a unit surgically, the final desired maxillary and mandibular incisor inclinations and thus the orthodontist and the surgeon determine the smile aesthetics to be achieved by the treatment. Comparing for the patient the difference between the patient and his or her siblings and parents serves as a guide toward what goals can realistically be achieved. Once the final skeletal position is determined relative to the skull base, the surgeon and the orthodontist need to work backward. The orthodontist needs to determine what to do with the teeth to allow the surgeon to achieve the final skeletal position in the construction of the desired face. A classic example is in cleft patients who present with a class III dentofacial skeletal relationship, in which the skeletal deficiency is more than the dental discrepancy. The surgeon would like to significantly advance the midface, but the skeletal advancement is limited by the minimal discrepancy at the occlusal level (insufficient negative overjet). The outcome would be less than ideal without orthodontically increasing the negative overjet. If the orthodontic preparation was not ideal, alloplastic implants may be needed as a compromise. Similarly, for class II patients who would benefit from significant mandibular body advancement, the occlusal relationship may be insufficient to allow for the desired advancement, and the projection of the facial plane must be made up by an osseous genioplasty. There must be adequate dental decompensation to make the occlusal relationship worse to achieve the desired skeletal movement to optimize a favorable outcome. Although the treatment planning options are well established to optimize outcome in the developmental dentofacial skeletal cases, for congenital conditions ranging from minor facial clefts to syndromic conditions as Goldenhar and Treacher Collins, the path to the final goals is not as clear. Classic approaches are challenged by severe tissue deficiency at multiple tissue planes and severely abnormal architecture, so simple rearrangement of the existing skeletal elements cannot be achieved in a stable manner without bone grafts. Unlike developmental cases, for which surgical intervention primarily takes place at skeletal maturity, the need to intervene in the actively developing immature skeleton is motivated by functional concerns and the need to limit compensatory or progressive distortion of the anatomy. Distraction osteogenesis allows the surgeon to use the biologic machinery to lengthen bone and expand the hypoplastic surrounding soft tissue matrix: muscle, nerve, and integument. It is in such cases that the surgeon enlists the aid of the orthodontist to support the functional and reconstructive goals with the understanding that the occlusal outcome may initially be less than ideal with distraction alone. Solving the three-dimensional nature of the problem is hindered by the limited ability to control the vector of the distraction process because of the simplicity of the mechanical devices. It is generally unidirectional and at best bidirectional. Thus, in the end, classic orthognathic procedures are likely needed to fully control the three-dimensional nature to optimize the outcome. The surgeon must therefore communicate to the patient and the family that a distraction may need to be multistaged to address the different vectors through different periods of growth and development, and that classic orthognathic surgery is commonly needed at skeletal maturity to allow the surgeon and the orthodontist full three-dimensional control over the reconstruction. Expectations must be managed. Skeletal surgery is “carpentry,” and that carpentry does not restore normal growth and development in these children. It puts the bones where they should be, but in a growing child the arrangement is not likely to remain ideal, either because of relapse or lack of growth. Relapse can be limited by distraction, but may not restore growth because of the underlying pathology. Optimizing the outcome of orthognathic surgery for cleft patients begins long before skeletal maturity (Fig. 43.3). In my practice, it begins in early adolescence at age 12 to 14 years, when it is important that both the surgeon and the orthodontist assess the cleft patient and begin the discussion with the family of the possible need for skeletal correction and occlusion depending on mandibular growth and on the maxillary deficiency that is common at this age. Early discussion with the family, monitoring growth, and a close working relationship with the orthodontist will alleviate some of the difficulties that may be encountered in late adolescence if treatment planning is delayed. The surgeon and the orthodontist must address several considerations in early adolescence: 1. Status of the alveolar bone graft 2. Need for cleft orthognathic surgery 3. Management of the typically missing lateral incisor Ideally patients have undergone phase I orthodontics that would involve transpalatal expansion, initial alignment of the dentition, and iliac bone grafting of the primary alveolar cleft in early mixed dentition. If this has not been addressed, it should be done before initiating phase II orthodontics when the patient is in permanent dentition. This is needed to support the dentition adjacent to the cleft margin, allow canine eruption and orthodontic movement across the cleft site, and improve gingival-mucosal vascularity. In many cleft patients, the lateral incisor is congenitally missing, has been extracted because of inadequate bone support, or is lost because of dental caries. A decision must be made with the family, the orthodontist, and the restorative prosthodontist whether to maintain the dental space for an implant-retained dental prosthesis or a bridge versus segmental maxillary osteotomy and closure of the dental space by moving the canine into the lateral incisor position. If a canine substitution is planned by advancing the lesser alveolar segment, then the cleft site may not need to be grafted before segmentation unless bone is needed to support the central incisor and canine root. In many cleft patients, there is a transverse width discrepancy even after phase I orthodontics that is significant in adolescents at the time of consideration for phase II final orthodontic-surgical management. Although a segmental Le Fort I osteotomy can correct a residual transverse width discrepancy, my experience is that immediate surgical expansion at the time of surgery can be accomplished but difficult to maintain despite orthodontic retention because of the relapsing forces of an inelastic scarred palatal mucosa. Our preference is to correct the transverse width with slow expansion using a transpalatal expander and when needed unilateral or bilateral maxillary osteotomy (surgically assisted palatal expansion) before formally correcting the sagittal and vertical skeletal discrepancies. Thus my goals for cleft patients include the following: 1. Convert a multisegmented cleft alveolus to a noncleft single dental maxillary alveolar arch. 2. Address the missing lateral incisor early in the planning in terms of substitution versus replacement. 3. Correct the transverse width discrepancy before sagittal and vertical advancement (with surgically assisted palatal expansion if needed). 4. Optimize the facial skeletal aesthetics by maximal dental decompensation with a treatment plan established in early adolescence well before skeletal maturity. There are pitfalls in the preparation of the dentition for orthognathic surgery that must be well understood by the orthodontist and the surgeon.6,22,23 Less-than-ideal orthodontic preparation will lead to a less-than-ideal surgical and occlusal outcome (see Fig. 43.2). In patients with skeletal discrepancies requiring orthognathic surgery, dental compensations occur as a natural biologic response to optimize occlusion in the face of maxillary–mandibular discrepancy. These dental compensations occur in all three planes: anterior-posterior, transverse, and vertical. A surgeon whose goal is to optimize the aesthetic skeletal outcome and an orthodontist who seeks to achieve maximal coordination (intercuspal relationship) of the dental arches must agree on the extent to which the teeth must be decompensated before skeletal surgery. Failure to communicate at the outset the goals from each perspective and the compromises that must be made will result in a disappointing outcome. The goal is determine the ideal skeletal projection and then determine how to handle the dentition to achieve the desired skeletal result. Fig. 43.3 This patient had been undergoing orthodontic treatment for more than 2 years when he was referred to a surgeon at age 18 years, 3 months before his high school graduation. The patient and his parents were anxious for the “final” surgery shortly after graduation because he was planning to attend college in another city. However, the cleft alveolus was never reconstructed, and there was a missing lateral incisor. Ideally one of the options discussed with the family would have included cleft alveolar bone grafting for stabilization of the dental arch with preservation of space 10 for subsequent osseointegrated implants versus a segmental Le Fort I closure of the dental space with a canine substitution for the missing lateral incisor. Because the patient would need correction of the mandibular asymmetry, the impacted mandibular third molars would have been extracted well before the orthognathic surgery to minimize unfavorable osteotomies. In addition, the patient had velopharyngeal insufficiency that would likely worsen with the maxillary advancement. Thus the critical need for surgery for the velopharyngeal incompetence limited by the mid-August start of school made it nearly impossible to proceed with the cleft orthognathic surgery as the family had planned. The cleft nasal and lip revision surgery needed to be addressed after the orthognathic surgery, but the patient was hoping to have had this improved before he started college. This case illustrates the importance of thoughtful treatment planning at the beginning of care before initiating orthodontic treatment. In patients with a class III skeletal pattern, the maxillary incisors are typically flared and the mandibular incisors are upright or even retroclined. Failure to appropriately decompensate will result in an insufficient negative overjet and in turn will result in inadequate maxillary advancement and/or inadequate mandibular setback to optimize the aesthetic outcome. The surgical goals are thus compromised. Additionally, inadequate decompensation may result in inability to achieve a class I buccal segment limited by the angulation of the anterior dentition. The occlusal goals are thus compromised. When a significant negative overjet is needed from a skeletal perspective, the anterior dentition from canine to canine can be righted and retracted by extracting either the first or second premolars to make room in the dental arch. Which set of premolars to extract depends on the amount of crowding and the amount of retraction needed. In the lower arch, decompensating the lingual inclined or righted mandibular incisors allows for further increase in the negative overjet. With severe anterior mandibular dental crowding, extraction of a single central incisor can be an option. Leaving the patient with three central incisors can be an acceptable compromise, because the lower dental midline is not visible until late in life. Moreover, decompensating by proclining the lower anterior dentition improves the support and aesthetic projection of the lower lip to create a desirable labial-mental sulcus. In patients with a class II skeletal pattern, the opposite occurs. The mandibular incisors are flared (proclined) and the maxillary incisors are righted. In patients with severe convexity who would benefit from maximal mandibular advancement from an aesthetic perspective and functionally from an airway perspective, the orthodontic goal would be to maximally decompensate the dentition to increase the positive overjet. Failure to maximally decompensate the anterior dentition limits the surgeon’s ability to advance the mandible and limits the orthodontist’s ability to achieve class I buccal segments postsurgically. Maximal decompensation may require extraction of either the first or second mandibular premolars to allow retraction of the anterior dentition into the extraction spaces. Additionally, proclining the maxillary incisors adds additional overjet to the mandibular decompensation and improves the upper lip support. As with the anterior-posterior compensations for skeletal discrepancies, there is transverse compensation that needs to be addressed in the presurgical phase to prevent postsurgical cross-bite and lingual-buccal inclinations. This is best assessed by hand articulating dental study models in a class I canine relationship. The decision that the orthodontist and the surgeon must make is whether the transverse width discrepancy can best be addressed by orthodontically based expansion alone, surgically assisted orthodontic expansion, or multisegmental surgical maxillary expansion. When the intercanine width is narrow, a two-segment maxillary expansion is an option to correct the width discrepancy. If the intercanine width is appropriate but there is a posterior buccal cross-bite, a three-segment maxillary expansion can be considered. Thus there must be sufficient interdental spacing and root divergence to allow the surgeon to safely accomplish the interdental osteotomy to minimize compromising adjacent tooth vitality. For patients who present with apertognathia, a Le Fort I osteotomy with posterior maxillary impaction will allow skeletal closure of the open bite. In such patients the curve of Spee may be excessive, and prior leveling of the curve should be done with care. Mandibular incisors will typically be overerupted and decompensated orthodontically. However, orthodontic leveling of the curve of Spee in the maxillary dental arch may create a risk for postoperative relapse and recurrence of the open bite, especially when the vertical leveling must exceed 2 mm. Excessive maxillary incisor extrusion before a single segment Le Fort I surgery is likely at risk for relapse of an open bite of dental origin. In such cases multisegmental orthodontic alignment and osteotomies are a more stable treatment choice. Operative complications of orthognathic and maxillofacial distraction surgery can be categorized by the surgical technique (Box 43.1). However, because the various maxillofacial surgical procedures are interrelated and are commonly performed in combination, operative complications are best discussed in the following broad categories. Intraoperative airway control is critical; nasoendotracheal intubation is necessary for surgical treatment of occlusion with maxillary–mandibular fixation. Nasal intubation can be difficult in patients with facial clefts who have previously undergone a pharyngeal flap procedure. Intubation can be accomplished with fiberoptic guidance and/or exchange over a stent after oral intubation. Occasionally, nasal intubation is not possible and, although less preferable, the procedure can be performed in these cases with orotracheal intubation and with the oral tube positioned retromolar at the time of maxillary–mandibular fixation. During the posterior aspect of the Le Fort I osteotomy, the nasotracheal tube is particularly at risk at the times of septal–vomer dysjunction and with the osteotomy of the lateral nasal wall on the side of the tube. The tube itself or the access to the balloon cuff can be lacerated or transected by the osteotome or by the reciprocating saw.24,25 In the case of complete transection, immediate air leak or loss of air exchange is evident by blood within the endotracheal tube. To prevent endotracheal tube injury, I first perform the septal dysjunction with a guarded osteotome; this facilitates placement of the reciprocating saw within the nasal piriform, because the septum and nasotracheal tube are deflected to the opposite side, decreasing the risk of injury to the tube. The maxillary osteotomy is made with a reciprocating saw and should be directed from medial to lateral, away from the nasotracheal tube (Fig. 43.4). If injury to the nasoendotracheal tube occurs, exchange of the tube is easier before the maxillary osteotomy is initiated.25 In the case of laceration of the tube or the balloon and a resulting mild air leak when tube exchange would be difficult, posterior oropharyngeal packing may be beneficial in controlling the air loss. There are several reasons for increased airway resistance after completion of the maxillary–mandibular surgery. Intermaxillary fixation increases airway resistance, reducing peak air flow, and patients who have undergone a Le Fort I procedure in addition will necessarily have some degree of nasal airway obstruction.26 For these reasons, many prefer no maxillary–mandibular fixation or only guiding elastics during the immediate recovery period. Coughing or straining with agitation can cause a fracture or an avulsion of the internal fixation hardware. Avoiding maxillary–mandibular fixation may also reduce the risk of this complication. I prefer not to use any maxillary–mandibular fixation during the immediate recovery phase for patient comfort until the first postoperative appointment, 1 to 2 weeks after surgery. Any preexisting coagulopathy should be determined through a history and physical examination. Patients should be specifically asked about a history of excessive bleeding after minor injuries or bleeding after previous procedures such as third molar extractions. In addition, a careful medication history should be taken, with particular attention to the use of medications such as aspirin, other medications with anticoagulant properties, and herbal or nonformulary medications whose composition might not be clear. These should be stopped long before surgery. Maxillary Procedures (Le Fort I) • Avascular necrosis • Dental injury (segmental) • Fixation failure (plates, screws, and distraction devices) • Gingival recession (segmental) • Hemorrhage • Infection • Injury to the internal maxillary artery • Injury to Stensen’s duct • Lacrimal duct injury • Malocclusion or relapse • Maxillary sinusitis • Nasal septal deviation or perforation • Traction injury of the infraorbital nerve • Transection of the descending palatine neurovascular (inevitable) • Transection of nasopalatine artery • Unanticipated fractures • Vascular injuries (arteriovascular fistula, aneurysm) • Velopharyngeal insufficiency • Vision (blindness) Mandibular Procedures (Bilateral Sagittal Split Osteotomy, Intraoral Vertical Ramus Osteotomy) • Avascular necrosis • Condylar resorption • Fixation failure (plates, screws, and distraction devices) • Hemorrhage • Infection • Traction injury of the inferior alveolar neurovascular bundle • Traction injury of the lingual nerve • Transection of the inferior alveolar neurovascular bundle • Malocclusion or relapse • Malpositioned proximal ramus • Unanticipated fractures • Vascular injuries (arteriovenous fistula, aneurysm) Genioplasty • Gingival recession • Fixation failure (plates and screws) • Mental nerve injury • Mandibular border contour deformity Fig. 43.4 Endotracheal tube position after nasotracheal intubation. The balloon tubing and/or the endotracheal tube can be lacerated. The endotracheal tube may be injured during osteotomy through the medial buttress. Directing the saw from medial to lateral will minimize the risk of transecting the endotracheal tube. Separating the septum first will increase the intranasal space before the maxillary osteotomy and facilitate placing the saw within the nasal cavity. The use of local anesthetic with a vasoconstrictor and controlled hypotensive anesthesia significantly reduces generalized bleeding and the need for blood transfusion while greatly improving visualization of the operative field.27,28 One study demonstrated controlled operative hypotension reduced blood loss by approximately 44%.29 Significant hemorrhage is uncommon, but it is more likely with maxillary osteotomies.3,29 With maxillary osteotomy, the vessels at risk include the greater palatine vessels, the maxillary artery, and the pterygoid plexus.30,31 Bleeding from the descending palatine vessels occurs when the posterior aspect of the lateral nasal wall osteotomy is made and, in most circumstances, spontaneously stops as it is retracted into the bony canal. However, in such circumstances it is important to carefully visualize the site of the descending palatine vessels and coagulate with a flat-tip monopolar cautery pressed against the bone. When bleeding persists and the vessels can be visualized, it is easily controlled by vascular clips or bipolar electrocautery once the maxilla is downfractured. Such lacerations can be avoided by stopping the osteotomy at the palatine bone and keeping it as low as possible near the tuberosity as the maxilla is slowly downfractured and the vessels identified. The descending palatine artery may also be compromised during pterygomaxillary separation and may require pterygopalatine fossa packing. Because the separation of the pterygopalatine plate with an osteotome is not directly visualized, placement of the osteotome at its inferior aspect by palpation is critical to avoid injury to the vessels within the pterygopalatine fossa. The margin of safety is approximately 10 mm.32 Hemorrhage, when it does occur, can be rapid and is best controlled by dense packing of the fossa with cottonoid sponges soaked in an epinephrine solution. In most cases, bleeding, although significant, is easily controlled by local measures. When bleeding cannot be controlled by local measures, the operative site should be packed with cotton, the maxilla returned to its original position for compression and plated, and the patient transferred to interventional radiology for vascular control via embolization. Carotid ligation is a means of last resort if interventional radiology is unavailable and the bleeding cannot be controlled by these maneuvers. While significant hemorrhage with mandibular osteotomies (bilateral sagittal split osteotomy [BSSO], intraoral vertical ramus osteotomy [IVO]) is uncommon, the vessels at risk include the inferior alveolar, the maxillary, and the facial arteries; the retromandibular vein; and the pterygoid venous plexus.33–36 Careful subperiosteal dissection, retraction of soft tissues, and lateral splitting protected by appropriate retractors help prevent vascular injuries in most patients. During the exposure of the medial surface of the ramus, vascular injury to the inferior alveolar neurovascular bundle where it enters the mandible may occur with inadvertent supraperiosteal dissection. In dissecting the medial ramus, it is helpful to start the dissection anterior to posterior and superior to inferior. As the exposure continues inferiorly from the sigmoid notch, the inferior neuromuscular bundles are reflected and protected by the elevator and/or a medial ramus retractor. If bleeding occurs, epinephrine-soaked cotton can be used temporarily to pack the medial ramus to control the bleeding; however, the split may need to be completed before bleeding from the posterior ramal border can be controlled. At the time of splitting of the mandibular ramus, the inferior alveolar neuromuscular bundles are at risk. Using a wedge-shaped osteotome and directing the split along the lateral cortex can minimize the risk of injury, but the risk cannot be fully eliminated because the bundles course within a narrow width of the ramus. Bleeding along the course of the artery resulting from injury at the time of the split usually stops spontaneously. If it does not, the artery can be dissected away from the inferior alveolar nerve and carefully ligated. Cauterization poses a risk to the nerve and should be avoided. In addition, at the time of the split, the inferior and posterior border must be protected with a channel retractor to minimize risk to the facial artery and retromandibular vasculature. For persistent bleeding, as may occur when the masseteric or the facial artery is injured during mandibular osteotomy, temporary packing with pressure is sometimes helpful. Significant facial artery injuries require isolation of the vessel and its ligation.37 Even with intraoperative control, patients will present in the immediate postoperative period with bleeding as they become normotensive. Any expanding hematoma should of course be reexplored immediately. In most cases the descending palatine artery is the primary source of postoperative bleeding missed intraoperatively.38 It is preferable to allow the patient to become normotensive after the osteotomies and downfracture to control any actively bleeding vessels. It is important to note that intraoperative vascular events that may be life-threatening may only become evident in the outpatient setting in the early recovery period weeks after the surgery (Fig. 43.5). Uncontrolled epistaxis, arteriovenous fistulae, false aneurysms, carotid cavernous fistulae, and carotid artery thrombosis after either maxillary or mandibular osteotomies have been reported as isolated rare case reports.39–42 Suspicion must be high, and computed tomography (CT) angiography and embolization are needed. Mucosal degloving, osteotomies, and repositioning of the facial skeletal elements may reduce the blood supply to the osteotomized segment significantly. This reduction in blood supply can affect both the skeletal and soft tissue elements (pulp, periodontium, and gingiva). Usually, this vascular compromise is transient without significant clinical impact on the outcome.31,43 Devitalization of the teeth, periodontal defects, and segmental bone loss have been described after segmental Le Fort I osteotomies44,45 (Fig. 43.6). These complications often have been attributed to incisions, to excessive stripping of the periosteum, to scars in the palatal mucosa (secondary to previous cleft surgery), to interdental or segmental osteotomies with loss of the attached gingiva, and to transverse expansion with an excessive stripping of the palatal mucosa. When persistent intraoperative gingival cyanosis is noted during the surgery, the surgeon may consider returning the maxilla to its original position and placement of midfacial distraction appliances at the time of the procedure. An alternative is readvancement 2 weeks after surgery when the mucosal vascularity is improved as a delayed advancement.
43
Orthognathic Surgery and Maxillofacial Distraction Surgery
Avoiding Unfavorable Results and Complicationsin Orthognathic Surgery and Maxillofacial Distraction Surgery
Preoperative Planning
Errors in Communication

Errors in Diagnosis
Records, Diagnosis, and Simulation
Treatment Planning
Preoperative Orthodontic Stage
Managing Unfavorable Results and Complicationsin Orthognathic Surgery and Maxillofacial Distraction Surgery
Operative Complications
Airway Complications
Hemorrhage
Vascular Compromise
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine