Oral Antifungal Agents: Introduction
|
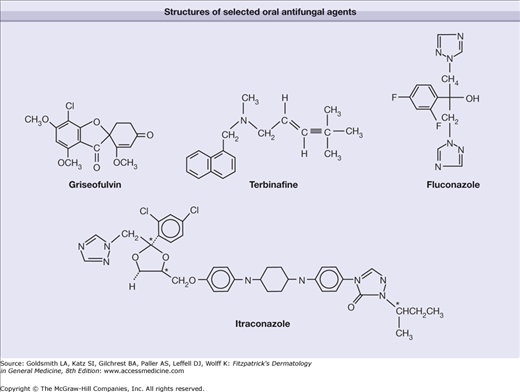
Oral antifungal agents are widely and frequently used for the treatment of fungal infections of the skin, nails, and mucous membranes.1 This chapter summarizes the four most widely used oral antifungal agents in dermatology: (1) terbinafine, (2) itraconazole, (3) fluconazole, and (4) griseofulvin.
Allylamines: Terbinafine
Terbinafine hydrochloride is a topical and oral antimycotic agent that belongs to the family of compounds known as the allylamines. Naftifine, a topical antifungal agent, also belongs to this class. All allylamine derivatives possess a tertiary allylamine, a structural component crucial for antifungal activity (Fig. 232-1).2 In vitro, terbinafine is highly active against dermatophytes but less active against molds, dimorphic fungi, and yeasts.2
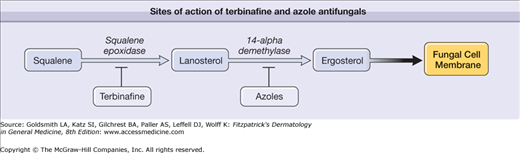
Terbinafine inhibits the enzyme squalene epoxidase in the fungal cell membrane, thereby blocking the biosynthesis of ergosterol (Fig. 232-2).3 Squalene epoxidase, a complex, microsomal noncytochrome P450 enzyme, catalyzes the first enzymatic step of ergosterol synthesis: the conversion of squalene into squalene epoxide. Consequently, terbinafine causes an abnormal intracellular accumulation of squalene and a deficiency in ergosterol.4 In-vitro accumulation of squalene accounts for the drug’s fungicidal activity by weakening the cell membrane, while deficiency of ergosterol is associated with the drug’s fungistatic activity, as ergosterol is a component of fungal membranes required for normal growth.4
Terbinafine is well absorbed from the gastrointestinal tract, mostly in chylomicrons. The distribution half-life is 1.5 hours, and the elimination half-life is 22 hours.5 Terbinafine is highly lipophilic and keratophilic in nature and, therefore, is widely distributed upon absorption throughout skin and adipose tissue. Terbinafine is extensively biotransformed by the liver through oxidation by CYP2D6. More than 80% of the drug is excreted in urine; the rest is eliminated with feces.6
The US Food and Drug Administration has approved terbinafine tablets for the treatment of onychomycosis due to dermatophytes. Terbinafine oral granules are approved for the treatment of tinea capitis in patients over 4 years old. Terbinafine also has clinically proven efficacy for select cases of tinea corporis, tinea pedis, or tinea cruris that are widespread, severe, or resistant to topical treatment (Box 232-1).
|
For the treatment of tinea capitis in children, terbinafine oral granules may be sprinkled over food such as pudding. The dosage is based on weight, with children weighing less than 25 kg receiving 125 mg/day, children weighing between 25 and 35 kg receiving 187.5 mg/day, and children weighing over 35 kg receiving 250 mg/day.7 The standard treatment course is 6 weeks.7 A study comparing a 6-week course of terbinafine 5–8 mg/kg versus a 6-week course of griseofulvin 10–20 mg/kg showed that mycological cure and complete (mycological plus clinical) cure rates were significantly higher for terbinafine than for griseofulvin.8 However, subgroup analysis revealed that among patients infected with Microsporum canis, mycological and complete cure rates were superior with griseofulvin.8 Conversely, among patients infected with Trichophyton tonsurans, mycological and complete cure rates were superior with terbinafine.8
Terbinafine can also be safely used in children for onychomycosis when dosed by weight as for tinea capitis.9
Terbinafine is indicated for the treatment of onychomycosis of the toenails and fingernails caused by dermatophytes.10 A dose of 250 mg/day for 12 weeks is typically used.
Several studies have compared the standard 12-week regimen of terbinafine to itraconazole, used in either a continuous or pulsed fashion. Terbinafine produced higher rates of clinical and mycological cures.11–14 In a study comparing continuous terbinafine with intermittent itraconazole (1 week of treatment per four weeks) in the treatment of toenail onychomycosis, terbinafine was significantly more effective than pulsed itraconazole.11 At week 72, the mycological cure in those patients treated with a 3-month daily course of terbinafine was 76%, compared with a mycological cure rate of 38% in those patients treated with a 3-month course of intermittent pulse therapy with itraconazole. A longer follow-up of these patients at an average of 54 months revealed 46% cure after continuous terbinafine versus 13% cure after the pulsed itraconazole12; similar results were found by others at 2-year follow-up.13 Twelve weeks of terbinafine 250 mg/day is clearly superior to itraconazole 200 mg/day, with mycological cure rates of 73% versus 46% after 48 weeks of follow-up.14
Studies comparing various intermittent dosing regimens of terbinafine to the gold standard of continuous 12-week therapy for toenail onychomycosis have yielded mixed results.15,16
No increase in mycological cure rate is gained by aggressive debridement of the toenail when combined with terbinafine; however, the clinical appearance of the nail is improved with debridement.17 Additionally, aggressive nail debridement, when combined with oral terbinafine, improves treatment satisfaction and reduces symptom frequency.18 The addition of a topical lacquer such as ciclopirox 8% lacquer or amorolfine 5% lacquer (see Chapter 219) enhances clinical efficacy when used with terbinafine and then continued for 6–9 months after the cessation of terbinafine.19,20
Tinea corporis, tinea cruris, and tinea pedis can be treated with oral terbinafine with high clinical and mycological cure rates. In a study of 22 patients with tinea corporis and tinea cruris who used terbinafine 250 mg daily for 1 week, 100% clinical and mycological clearing was observed at 6 weeks.21 In a study of moccasin tinea pedis and tinea manuum, after a 2-week course of terbinafine, 250 mg daily, there was an 86% mycological cure rate at 8 weeks.22 Two placebo-controlled trials demonstrated that a 4- to 6-week course of terbinafine 250 mg daily is effective in the treatment of seborrheic dermatitis23,24 (see Chapter 22). Interestingly, terbinafine is not effective orally for the treatment of tinea versicolor,21 but twice daily application of topical terbinafine 1% solution, cream or gel, has been effective in randomized placebo-controlled trials.25
Terbinafine is well tolerated by the elderly and requires no further cautions than those for the general population.26 A study of 504 patients older than 65 years of age confirmed efficacy and tolerance of the standard adult regimen for onychomycosis, with no reported drug interactions.27
Terbinafine is a pregnancy category B drug.10
Terbinafine is supplied as a 250-mg tablet or packets of oral granules. See Table 232-1.
Adult | Pediatric | |
|---|---|---|
Onychomycosis | Fingernails: 250 mg/day × 6 weeks Toenails: 250 mg/day × 12 weeks | 3–6 mg/kg/day × 6–12 weeks |
Tinea capitis | 250 mg/day × 2–8 weeks | Under 25 kg: 125 mg/day × 6 weeks 25–35 kg: 187.5 mg/day × 6 weeks Over 35 kg: 250 mg/day × 6 weeks |
Tinea corporis, tinea cruris | 250 mg/day × 1–2 weeks | 3–6 mg/kg/day × 1–2 weeks |
Tinea pedis (moccasin) | 250 mg/day × 2 weeks | |
Seborrheic dermatitis | 250 mg/day × 4–6 weeks |
Positive tests [potassium hydroxide (KOH), culture, histology] for fungal infection should be documented before initiation of oral terbinafine therapy. Pretreatment serum transaminase tests are advised for all patients before taking terbinafine, and the drug is not recommended for patients with liver or renal disease.22
Many physicians advocate monitoring liver function after 6 weeks of therapy, although the incidence of hepatic toxicity is very low [see Sections “Complications (Adverse Effects)” and “Risks and Precautions”]. Because of transient lymphopenia observed in patients on terbinafine, complete blood cell counts should be monitored in immunodeficient patients who are receiving terbinafine for longer than 6 weeks.28 If signs or symptoms of secondary infection occur in patients while on terbinafine, a complete blood count should be performed to rule out neutropenia.28 Cautions and monitoring in children are the same as for adults, but there is evidence that children may suffer fewer adverse events.9
Because of its high selectivity, terbinafine is generally well tolerated with a low incidence of adverse side effects. The most common side effects after oral administration are of a gastrointestinal nature (3.5%–5.0%).29 Other rare side effects include headache, exanthematous eruption, acute generalized exanthematous pustulosis, pustular psoriasis, subacute cutaneous lupus erythematosus, chest pain, elevated laboratory parameters, loss of taste, fatigue, and malaise.28–33 A few cases of hepatocellular injury (including fulminant hepatic failure),34,35 reversible agranulocytosis,36 and severe skin reactions, including toxic epidermal necrolysis and erythema multiforme, were also reported.37
Terbinafine should be prescribed with caution in patients with hepatic disease or history of hepatic toxicity with other medications (Box 232-2). Furthermore, there is insufficient data to recommend its use in patients with renal impairment. Because terbinafine rarely causes a lupus-like rash and neutropenia, patients with known systemic lupus erythematosus or immunodeficiency also may not be good candidates for this medication.10
|
Terbinafine is not contraindicated with any specific drug. However, cytochrome P450 (CYP) enzymes metabolize terbinafine. Plasma clearance of terbinafine is increased by the P450-inducer rifampin and decreased by the P450-inhibitor cimetidine.38 Terbinafine is also reported to decrease cyclosporine levels by increasing cyclosporine clearance.22,39 Isolated reports of interactions with warfarin have been reported; however, prospective pharmacokinetic studies have not revealed any clinically significant reactions.39 It was shown that terbinafine inhibits CYP2D6, a cytochrome P450 isoenzyme that metabolizes tricyclic antidepressants and other psychotropic drugs.40 Other drugs predominantly metabolized by this enzyme include β-blockers, selective serotonin reuptake inhibitors, and monoamine oxidase inhibitors type B.22 In a postmarketing surveillance study of patients on terbinafine, no adverse drug interactions with CYP2D6 substrates were reported.41 However, there have been two reports of nortriptyline intoxication induced by terbinafine.42,43
Triazoles
Both itraconazole and fluconazole are triazole antimycotic agents sharing a common structural moiety—a triazole ring—not found in azoles of the imidazole family.
Itraconazole (Fig. 232-1) is a highly lipophilic compound that has a wide spectrum of activity.44 In vitro, it is fungistatic and effective against dermatophytes, yeast, molds, and dimorphic fungi.45–47
Itraconazole inhibits 14-α-demethylase, a microsomal cytochrome P450 enzyme, in the fungal membrane (Fig. 232-2).48 14-α-Demethylase is necessary for the conversion of lanosterol to ergosterol, which is the principal structural component of the fungal cell membrane.46 Consequently, the accumulation of 14-α-methylsterols leads to the impairment of membrane permeability and membrane-bound enzyme activity and to the arrest of fungal cell growth.
The serum concentration of itraconazole is influenced by several parameters, including food and gastric acidity.49,50 Itraconazole is extensively metabolized, primarily by the CYP3A4 isoenzyme system to more than 30 metabolites. Hydroxyitraconazole is the main metabolite. Approximately 54% of the metabolized drug is excreted in the feces, and 34% is excreted in the urine. After single-dose administration, the terminal elimination half-life is 21 hours for itraconazole and 12 hours for its active metabolite. The pharmacokinetic variables of itraconazole are not affected in patients with renal insufficiency.51 In patients with liver cirrhosis, the absorption is slightly increased and the half-life is prolonged because of a reduced first-pass metabolism. Absorption of the standard tablet formulation is decreased in patients with acquired immunodeficiency syndrome as a result of gastric hypochlorhydria.51 A new hydroxypropyl-β-cyclodextrin oral solution formulation is better absorbed in a fasting state than with food,52 appropriate for patients who cannot ingest large amounts of food or have high gastric pH. Young children, especially those less than 5 years of age, have lower serum levels than adults and usually require twice daily dosing.53
Itraconazole has the broadest efficacy compared to other commonly prescribed antifungals.47 Thus, it is a first-line therapy for infections due to Candida and other nondermatophyte species (Box 232-3).
|
Itraconazole can be used to treat tinea capitis in children. It is more often prescribed in the capsule formulation with food or acidic beverages such as colas because the cyclodextrin in the liquid form of itraconazole causes more gastrointestinal side effects such as diarrhea and also due to reports of neoplasms associated with high doses in murine and rat models.54 Nevertheless, for children who cannot swallow capsules or take capsules with food, the solution has a pleasant taste and is considered to be safe.55 Itraconazole is dosed at 5 mg/kg per day for 4–6 weeks.56 Children who weigh between 15 and 30 kg require one 100 mg capsule daily; children weighing 30–40 kg require 100 mg 1 day alternating with 200 mg the next day, to average 150 mg daily.57 Children weighing over 50 kg can be dosed as adults.55 Tinea capitis caused by T. tonsurans requires a course lasting 2–4 weeks58; however, a longer treatment course is recommended for M. canis.59 Because onychomycosis is less common in children than in adults, there is much less data available for treatment of pediatric onychomycosis. For better compliance due to decreased adverse effects, lower cost, and overall reduced exposure to drug, one can prescribe a pulsed regimen of 5 mg/kg/day for 1 week alternating with 3 weeks off; two pulses are recommended for fingernail involvement and three pulses for toenail involvement.9
The oral solution is a good option for oropharyngeal or esophageal candidiasis in children, even in fluconazole-resistant infections.53
Itraconazole has been approved for the treatment of onychomycosis caused by dermatophytes54 and is effective as continuous or pulse therapy. A 2-month course of itraconazole pulse therapy is necessary for fingernail onychomycosis, while toenail onychomycosis requires a 3-month course. A single course consists of 200 mg twice daily for 1 week per month. Itraconazole pulse therapy is at least equal in efficacy, if not superior, in the treatment of toenail onychomycosis when compared to continuous itraconazole therapy.60 Itraconazole has been used for the treatment of tinea pedis. A 1-week course of itraconazole, 200 mg twice daily, is more effective than 200 mg or 100 mg daily for 2–4 weeks.61 Nonetheless, itraconazole is less effective in the treatment of dermatophyte infections than terbinafine (see Section “Allylamines: Terbinafine”). Itraconazole at a dose of 200 mg daily for 5–7 days is effective in the treatment of pityriasis versicolor.62 Recurrence, which is common in this disease, can be prevented by taking 200 mg twice daily for 1 day a month.62
Itraconazole (pulse) therapy is effective and safe in the elderly and only requires caution in the setting of comorbidities and drug interactions [see Section “Complications (Adverse Effects)”].26
Itraconazole is a pregnancy category C drug, and therefore, is not recommended during pregnancy or while nursing because it is excreted in human milk.54
Itraconazole is supplied in 100-mg capsules, a 10-mg/mL oral solution, and an intravenous solution. Capsules should be taken with a full meal to ensure maximum absorption54 (see Table 232-2).
Adult | Pediatric | |
|---|---|---|
Onychomycosis | Fingernails: 200 mg bid × 1 week/month × 2 pulses Toenails: 200 mg/day × 12 weeks Or 200 mg bid × 1 week/month × 3 pulses | Fingernails: 5 mg/kg/day × 1 week/month × 2 pulsesa Toenails: 5 mg/kg/day × 1 week/month pulsed × 3 pulses |
Tinea capitis | 250 mg/day × 2–8 weeks | Trichophyton infections: 5 mg/kg/day × 2–4 weeks Microsporum infections: 5 mg/kg/day × 4–8 weeks |
Tinea corporis, tinea cruris, tinea pedis | 200 mg bid × 1 week or 100–200 mg/day × 2–4 weeks | Dose by weight × 1–4 weeks |
Oropharyngeal candidiasis Pityriasis versicolor | Swish and swallow solution 100–200 mg/day 200 mg/day × 5–7 days, prevent recurrence with 200 mg bid once/month | Swish and swallow solution by weighta |
Positive tests (KOH, culture, histology) for fungal infection should be documented before initiation of oral itraconazole therapy. Baseline evaluation of hepatic function is recommended in patients with preexisting liver disease, or if lengthy treatment is anticipated.54
Hepatic function monitoring is indicated through therapy only for those patients with preexisting liver disease or those with a history of hepatic toxicity with other medications.54,63 When itraconazole must be administered with medications, it is known to compete with for hepatic enzymes, appropriate monitoring for drug levels or toxic effects of these medications is indicated (see Section “Drug Interactions”).
The most common reported side effects associated with itraconazole therapy are of a gastrointestinal nature.64 Less-frequent adverse effects are hypertriglyceridemia, edema,65 urticaria, anaphylaxis, erythema multiforme, headache, neuropathy, impotence, hypertension, leukopenia, nephrotic syndrome, and mildly elevated liver enzymes.54,64 Instances of hepatic injury and, rarely, fulminant hepatotoxicity are associated with the administration of itraconazole. There are also rare reports of congestive heart failure and pulmonary edema. When administered intravenously to dogs and healthy human volunteers, negative inotropic effects were noted.66
Administration of itraconazole to patients with a history of heart failure is contraindicated, and it is not recommended for patients with a history of liver disease.54 There are also several significant drug interactions to be aware of (see Box 232-4).
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


