Nasal reconstruction has been refined to the point that its goals should include full restoration of form and function in addition to providing an aesthetically-pleasing result. Contemporary facial plastic surgeons have all the tools available in their armamentarium to repair the complex composite structure of nasal lining, structure, and skin cover. Nasal defects most often result from oncologic surgery or, less commonly, nasal trauma. While defects of nasal cover are more prominent, the impact of unrepaired nasal lining defects should not be underestimated. Meticulous repair of lining, structure and cover are all required for functional, stable and aesthetic nasal reconstruction.
Cause
Nasal reconstruction has been refined to the point that its goals should include full restoration of form and function in addition to an aesthetically pleasing result. Contemporary facial plastic surgeons have all the tools available in their armamentarium to repair the complex composite structure of nasal lining, structure, and skin cover. Nasal defects most often result from oncologic surgery (Mohs, wide local, or square excision) or nasal trauma. Of paramount importance in the reconstruction of oncologic defects is the confirmation of clear resection margins before undertaking reconstruction. Failure to confirm clear margins risks tumor recurrence, rendering moot the successful nasal reconstruction. Mohs micrographic surgery lends itself to immediate confirmation of clear margins. Wide local excision, on the other hand, relies on frozen-section analysis of a representative sample of the defect margin or delayed reconstruction, allowing time to confirm negative margins of permanent pathologic specimens.
Although this article focuses on reconstruction of oncologic defects, the principles discussed can be effectively applied to reconstruction of nasal-lining defects resulting from any cause. Restraint should be exercised in the initial management of traumatic, or otherwise contaminated, defects to allow elimination of potential wound contamination before repair. In many cases, expectant management results in sufficient healing by secondary intention to either reduce the significance of the required reconstruction or preclude surgical intervention.
Defect analysis
Critical analysis of a nasal defect should precede reconstruction of even the smallest wound. The primary goal of this exercise is to identify viable options on the reconstructive ladder and to choose the optimal modality among those in the reconstructive surgeon’s armamentarium. At the most basic level, nasal tissue may be divided into cover (skin, subcutaneous tissue, and nasalis muscle), structure (upper and lower lateral cartilages, septum, and nasal bones) and internal lining (vestibular skin and nasal mucosa). This article focuses on reconstruction of nasal-lining defects.
Unrepaired nasal-lining defects create two potential issues in nasal reconstruction. First, even small nasal-lining defects are subject to secondary intention healing. The resulting cicatricial contractile forces can result in distortion of the nasal framework. Second, unrepaired lining defects can expose overlying structural grafts. Exposed cartilage or bone grafts are susceptible to bacterial colonization and/or infection and lack the robust blood supply necessary for survival. Most nasal-lining defects occur in the context of a composite loss of full-thickness nasal tissue. Failure to restore continuity in the nasal lining risks wound infections, graft exposure, graft extrusion, and suboptimal functional and aesthetic results. Thus lining defects, especially of the lower third of the nose, must be meticulously repaired with primary closure, bipedicled vestibular advancement, inferior turbinate mucoperiosteum, septal mucoperichondrium, or septal composite pivotal flaps. Although additional options exist and are discussed in this article, these reconstructive modalities are ideal because they replace nasal mucosal lining with similar intranasal mucosal flaps. These methods maintain or replace the thin, supple, functioning nasal mucosal tissue to support nasal mucociliary clearance, humidification, and temperature regulation of inspired air.
Nasal-lining defects most often occur as part of a defect involving nasal structure and skin cover. Thus, in the context of discussing nasal-lining defects it is important to consider several basic principles of full-thickness nasal reconstruction. First, composite defects should be reconstituted with like tissue. In addition to reconstruction of the skin cover, discussed elsewhere, robust structure must also be provided using structural cartilage (concha, septum, rib) or bone (perpendicular plate, split calvarium) grafts. Structural grafts are used both to support the nose and to fine-tune the contour of reconstructed nasal unit(s). To achieve these goals, autogenous grafts are placed in both anatomic and nonanatomic locations, as described later.
Patient factors
Of the numerous patient factors to consider, one of the most important and modifiable risk factors is use of tobacco products. Current smokers are at risk for skin flap and graft failure. Nasal-lining flaps are particularly at risk in tobacco users given the thin, delicate nature and tenuous blood supply of commonly used flaps. If patients are unable to curtail use of tobacco products before reconstruction they must be counseled about the increased risk of graft or flap failure. These risks can be mitigated by eschewing skin grafts, raising thicker cutaneous flaps (recruiting a more robust subdermal vascular plexus) and minimizing wound closure tension (optimizing flap perfusion). Regardless of the precision of nasal skin and structure replacement, a deficit of nasal lining caused by flap loss or poor surgical planning results in impressive contraction of the reconstructed nasal unit(s), with the expected nasal deformity and impairment in nasal breathing.
A history of previous skin cancer or nasal surgery should be elicited. In some instances this might include a history of head and neck irradiation. In many cases, a pattern of alopecia in the beard or neck region delineates the area of previous cutaneous irradiation and potentially compromised skin vascularity. Both head and neck irradiation and intervening scars may be expected to compromise skin flap vascularity and viability. Specifically with regard to use of nasal-lining flaps, previous septoplasty, rhinoplasty, or turbinate surgery should be investigated to determine whether intranasal flaps are viable reconstructive options. Septal perforations should be identified because their location might preclude ipsi- and/or contralateral septal mucoperichondrial hinge flaps.
Reconstructive ladder
Nasal reconstruction requires careful composite reconstitution of missing nasal lining as well as structure and/or cover with like tissue. Given the diverse options for replacement of nasal lining, it is helpful to compartmentalize the options into a reconstructive ladder ( Fig. 1 ) that stratifies reconstructive modalities from least (secondary intention) to most complex (free-tissue transfer). Secondary intention healing can be successful for carefully selected small defects limited to the nasal lining. Some nasal-lining defects of 5 mm or less can be closed primarily with careful undermining. However, most nasal-lining defects require repair with pedicled soft-tissue flaps such as bipedicled vestibular advancement, inferior turbinate mucoperiosteum, septal mucoperichondrial hinge, septal composite pivotal, or paramedian forehead flaps. In rare cases, microvascular free-tissue transfer is required for recreation of nasal lining. Detailed discussion of free-tissue transfer is beyond the scope of this article but is well described elsewhere.
Secondary intention
Secondary intention is the most simple, and infrequently used, method of managing nasal-lining defects. No intervention beyond proper local wound care and monitoring the wound-healing process is required. General wound-healing principles to be observed include minimizing the bacterial burden and keeping the wound clean and moist. Nasal-lining defects most often occur as part of a full-thickness nasal defect, requiring composite reconstruction of nasal cover, structure, and lining. Nasal-lining defects, especially in the lower one-third of the nose, tend to contract, resulting in distortion of the tip and alar unit(s) and compromise of the nasal airway. For these reasons, lining defects are most often repaired using one of the methods detailed later.
General principles of nasal-lining reconstruction
- •
Confirm negative oncologic margins
- •
Determine size and location of nasal-lining defect
- •
Determine whether defects in nasal structure and/or cover are present
- •
Rule out preexisting septal incisions, septal perforation, or evidence of previous inferior turbinectomy that might preclude intranasal local flap repairs of the lining defect
- •
Inject nose, nasal septum, and/or turbinates with local anesthetic (typically 1% lidocaine containing epinephrine)
- •
Inject regional donor sites or involved adjacent facial aesthetic units in subcutaneous tissue plane, as necessary
- •
Consider conservative undermining for small (≤5 mm) lining defects to facilitate tension-free primary closure.
- •
Ensure that all nasal-lining defects are repaired and that composite defects are reconstituted with robust structure to resist contractile effects of wound healing.
Primary closure
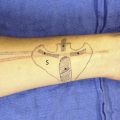
Primary closure is suitable for small (≤5 mm) nasal-lining defects. This technique is best suited for repair of a linear, vertically oriented lining defect ( Fig. 2 ) that lends itself to closure without elevation of the alar margin. Conservative undermining of the nasal lining away from surrounding cartilage or subcutaneous tissue can facilitate tension-free closure. If initial attempts at primary closure result in shortening the nasal lining, elevation of the alar margin or distortion of the nasal valve region another method should be used to repair the nasal lining.
Skin grafts
Full-thickness Skin Graft
Historically, full-thickness skin grafts (FTSGs) have been used for replacement of nasal lining. However, their use in nasal-lining reconstruction is limited by the inability to use FTSGs to cover structural cartilage grafts. FTSGs also have a predilection toward moderate amounts of contraction, which is problematic. Replacement of nasal mucosal lining with skin can interfere with nasal functions, including filtering of pollutants, humidification of inspired air, and mucociliary clearance.
The main indication for use of FTSGs involves reconstruction of the donor site for the bipedicled vestibular advancement flap (see later discussion). The bipedicled flap is used to reconstruct nasal-lining defects of the lower one-third of the nose, creating a nasal-lining defect cephalad to the scroll region/intercartilaginous incision. An FTSG is placed on the perichondrium of the upper and/or lower lateral cartilage(s) to repair the donor site and to prevent contraction and distortion of the reconstructed lower third of the nose.
In theory, FTSGs can be used to reconstitute nasal lining when juxtaposed to the undersurface of a well-vascularized pedicled flap used to replace the nasal cover. This strategy does complicate composite reconstruction because structural cartilage grafts cannot be placed between pedicled cutaneous flaps and an FTSG. Division of the supratrochlear vessel into distinct branches that supply the skin/subcutaneous tissue and the frontalis muscle enables division of the forehead flap into 2 distinct vascularized units. Thus, it is possible to secure FTSGs to the galea/frontalis muscle of a paramedian forehead flap and simultaneously place cartilage grafts into precise pockets between the frontalis muscle and subcutaneous fat of the forehead flap. This method does require secondary/tertiary procedures to debulk the cutaneous flap and add additional structural cartilage grafts to the cephalad portion of the reconstructed nose. In our experience this technique is highly complicated, technically challenging, and risks early contraction of the reconstructed nasal unit(s). Further, large lining defects repaired with this method rely on the blood supply of the frontalis muscle being able to adequately supply both the muscle and the underlying FTSG to ensure survival of the nasal lining and, by extension, the entire reconstruction. Secondary repair of a contracted nasal reconstruction resulting from a nasal-lining deficit can be challenging.
FTSGs consist of the epidermis and variable amounts of dermis. Although FTSGs are subject to less contraction than split-thickness grafts, their higher metabolic demand makes FTSGs survival more tenuous than split-thickness grafts. Skin grafts obtain their nutrition through 3 distinct stages. During the initial 24 to 48 hours, FTSGs obtain nutrients and oxygen via plasmatic imbibition by drinking from the surrounding extracellular fluid. Next, blood vessels in the graft and donor site align and begin to penetrate the graft during the stage of inosculation. Last, vascular ingrowth proceeds and the entire periphery of the graft becomes vascularized. During this critical phase of graft survival, infection and small-vessel compromise (smoking) limit FTSG survival. Thus, antibiotics and smoking cessation are routinely recommended and have been shown to result in improved FTSG survival.
Commonly used FTSG donor sites include pre- and postauricular skin, supraclavicular skin, and the melolabial fold. We prefer to use the preauricular donor site because it provides generous amounts of skin with similar color and texture match with nasal skin. Using the contralateral preauricular donor site allows 2 surgeons to work simultaneously on graft harvest and closure of the donor site and lining defect.
Split-thickness Skin Grafts
Split-thickness skin grafts (STSGs) have higher survival rates as a result of a lower metabolic demand than FTSGs. However, because of their greater predilection toward contraction, STSGs have had limited use in replacement of nasal lining. Nasal-lining defects amenable to skin graft repair tend to be small and thus can be accommodated using common FTSG donor sites with lower risk of contracture.
Cutaneous hinge flaps
Cutaneous hinge flaps are based on a subcutaneous pedicle composed of scar tissue located at the defect margin. The most common donor sites for cutaneous hinge or turn-in flaps are the medial cheek and/or nasal sidewall as well as the cephalic edge of an alar defect ( Fig. 3 ). The hinge flap in the latter case most often consists of the remaining skin of the alar unit, which would otherwise be discarded as part of the cutaneous alar reconstruction. The fact that the vascular pedicle is based on scar tissue at the defect margin limits the potential vascularity of this flap. Delay of the flap, wherein its borders are incised before being re-inset, can improve survival of the cutaneous hinge flap. However, this strategy adds an additional procedure and 3-week delay until definitive reconstruction. Delaying the cutaneous turn-in flap does create an opportunity to inset an FTSG for later use in replacement of nasal lining and/or cover. However, the ability of turn-in flaps resurfaced with an FTSG to adequately cover and nourish structural cartilage grafts is limited. Thus, the use of cutaneous hinge flaps should be reserved for defects in which other options are unsuitable.