6
Oncoplastic procedures to allow breast conservation and a satisfactory cosmetic outcome
Part 1
Volume replacement techniques to improve cosmetic outcomes after breast-conserving surgery
Introduction

A number of prospective randomised trials have compared BCS with mastectomy, showing a survival rate that is unrelated to the type of surgery performed,1–4 although local recurrence (LR) rates smay be higher when the breast is conserved.1
The risk of LR is related to a number of factors, including positive margins, tumour grade, extent of in situ component, lymphovascular invasion and age. Whole-breast section analysis techniques have been used to show the likelihood of complete excision of unicentric carcinomas using different margins of excision (see Chapters 4 and 15).

Local recurrence and cosmetic outcome
The margins of clearance and to a lesser degree the extent of local excision during BCS are strong predictors of subsequent LR.6
The extent of local excision remains a controversial issue in BCS. The wider the margin of clearance, the less the risk of incomplete excision and thus potentially of LR (Table 6.1), but the greater the amount of tissue removed, the higher the risk of visible deformity leading to an unacceptable cosmetic result. This clash of interests8 is most evident when attempting BCS in patients with smaller breast–tumour ratios, for example when planning BCS for a 10-mm tumour in a 200-g breast or a 5-cm tumour in a 700-g breast.
Table 6.1
Technique-related outcomes of breast-conserving surgery
| Quadrantectomy | Wide local excision | |
| Margin (cm) | 2–4 | 1–2 |
| Clearance (%)* | < 90 | < 58 |
| Recurrence (%)† | 2 | 7 |
| Cosmesis | Fair | Good |
The chances of a poor cosmetic outcome are increased still further when the tumour is in a central, medial or inferior location.9,10 Cosmetic failure is more common than generally appreciated, occurring in up to 50% of patients after BCS.11–15 A number of factors are responsible, including volume loss of more than 10–20% leading to retraction and asymmetry, nipple–areola displacement or distortion, the use of ugly and inappropriate incisions, and the local effects of radiotherapy. Volume loss underlies many of the most visible and distressing examples of poor cosmetic outcome and the effects may be compounded by associated displacement of the nipple–areola complex (NAC). Poor surgical technique leading to postoperative haematoma, infection or breast tissue and fat necrosis will increase the amount of scarring and retraction, and add to the risks of deformity. Moreover, the use of suction drains, inappropriate incisions and en bloc resections can worsen the cosmetic result still further.
Role of oncoplastic surgery
1. Oncoplastic techniques allow wider excision of breast cancers without risking major local deformity.
2. The use of oncoplastic techniques to prevent deformity can extend the scope of BCS to include patients with 3–5 cm tumours, without compromising the adequacy of resection or the cosmetic outcome.
3. Volume replacement can be used after previous BCS and radiotherapy to correct unacceptable deformity16 and may prevent the need for mastectomy in some cases of local recurrence when further local excision would result in considerable volume loss.
Choice of oncoplastic technique
The choice of technique depends on a number of factors, including the extent of resection, position of the tumour, timing of surgery, experience of the surgeon and expectations of the patient. Reconstruction at the same time as resection (breast-sparing reconstruction) is gaining in popularity. As a general rule, it is much easier to prevent than to correct a deformity that has developed as the sequela of previous surgery. Immediate reconstruction at the time of mastectomy is associated with clear surgical,17 financial18,19 and psychological20 benefits, and similar benefits are seen in patients undergoing immediate breast-sparing reconstruction after partial mastectomy.
Resection defects can be reconstructed in one of two ways: (i) by volume replacement, importing volume from elsewhere to replace the amount of tissue resected; or (ii) by volume displacement, recruiting and transposing local dermoglandular flaps into the resection site. Volume replacement techniques can restore the shape and size of the breast, achieving symmetry and excellent cosmetic results without the need for contralateral surgery. However, these techniques require additional theatre time and may be complicated by donor-site morbidity, flap loss and an extended convalescence. In contrast, volume displacement techniques require less extensive surgery, can limit scars on the breast and limit donor-site problems. These procedures may be complicated by necrosis of the dermoglandular flaps and contralateral surgery is usually required to restore symmetry as volume loss is inevitable (Table 6.2).
Table 6.2
Comparison of techniques for breast-conserving reconstruction
| Volume replacement | Volume displacement | |
| Symmetry | Good | Variable |
| Scars | Breast + back | Periareolar inverted-T |
| Problems | Donor scar Seroma flap loss | Parenchymal necrosis Nipple necrosis Volume loss |
| Theatre time (hours) | 2–3 | 1–2 (per side) |
| Convalescence (weeks) | 4–6 | 1–2 |
| Timing | Immediate or delayed | Immediate > delayed |
| Mammographic surveillance | Possibly enhanced | Unaffected |
Volume replacement techniques
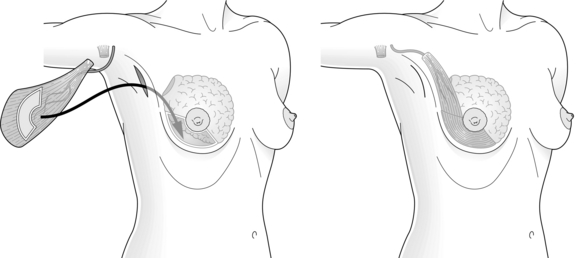
The myocutaneous LD flap carries a skin paddle that can be used to replace skin which has been resected at the time of BCS or as a result of contracture and scarring following previous resection and radiotherapy16 (Fig. 6.1). Although the skin paddle adds to the replacement volume, it can lead to an ugly ‘patch’ effect because of the difference in colour between the donor skin and the skin of the native breast.

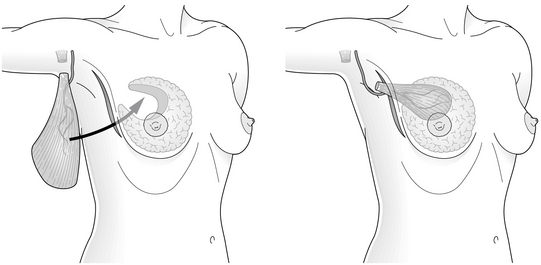
A myosubcutaneous LD miniflap21 circumvents this problem by harvesting the flap in a plane deep to Scarpa’s fascia. This produces a bulky flap without a skin island and includes a layer of fat on its superficial surface that is used to reconstruct defects following wide excision with preservation of the overlying skin (Fig. 6.2).
Perforator flaps22,23 based on thoracodorsal artery perforators (‘TDAP flaps’) and lateral intercostal artery perforators (‘LICAP flaps’) are gaining popularity. They provide skin and subcutaneous fat for volume replacement, are relatively quick to perform, and appear to be associated with a faster recovery and less morbidity than LD flaps. As the LD is relatively undisturbed, the LD muscle can be used for breast reconstruction if a mastectomy is required for a subsequent local recurrence. TDAP flaps are most suitable for lateral and upper pole defects, while LICAP flaps can be used to reconstruct small to medium-sized lateral pole defects. Neither flap can be transposed sufficiently to reconstruct medial pole defects, which are more suitable for reconstruction by an LD miniflap that has been fully mobilised following divison of the tendon, all the serratus anterior branches of the vessels and all remaining fascial attachments to terres major. Other flaps, such as the lateral thoracic adipose tissue flap, have been described24 but their clinical utility is unclear.
Lipomodelling techniques25 have been used to correct rather than to prevent deformity after BCS.26 Stem cells harvested from fat are injected around the defect, into underlying pectoralis muscle and overlying subcutaneous fat, avoiding the breast parenchyma. This helps to avoid the confusing mammographic images resulting from areas of calcified fat necrosis in the vicinity of the tumour bed. The theoretical risk of tumour induction by injected stem cells remains a concern, and has led to the somewhat cautious introduction of this innovative technique into clinical practice.26 Some surgeons have started to use lipomodelling at the same time as wide local excision but no long-term results of this technique have yet been reported.
Non-autologous volume replacement with saline or silicone implants has been tried with mixed success.27,28 Implants can be placed directly into the resection defect or under pectoralis major. They cannot be moulded to fit the resection defect and they form localised capsules, particularly in irradiated tissues. This may interfere with clinical examination and also mammographic surveillance, although there are techniques to allow mammaplasty in breasts with implants and magnetic resonance imaging (MRI) follow-up is an option in such patients. If using implants, low height and low projection implants placed low in the treated breast combined with lipomodelling gives the best results. If there is deformity and significant nipple deviation then a myocutaneous flap is preferred. Autologous tissue transfer is usually the best option for most patients and results in a lifelike breast of normal shape and size.
1. Resection through a radial incision and LD harvest through an axillary incision.29

2. Conventional LD myocutaneous flap harvest for correction of major resection defects.16
3. Resection through a circumferential incision and endoscopic LD flap harvest and reconstruction through an axillary incision.30
4. Resection, LD harvest and reconstruction through a single lateral incision.21
Indications for volume replacement

Resection of more than 20% of breast volume, particularly from central, medial or inferior locations, significantly increases the likelihood of a significant and unsightly local deformity,31 which results in psychological morbidity.32 In these patients, volume replacement can extend the role of BCS and avoid mastectomy when resecting up to 70% of the breast.
Breast conservation with or without reconstruction was formerly reserved for patients with unifocal tumours, but the much wider excision achieved in patients undergoing immediate volume replacement allows resection of multifocal disease with clear margins and excellent local control.33 Volume replacement may be inappropriate in those with more widespread disease or locally advanced T4 tumours. Likewise, LD volume replacement is hazardous in patients with a history suggesting damage to the thoracodorsal pedicle or to the LD muscle, and alternative methods should be considered (Box 6.1). Patients should be informed that using LD for breast conservation precludes its subsequent use for later breast reconstruction. If a mastectomy is required to treat recurrent disease, the options include a variety of free flaps or subpectoral implant-based reconstruction.
Timing of procedures
Immediate reconstruction can be carried out as a one-stage procedure,21,34 which involves simultaneous resection and correction of the resulting defect. This requires perioperative confirmation of complete tumour excision using frozen-section techniques. As an alternative, the procedure can be split into two steps.35 The first step involves excising the cancer and performing a sentinel node biopsy if the nodes are clinically and radiologically normal and the second step includes axillary dissection if required, flap harvest and reconstruction, and is carried out a few days later after confirmation of clear tumour resection margins. Patients undergoing a one-stage procedure must be informed that a mastectomy with or without reconstruction may be required if subsequent histopathological analysis confirms incomplete tumour excision.
Volume replacement with latissimus dorsi miniflaps
There are many similarities between the different surgical approaches used in breast-conserving reconstruction and these can be best illustrated by summarising the main steps involved in LD miniflap reconstruction, which has been described in detail elsewhere.36,37 This procedure involves the use of a myosubcutaneous flap of LD for immediate reconstruction of a partial mastectomy defect, most commonly in the central zone but also in the upper outer and upper inner quadrants of the breast. The term ‘miniflap’ is somewhat misleading, as the flap needs to be of sufficient volume to replace resection defects resulting from the excision of 150–350 g of breast tissue. Moreover, the miniflap needs to be bulky enough to allow for a small degree of postoperative flap atrophy.
Perioperative outcomes
The time required for breast-conserving immediate reconstruction with a miniflap lies somewhere between BCS alone and total mastectomy combined with immediate LD reconstruction. Early postoperative complications include infection, flap necrosis, haematoma formation and transient brachial plexopathy,34 although postoperative stay and disability are similar to other types of BCS. Breast oedema is common, particularly after extensive resection, but usually settles within 6–8 weeks. It may be caused by division of multiple afferent lymphatic pathways during retromammary dissection. Donor-site seroma formation occurs in almost all patients, and can be reduced by ‘quilting’ or delaying drain removal. Flap necrosis is rare, and can be avoided by gentle resection and handling of the pedicle and by taking care to prevent traction and twisting injuries during transposition and fixation of the flap after tendon division.
Late sequelae of volume replacement include lateral retraction of the flap, leading to distortion and hollowing of the resection site, and flap atrophy. Flap retraction can be avoided by division and fixation of the tendon and careful suture of the flap into the resection defect. Detectable flap atrophy occurs in a minority of patients followed for up to 10 years.38 It can be counteracted by over-replacement of the resected volume with a fully innervated flap that has been harvested with a generous layer of subcutaneous fat, by using a myocutaneous flap or by later lipofilling.16
Frozen-section analysis of bed biopsies has been found to correlate closely with the adequacy of excision determined by formal histopathology.33 Moreover, the use of LD miniflap reconstruction leads to a significant fall in the number of incomplete excisions compared with BCS alone24 without compromising the cosmetic outcome. Sensory loss following miniflap reconstruction is minimal compared with the loss following total mastectomy.39 The sensory innervation of the breast and NAC is largely intact, except over the resected quadrant. Finally, volume replacement preserves symmetry, avoiding the need for alterations to the contralateral breast in almost all patients (Fig. 6.3).


Mammographic surveillance
The mammographic appearance of the partially reconstructed breast compares favourably with the appearances after routine BCS. Symmetry is preserved and the fibres of the isodense flap may be detectable, often associated with a variable zone of radiolucency that corresponds to the layer of surface fat. Flaps may be indistinguishable from the surrounding breast tissue, and important radiological characteristics such as skin thickening, stellate lesions and microcalcifications are easily visualised after flap transfer. Volume replacement does not compromise the early detection of LR,40 which typically develops at the junctional zone between muscle and breast parenchyma. The appearance of miniflap on mammograms contrasts with the radiodense distorting stellate scars that are a common source of diagnostic confusion following conventional BCS. Lastly, very few patients develop clinically detectable flap atrophy, with the majority of flaps remaining bulky and functional throughout the period of follow-up.
Future prospects
The role of breast-conserving volume replacement is set to increase as more precise, image-guided resection of specific zones of breast tissue becomes possible. Increasingly sophisticated imaging techniques, such as high-frequency ultrasound and contrast-enhanced dynamic magnetic resonance imaging,41 may in future enable exact delineation and excision of all malignant and premalignant changes. Endoscopically assisted techniques42 may increase the ability to harvest more bulky myosubcutaneous flaps, allowing the reconstruction of more extensive resection defects. This will require the further development of novel techniques for endoscopic dissection,30 including the use of balloon-assisted techniques42,43 and carbon dioxide insufflation to maintain the epimuscular optical cavities. Current progress is hampered by the use of non-flexible straight endoscopes to carry out dissection over the rigid convex surface of the chest wall.
Deformities following breast-conserving surgery
In order to better assess the surgical approach for these patients, a classification of the cosmetic sequelae after BCS has been published by Clough et al.44,45 This simple classification defines three groups of patients based on clinical examination (Fig. 6.4). The advantage of this classification is that it is a valuable guide for choosing the optimal reconstructive technique, but it is also a good predictor of the final cosmetic result after surgery.



Figure 6.4 Deformities after conservative treatment of breast cancer. (a) Type I: a symmetrical breast with no deformity of the treated breast. (b) Type II: deformity of the treated breast, compatible with partial reconstruction and breast conservation. (c) Type III: major deformity of the breast requiring mastectomy. Reproduced from Clough KB, Claude N, Fitoussi A et al. Oncoplastic conservative surgery for breast cancer. In: Operative techniques in plastic and reconstructive surgery. Philadelphia: WB Saunders, 1999; pp. 50–60. With permission from Elsevier.

• Type I deformities: patients have a treated breast with a normal appearance but there is asymmetry between the two breasts.
• Type II deformities: patients have a deformity of the treated breast. This deformity can be corrected by partial breast reconstruction and breast conservation, with the irradiated breast tissue being spared in the reconstruction.
• Type III deformities: patients have a major distortion of the treated breast, or diffuse painful fibrosis. These sequelae are so severe that only a mastectomy can be considered.44
Poor remodelling is one of the reasons for an ugly deformity after lumpectomy or quadrantectomy.46,47 Some surgeons perform no remodelling at all, leaving an empty defect and relying on a postoperative haematoma to fill the dead space. This may produce acceptable results in the short term but breast retraction of larger defects invariably occurs with longer follow-up, leading to major deformities that are increased by postoperative radiotherapy.10,44,48,49

Reshaping of the breast is required after any tumour excision in order to recreate a normal breast shape in one operative procedure. In most cases this can be achieved with a simple unilateral approach, mobilising glandular flaps to close the defect or by recentralising the NAC. In other cases, a bilateral approach incorporating a bilateral mammaplasty will be the only way to perform a wide excision with no deformity.50 This graded approach to breast reshaping is discussed below.
References
1. Fisher, B., Redmond, C., Posson, R., et al, Eight-year results of a randomised clinical trial comparing total mastectomy and lumpectomy with or without irradiation in the treatment of breast cancer. N Engl J Med 1989; 320:822–828. 2927449 A seminal trial (NSABP B-06) showing equivalent overall survival in patients with breast cancer treated either by mastectomy or by lumpectomy and radiotherapy.
2. Veronesi, U., Saccozzi, R., Del Vecchio, M., et al, Comparing radical mastectomy with quadrantectomy, axillary dissection and radiotherapy in patients with small cancers of the breast. N Engl J Med 1981; 305:6–11. 7015141 A seminal trial comparing the treatment of patients with breast cancer by radical mastectomy or quadrantectomy, showing equivalent overall survival in each group.
3. Veronesi, U., Banfi, A., Del Vecchio, M., et al, Comparison of Halsted mastectomy with quadrantectomy, axillary dissection, and radiotherapy in early breast cancer: long-term results. Eur J Cancer Clin Oncol 1986; 22:1085–1089. 3536526 A seminal trial comparing the treatment of patients with breast cancer by radical mastectomy or quadrantectomy, showing equivalent overall survival in each group after long-term follow-up.
4. Abrams, J., Chen, T., Giusti, R., Survival after breast-sparing surgery versus mastectomy. J Natl Cancer Inst 1994; 86:1672–1673. 7966392
5. Holland, R., Veling, S.H., Mravunac, M., et al, Histologic multifocality of TIS, T1–2 breast-carcinomas: implications for clinical trials of breast-conserving surgery. Cancer 1985; 56:979–990. 2990668 A detailed study using serial whole-breast sections to establish the distribution of breast malignancy in relation to the margin of the reference tumour.
6. Dixon, J. Histological factors predicting breast recurrence following breast-conserving therapy. Breast. 1993; 2:197.
7. Veronesi, U., Voltarrani, F., Luini, A., et al, Quadrantectomy versus lumpectomy for small size breast cancer. Eur J Cancer 1990; 26:671–673. 2144153 A seminal trial comparing very wide local excision (quadrantectomy) with limited excision of breast carcinoma (lumpectomy). Quadrantectomy was associated with significantly lower rates of local recurrence when compared with lumpectomy.
8. Audretsch, W.P. Reconstruction of the partial mastectomy defect: classification and method. In: Spear S.L., ed. Surgery of the breast: principles and art. Philadelphia: Lippincott-Raven; 1998:155–195.
9. Pearl, R.M., Wisnicki, J., Breast reconstruction following lumpectomy and irradiation. Plast Reconstr Surg 1985; 76:83–86. 2989962
10. Berrino, P., Campora, E., Sauti, P., Postquadrantectomy breast deformities: classification and techniques of surgical correction. Plast Reconstr Surg 1987; 79:567–572. 3823249
Related posts:
 Psychosocial issues in breast cancer
Psychosocial issues in breast cancer
 Nipple discharge and the role of ductoscopy in breast diseases
Nipple discharge and the role of ductoscopy in breast diseases
 Techniques of mastectomy: tips and pitfalls
Techniques of mastectomy: tips and pitfalls
 Breast reconstruction
Breast reconstruction
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


