Open Correction of Zygomatic Fractures
Warren Schubert
Yeshaswini Thelekkat
DEFINITION
Zygomatic fractures are fractures of the zygomatic bone together with any one or all of its four processes—maxillary, frontal, orbital, and temporal (FIG 1).
When the fracture involves only the temporal process, it is referred to as an isolated zygomatic arch fracture.
More often, fractures involve the adjacent bones through the other processes, and the term zygomatic complex or zygomaticomaxillary complex (ZMC) fracture is more appropriate.
ZMC fractures are also referred to as fractures of the zygoma, malar complex, quadripod, quadramalar, tetrapod, trimalar fractures, and orbitozygomatic fractures.
ANATOMY
The zygoma maintains points of articulation with the maxilla at the zygomaticomaxillary buttress (ZMB or lateral column of the midface) and at the inferior orbital rim (IOR), the frontal bone at the zygomaticofrontal (ZF) suture, the greater wing of the sphenoid at the zygomaticosphenoid (ZS) suture, and the temporal bone at the zygomaticotemporal (ZT) suture.
The ZS component makes up the lateral component of the orbital wall.
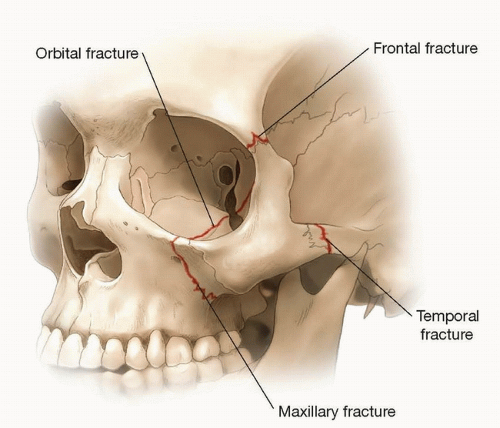
FIG 1 • ZMC showing fracture of four processes of the zygoma— maxillary, frontal, orbital and temporal.
The zygoma also forms a major component of the maxillary sinus, contributing partially to the roof and to the posterolateral wall of the sinus.
The zygoma serves as an attachment for a major portion of the masseter along the body and the zygomatic arch. The arch also serves as an attachment for both the superficial and deep portion of the deep temporal fascia along the zygomatic arch and posterolateral edge of the temporal process. The masseter muscle has a significant role in causing intrinsic deformations of the body and arch1 (FIG 2A).
The zygoma also provides attachment to the muscles of facial animation. These main muscles include the levator labii superioris along the infraorbital rim and the zygomaticus major and minor muscles along the malar eminence.1
The Whitnall tubercle lies on the medial aspect of the zygomatic bone, about 9 mm inferior to the ZF suture and 4 mm posterior to the lateral orbital rim (FIG 2B).2,3 This tubercle provides attachments to the lateral palpebral ligaments and the suspensory ligament of Lockwood, which forms the inferior hammock of the globe.
A key to a successful reduction of the ZMC fracture is the alignment of the zygomaticosphenoidal suture in the lateral wall of the orbit, as this area is least likely to be comminuted.5
Though it is referred to as the zygomatic “arch,” this structure is anatomically closer to being a relatively straight structure in the AP direction, rather than a curvilinear arch.
A fracture of the ZMC is indeed complex as the zygoma helps to define the degree of midface projection and width, as well as contribute to the anatomy defining orbital volume, including the lateral orbital wall and part of the orbital floor (OF).
Malposition of the ZMC can have a significant impact on the function of the eye as well as sensation to the infraorbital nerve.
The various techniques that are described depend on how many points of fixation the surgeon feels are necessary for adequate reduction and fixation.
PATIENT HISTORY AND PHYSICAL FINDINGS
The clinical presentation of the patient is dependent on the direction and strength of the force striking the midface. The patient often presents with a blunting of the malar eminence, which is commonly displaced posteriorly.
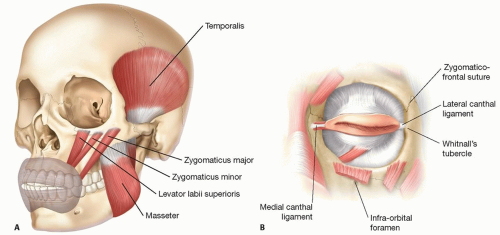
FIG 2 • A. Muscles that attach to the zygoma. B. Position of the Whitnall tubercle relative to the zygomaticofrontal suture with the lateral canthal ligament attached.
Unless the fracture is a pure fracture of the zygomatic arch, all zygomatic complex fractures also result in orbital fractures, commonly of the OF and lateral orbital wall. As the orbit is involved, a complete orbital exam is required to confirm that the patient’s globe and vision have not been compromised.
The surgeon should confirm that the extraocular muscles are functioning, without evidence of entrapment of the extraocular muscles or other periorbital soft tissue.
Diplopia may be due to entrapment or due to other malfunctions of the extraocular muscles or nerves to those muscles.
A forced duction test may be needed to discern the difference between entrapment and malfunction of the extraocular muscles.
Many have claimed to be able to perform a forced duction test adequately under topical anesthesia. We have generally found it necessary to have the patient completely relaxed and sedated to rule out entrapment in the acute phase of facial trauma.
Trapdoor orbital fractures are more common in the pediatric and very young adult skeleton owing to the increased elasticity of the bone. In response to an acute periorbital impact following trauma, the floor fractures, and temporarily bends, resulting in a linear crack. On the release of the force, the floor snaps back into its original position. There may be entrapment of the extraocular muscles and periorbita restricting the movements of the eyeball. There may be minimal signs of edema or ecchymosis externally, and CT imaging may be unremarkable when the volume of tissue entrapped is minimal. These fractures were referred to as “white-eyed blowout fracture” by Jordan et al.6
The patients often present with severe pain on attempted eye movement associated with nausea and vomiting due to an unresolving oculocardiac reflex, which may be misinterpreted as being a primary intracranial injury.
This form of entrapment requires emergent intervention, both for the comfort of the patient and to prevent prolonged muscle ischemia, which can result in a persistent diplopia.
ZMC fractures and the associated OF fractures are commonly associated with impingement on the infraorbital nerve and numbness in that distribution of the midface.
This should be recorded prior to any intervention to avoid postoperative concerns of an iatrogenic injury.
A depression of the zygomatic arch medially may be associated with impingement of the coronoid process, thereby interfering with the movements of the mandible.
This limits the patient’s ability to open or close his mouth, depending on the position of the patient’s mouth at the time of the impact and fracture of the arch and the degree of medial displacement of the arch.
Contact of the arch with the coronoid process may also limit the excursion of the mandible from side to side (FIG 3).
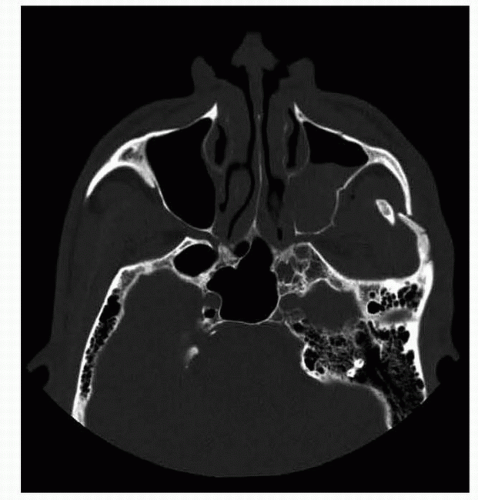 FIG 3 • Impingement of zygomatic arch on coronoid process. |
IMAGING
The appropriate radiologic workup requires fine-cut CT.
The ideal workup includes axial cuts, reformatted coronal cuts, and sagittal cuts through the orbit.
For our sagittal reformatting, we prefer oblique parasagittal cuts through the orbit that follow the axial line of the optic nerve.
In special cases of complex or comminuted fractures, a 3D reformatting may also be very useful.
NONOPERATIVE MANAGEMENT
If the zygoma is fractured, but not displaced, surgical intervention is usually not needed.
In isolated arch fractures, if there is no coronoid impingement or significant cosmetic deformity in the form of a depression on the cheek posterior to the malar eminence, no intervention is usually required.
SURGICAL MANAGEMENT
Steps involved in an appropriate open reduction and internal fixation (ORIF) of a complex zygoma fracture are variable, depending on the clinical findings, CT findings, degree of comminution, and instability of the zygoma.
The technique first described for fixation of a ZMC fracture is that of a standard three-point fixation of the zygoma.
The number of points of fixation needed depends on the degree of instability of the zygoma following fracture reduction.
Preoperative Planning
An exam documenting the patient’s visual acuity, movements of the globe in all directions, presence or absence of diplopia, and infraorbital nerve anesthesia/paresthesia should be included in the preoperative exam.
Adequate preoperative axial fine cuts and coronal and oblique parasagittal reformatted CT of the midface fractures should be part of the routine preoperative workup.
Oblique parasagittal reconstructions in the plane of the optic nerve offer the best single global view of the degree of displacement of the OF (and roof) and can present the surgeon an estimate of the length of material needed if an OF reconstruction is required.
Positioning
Positioning should be supine.
A decision should be made preoperatively as to whether it is necessary to perform a coronal approach, as this will affect the position of the endotracheal tube. For a pure ZMC fracture, a coronal approach is seldom needed.
Availability of intraoperative imaging or navigation also affects patient positioning on the table and the position of the operating table relative to anesthesia providers.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree