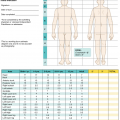
Dressing agent
Active substance
Presentation
Main use
Advantages
Disadvantages
Bacitracin
Bacitracin
Ointment
Superficial burns, skin grafts
Gram + coverage
No Gram − or fungal coverage
Polymyxin
Polymyxin B
Ointment
Superficial burns, skin grafts
Gram − coverage
No Gram + or fungal coverage
Mycostatin
Nystatin
Ointment
Superficial burns, skin grafts
Good fungal coverage
No bacterial coverage
Silvadene
Silver sulfadiazine
Ointment
Deep burns
Good bacterial and fungal coverage, painless
Poor eschar penetration, sulfa moiety, leucopenia, pseudoeschar formation
Sulfamylon
Mafenide acetate
Ointment and liquid solution
Deep burns
Good bacterial coverage, good eschar penetration
Painful, poor fungal coverage, metabolic acidosis
Dakin’s
Sodium hypochlorite
Liquid solution
Superficial and deep burns
Good bacterial coverage, inexpensive, and readily available
Very short half life
Silver
Silver nitrate, silver ion
Liquid solution, dressing sheets
Superficial burns
Good bacterial coverage, painless
Hyponatremia, dark staining of wounds and linens
37.2.1 Synthetic and Biosynthetic Membranes: Suprathel, Biobrane, and PermeaDerm
Alternative treatments for partial-thickness burns have been devised to increase patient comfort, protect against infection, and enhance skin regeneration. The most clinically applicable are the semi-occlusive and synthetic membranes. Re-epithelialization occurs under these dressings, and given that they are only partially occlusive, frequent dressing changes are not required, minimizing distress to the patient. Some are also occasionally utilized as skin substitutes for the temporary coverage of excised full-thickness burns. The most commonly used membranes are discussed below.
Suprathel, a product of Polymedics Innovations GmbH, (Denkendorf, Germany), is a copolymer membrane primarily consisting of DL-lactide as well as ε-caprolactone and trimethylene carbonate. This synthetic membrane is not only easily shaped, but also highly porous and permeable to water. It has an initial porosity over 80%, with interconnected pores between 2 and 50 μm. It is placed on the wound and overlaid with paraffin or non-adherent gauze. As wound re-epithelialization progresses, the membrane peels off, usually over the course of a couple of weeks [17]. Prospective randomized clinical studies have demonstrated that, compared to other commercially available membranes or dressing products, Suprathel decreases pain although it yields similar wound healing times and scar qualities over the long term [17–20].
Biobrane (Smith & Nephew, London, UK) consists of a semipermeable silicone film partially embedded with nylon fabric. In this biosynthetic wound dressing, collagen is chemically bound to a complex 3D structure of tri-filament thread and in this way, comes into contact with the wound bed. The dressing remains firmly attached to the wound, keeps the wound moist, and controls water vapor transfer, facilitating re-epithelialization. Since the 1980s, studies have demonstrated that Biobrane is efficacious in treating partial-thickness burns in children [21–27]. Biobrane can also be utilized for temporary coverage of partial-thickness burns and skin graft donor sites [28]. This product is versatile, relatively inexpensive, easy to store and apply, and safe with low infection rates when used according to the guidelines [29]. Recently, Biobrane has been proven effective for the temporary coverage of deep partial- or full-thickness wounds after debridement, as an alternative to allograft application [30]. Only a few studies have compared the outcomes of different skin substitutes, and no major differences in long-term scar quality have been detected [31]. Thus, burn wound characteristics and cost of treatment are critical factors in the selection of the appropriate skin substitute product.
PermeaDerm (PermeaDerm Inc., Carlsbad, California) is a biosynthetic product approved by the FDA in 2016. This product was developed from Biobrane and designed to serve as a temporary skin substitute in excised full-thickness burns. PermeaDerm is composed of a monofilament nylon-knitted fabric bonded to a thin slitted silicone membrane. The nylon side of this dressing is coated with a mixture of hypoallergenic porcine gelatin and a pure fraction of aloe vera. Biobrane and PermeaDerm primarily differ with regard to pore size and regularity. PermeaDerm consists of numerous rows of slits with parallel orientation on the surface of the dressing for water vapor transmission. This product is unique in that the surgeon can decide how large the pore should be by the strength utilized in stretching the product before applying it. Preliminary studies have shown that PermeaDerm is an effective biologic dressing for the treatment of burns, having variable porosity, major flexibility, and better adherence than Biobrane. PermeaDerm is associated with an overall lower accumulation of fluid and inflammation. When grown on PermaDerm, cultured cells grown have uniform growth, increased migration, and decreased expression of alpha smooth muscle actin and fibronectin. Currently, no human studies have been reported [32].
37.3 Biological Membranes
For centuries, human amnion has been utilized to dress wounds, since the beginning of the last century in the western world. Davis performed skin transplantations utilizing amniotic membrane in 1910 [33]; however, it became apparent that amnion was more suitable as a temporary dressing than a permanent skin transplant. Amnion was first used in burn wounds in 1913. As temporary dressing, amnion has numerous advantages, including low infection rates [34–37], improved wound healing [33, 34, 38], ease of handling [39], and most notably, alleviation of pain. In 1952, amnion was first used of as a temporary skin substitute for burn wounds [40]. Since then, amnion has primarily become established as a treatment modality for partial-thickness burns [36, 38, 41–43].
The number of studies investigating the use of amnion in chronic wounds and burns has steadily increased over the past two decades. Safe and reliable production methods have been pursued to establish amnion as a standard dressing alternative. Several countries have established amnion banks alongside tissue banks in an effort to meet the need [44–46].
The advantages of amnion include its slender form, adhesiveness, pliability, and removability. These qualities are critically important, especially in pediatric populations. Branski et al. compared amnion with standard dressing regimens and found comparable rates of infection, equivalent wound healing, and similar long-term cosmetic results [47]. The authors concluded that temporary wound coverage with amniotic membranes can be safely implemented, with the main benefit being the need for significantly fewer full dressing changes. A recent drive towards the standardization and commercialization of amnion has led to the development of glycerol-preserved forms of amniotic membranes or fresh frozen amniotic membrane (Grafix™, Osiris Therapeutics, Inc.).
37.4 Xenograft
In 1880, Lee first described heterografts [48], now known as xenografts, which are used to provide temporary wound coverage and ensure wound homeostasis. Many species can serve as donors for xenografts although pigs are the most common. Porcine xenografts are typically distributed as a reconstituted product. Homogenized porcine dermis is harvested with dermatomes, fashioned into sheets and later meshed, sterilized via radiation, and finally frozen for storage [49]. Xenografts can be utilized as a stand-alone covering for partial-thickness burns or as an overlay for widely meshed autograft in the same manner as allograft. Porcine xenograft is an adequate substitute for cadaveric skin allograft owing to its structural and functional similarities to human skin, effectiveness in wound protection and pain reduction, ability to limit heat and fluid loss, and prevention of bacterial overgrowth [50–53].
Zawacki et al. showed that early treatment of the wound with a biologic dressing such as xenograft can block necrosis, which occurs in the zone of stasis (i.e., potentially salvageable areas adjacent to burned and irreversibly damaged sites) [54]. Application of xenograft on debrided mid-dermal burns can also sometimes supplant excision and autografting. Additionally, the combination of silver with porcine xenografts has been demonstrated to suppress wound colonization [55, 56]. This semi-occlusive wound dressing creates a moist environment, remains avascular, and can be applied on the wound for more than 7 days. Moreover, it can be supplemented with sulfamylon or silver nitrate soaks for local antimicrobial treatment. Finally, the most common complication of porcine xenografts is fever within 48–96 h after application. This complication generally responds well to antipyretics, cooling, and soaking of the wound.
In addition to pig xenograft, fish skin can be used as a temporary cover for burns and has appeared on the market in the last years. Fish skin is extremely similar to human skin [57] and thanks to the high concentrations of omega-3 fat; it has strong antiviral [58], antibacterial [59], and anti-inflammatory properties [60]. Currently, acellular fish skin is available in the USA and Europe under the commercial name Kerecis Omega3 (Kerecis, Isafjordur, Iceland). Studies support the potential utility of fish skin in treating chronic wounds [61, 62] and burns when compared to amnion/chorion. Magnusson et al. showed that fish skin is more porous and has superior 3D ingrown of cells compared to amnion/chorion [63]. They also reported that bacterial invasion can be prevented up to 48–72 h from application and longer with application of additional omega-3.
37.5 Full-Thickness Burns
Full-thickness burns extend into the deep dermis. These so-called third-degree burn wounds rarely heal within 2–3 weeks. The preferred treatment is complete excision and either temporary coverage or permanent coverage, preferably with autograft. Early surgical treatment with excision of necrotic skin is paramount and has been the favored approach since the 1970s. In patients that have suffered extensive burns covering large areas of the total body surface area (TBSA), there may not be enough donor sites to provide coverage of the excised areas with autograft. In these cases, the burn surgeon should consider using homograft (or allograft) and dermal substitutes.
37.6 Dermal Analogs
For many years , burn research has focused on developing burn wound coverage methods that do not rely on autograft or homograft. That is, a readily available functional composite graft capable of dermal and epidermal replacement has been goal. The development of dermal analogs signifies progress towards this goal.
John Burke from Massachusetts General Hospital and Ioannis Yannas from Massachusetts Institute of Technology teamed to develop Integra (Integra LifeSciences Corporation, Plainsboro, NJ, USA). Integra is composed of bovine collagen and glycosaminoglycans, which permit fibrovascular ingrowth. After full-thickness excision, this dermal analog can be overlaid onto the wound bed, and the wound can then be covered with autograft 2–3 weeks later.
Alloderm is an alternative dermal analog composed of decellularized and de-epithelialized cadaveric dermis (LifeCell Corporation, The Woodlands, TX, USA). It is available for the treatment of full-thickness burns, is used in a way that is very comparable to other dermal analogs, and has exhibited favorable results [64, 65].
37.7 Non-surgical Debridement
Most enzymatic and chemical debridement products introduced thus far have been slow-acting and have been associated with an increased rate of infection because of maceration of necrotic tissue [66]. Recently, a new enzymatic debridement product known as Nexobrid has been introduced for burn wounds. This product incorporates partially purified and lyophilized bromelain into an inert carrier gel. The resultant gel dressing is able to debride burn wounds more rapidly than ever before [67]. Bromelain is a proteolytic enzyme derived from pineapple stems with specific enzymatic activity. Studies have shown that, at 4 h after application of Nexobrid, the burn eschar is removed and a clean wound bed is present [68]. Numerous studies have further shown that, when compared to standard of care for full-thickness burns, Nexobrid produces comparable long-term results and reduces the need for operations [68, 69]. Although Nexobrid is not intended to serve as a substitute for surgical debridement, it represents an extremely innovative and interesting product, especially under circumstances in which surgical procedures are not possible (e.g., on the battle field).
37.8 Negative Pressure Therapy
For almost two decades, negative pressure wound therapy has been used to treat acute and chronic wounds. This therapy is used also for burn wounds. It has been studied for the treatment of acute burn wounds, for bridging to skin graft, as bolster for autograft, as integration for dermal substitutes, and as a donor-site dressing [70]. Application of negative pressure in burns has recently led to the concept of total body wrap in patients with large burns. The idea of creating a total body dressing was first proposed by Genevoc et al., who argued that this approach would have the benefit of creating a sterile environment, securing skin grafts, promoting re-epithelization of donor sites, and removing inflammatory exudates from the burn areas [71]. The utility of this approach has recently been supported by two studies, which concluded that the total body negative pressure therapy is beneficial for healing and patient management and that it may enable one to monitor fluid loss for better resuscitation. However, both studies lacked objective endpoints and the number of patients included was very low [72, 73]. Despite the limitations of these recent studies, total body negative pressure is an interesting approach for patients suffering large burns and will require further investigation before it can be considered a consolidated therapy modality.
37.9 Keratinocyte Coverage
Cultured epithelial autografts (CEAs) are a sensible alternative under circumstances in which patients have massive burn injuries (e.g., >90% TBSA, full-thickness burns) and there is limited uninvolved skin available for coverage, even with the use of an expanding technique. In this approach, two full-thickness sections of unburned skin with a size of 2 × 6 cm are procured promptly upon admission. The samples then undergo processing and ex vivo culturing in the presence of murine fibroblasts, which promote growth (http://www.genzyme.com/business/biosurgery/burn/epicel_package_insert.pdf). Three weeks later, a CEA suitable for grafting is supplied as a 5 × 10 cm sheet of petrolatum gauze that is overlaid with keratinocytes 2–8 cells thick.
Special considerations must be taken into account when managing critically ill patients during manufacturing of the CEA. These include excision and temporary coverage with allograft or xenograft as well as aggressive treatment of complications such as wound infections and multiorgan failure. Execution of the above increases the prospects of survival and ultimately graft take.
CEAs are delicate and have been described as fragile wet tissue paper. Thus, they are difficult to apply. They are also susceptible to shearing and tend to be lost when applied to high stress areas such as the back, buttocks, and posterior lower extremities. Although CEAs are associated with longer hospitalization and the need for additional reconstruction, they provide better cosmetic outcomes than meshed autograft [74]. In recent studies, the outcomes of CEA application have been extraordinarily variable. In a retrospective cohort analysis, more than 30 patients with >75% TBSA burns had excellent survival, and CEAs were retained; however, this study lacked a control group [75]. A graft take exceeding 72% was reported with the combined use of allodermis base and CEA [76].
37.10 Keratinocyte Suspension
Variability in the effectiveness of CEA due to handling difficulties, fragility, and lack of standardized application, as noted by Wood et al. [77], have triggered interest in aerosolized delivery of a keratinocyte suspension. Aerosolized keratinocytes have proven to be an ingenious option in overcoming the limitations of CEAs. Reid et al. used a porcine model to investigate healing of split-thickness-grafted wounds in the presence or absence of aerosolized keratinocytes. They found that the addition of aerosolized keratinocytes significantly decreased contractures after healing ensued [78]. A subsequent clinical trial by James et al. revealed that the addition of aerosolized cultured autologous keratinocytes may assist in the reduction of meshed autograft contraction and decrease healing time [79]. In three-patient case report, Zweifel et al. described decreased hypertrophic scarring and faster healing time with an aerosol of non-cultured autologous keratinocytes, which were applied to split- and full-thickness burns at 2 days after admission [80].
Aerosolized keratinocytes are prepared by incubating a split-thickness skin graft in a 2% dispase solution on a shaking incubator until the epidermal layer is freed. The epidermal layer is then trypsinized to generate a single-cell suspension and expanded in culture over 3 weeks. This yields a final concentration of approximately 107 cells/mL, which can be used to create an aerosol capable of delivering 500,000 keratinocytes to every square centimeter of the wound. Nevertheless, a major shortcoming in the use of aerosolized keratinocytes is delayed application due to the amount of time required for cell expansion.
37.11 Facial Transplantation
Conventional treatment of severely disfiguring facial burns with various techniques and numerous reconstructive procedures typically produces mediocre aesthetic and functional results. In addition to experiencing physical distress and long-term disability, these patients can become socially isolated and may have psychological disorders and phobias. Composite tissue allo-transplantation may improve function and overall quality of life in patients with severe facial disfigurement after thermal, electrical, or chemical burn injuries. Facial transplants can be used to replace nonexistent facial tissue or reconstruct damaged tissue in these patients.
The first face transplantation took place in France in 2005 [81]. Twelve years and over 35 face transplants later, we can safely consider face transplantation an important medical milestone with promising application to the treatment of burn disfigurement. Current facial transplantation procedures have been refined over many years of use during reconstructive surgeries. Successful regimens developed to prevent organ rejection in solid organ transplantation are applicable to facial transplantations.
Clinical protocols for patient selection , procurement algorithms, and surgical techniques have been established, and several prospective studies are currently in progress [82, 83]. Current literature highlights the importance of proper recipient and donor selection. Recipients with a psychiatric history are at higher risk of adverse events. In the selection of the donor, it is critical to follow the established protocols to decrease the risk of rejection, especially in burn survivors who are often sensitized with numerous preformed antibodies [84, 85]. Life-long immunosuppression is a major commitment for patients, with associated risks having been well studied in solid organ transplantation. Pediatric patients are more challenging in this regard. Recent advances in immunomodulatory and immunosuppression agents hold potential for yielding more sustainable treatments. Even though considerable progress has been made in the last few years, facial transplantation is still at an experimental, trial-and-error stage, with many challenges yet to be addressed. Gaining a solid understanding of tolerance and rejection mechanisms, developing effective and safe therapies, monitoring long-term outcomes, assessing cost-benefit, and addressing existing ethical and psychosocial dilemmas are critical for the advancement of facial transplantation from an experimental modality to an established routine treatment for severe facial burns [86–90].
37.12 Tissue Engineering and Stem Cells
Current approaches to promoting wound healing, including skin grafting, are only partially successful. Drawbacks such as poor flexibility, elasticity, and scar production have fueled the search for a skin alternative that more closely recapitulates the histological characteristics of normal skin. A breakthrough innovation in this pursuit has been the combined dermal–epidermal replacement [91]. The combined product is produced by obtaining fibroblasts and keratinocytes from the patient, culturing them ex vivo, and inoculating them onto collagen-glycosaminoglycan substrates [92, 93]. The resulting cell–substrate sheet is cultured in a liquid medium at an air–liquid interface to provide nourishment to the dermal component and expose the epidermal component to air. This generates a keratinocyte layer that undergoes stratification and cornification [94, 95]. Moreover, a new autologous dermal matrix is created through fibroblast proliferation and expansion into collagen substrate and successive degradation within the dermal layer. In vitro production of collagen and formation of a basement membrane at the dermal–epidermal junction [96] increases junctional strength and decreases complications such as epidermolysis and blistering, which commonly occur with CEAs and split-thickness grafts.
Innovations in the engineering of these skin products has created replacements with improved color and cosmetic appearance through the addition of melanocytes and decreased hypopigmentation [97]. Introduction of angiogenic cytokines and vascular endothelial growth factors may assist in accelerating healing, averting graft loss, and overcoming the absence of a vascular plexus [98, 99].
Engineered skin substitutes
Model | Description | Indications |
|---|---|---|
Acellular | ||
Biobrane (Bertek Pharmaceuticals, Morgantown, WV) | Very thin semipermeable silicone membrane bonded to nylon fabric | Temporary adherent wound covering for partial-thickness excised burns and donor sites |
Integra (Integra Life Sciences, Plainsboro, NJ) | Bilayer structure; biodegradable dermal layer made of porous bovine collagen-chondroitin-6-sulfate matrix; temporary epidermal layer made of synthetic silicone polymer | Grafting of deep partial- or full-thickness burns; epidermal layer removed when donor sites available for autografting |
Alloderm (LifeCell Corporation, Branchburg, NJ) | Structurally intact allogeneic acellular dermis; freeze-dried after cells were removed with detergent treatment; rehydrated before grafting | Dermal template for grafting to burns and other wounds; repair of soft tissue defects |
Matriderm (Dr. Suwelack Skin & Health Care AG, Germany) | Non-cross-linked bovine collagen and elastin matrix that allows cellular ingrowth and neovascularization | Template for dermal reconstruction in the treatment of full-thickness burns |
Cellular-allogeneic | ||
Dermagraft (Advanced Biohealing, Westport, CT) | Cryopreserved allogeneic neonatal foreskin fibroblasts seeded on bioabsorbable polyglactin mesh scaffold; cells are metabolically active at grafting | Treatment of full-thickness chronic diabetic foot ulcers |
Apligraf (Organogenesis/Novartis, Canton, MA) | Bilayer; allogeneic neonatal foreskin fibroblasts and keratinocytes in bovine collagen gel | Treatment of chronic foot ulcers and venous leg ulcers; also used for burn wounds and EB |
OrCel (Forticell Bioscience, Englewood Cliffs, NJ) | Bilayer; allogeneic neonatal foreskin fibroblasts and keratinocytes cultured in bovine collagen sponge | Treatment of split-thickness donor sites in patients with burn and surgical wounds in EB |
Cellular-autologous | ||
Epicel (Genzyme Biosurgery, Cambridge, MA) | Autologous keratinocytes cultured from patient skin biopsy, transplanted as epidermal sheet using petrolatum gauze support | Permanent wound closure in patients with burn with greater than 30% TBSA injury and in patients with congenital nevus |
Epidex (Modex Therapeutiques, Lausanne, Switzerland) | Autologous keratinocytes isolated from outer root sheath of scalp hair follicles; supplied as epidermal sheet discs with a silicone membrane support | Treatment of chronic leg ulcers |
TranCell∗ (CellTran Limited, Sheffield, UK) [109] | Autologous keratinocytes cultured from patient skin biopsy, grown on acrylic acid polymer-coated surface; transplanted as epidermal sheets | Treatment of chronic diabetic foot ulcers |
Cultured skin substitute∗ (University of Cincinnati/Shriners Hospitals, Cincinnati, OH) [110–114] | Bilayer; autologous keratinocytes and fibroblasts cultured from patient skin biopsy, combined with degradable bovine collagen matrix | Permanent wound closure in patients with burn with greater than 50% TBSA injury; also used in patients with congenital nevus and chronic wound |
Stem cells participate in the wound healing process and hold potential in the treatment of burn injury. Several local and systematic mechanisms have been defined. Stem cells are present in human adipose tissue, umbilical cord blood, bone marrow, and embryonic blastocystic mass [115]. Use of human embryonic stem cells has raised ethical issues due to destruction of the human embryo. However, stem cells can be isolated from other tissue sources without damaging them, a capability that has propelled research in this field. Stem cells have a number of useful properties that can be exploited such as pluripotency, clonicity, and lack of immunogenicity. These characteristics would allow improved transplantation, re-epithelialization, and dermal regeneration [116, 117].
Studies of bone marrow stem cells have been shown that these cells migrate to injured tissue and facilitate the healing and regeneration process [118–120]. These stem cells are capable of blocking release of proinflammatory cytokines and stimulating expression of anti-inflammatory cytokines (e.g., IL-10) both while they are the bloodstream and after they have arrived at injured tissue [121].
Human embryonic stem cells can be forced to differentiate into keratinocytes while in culture and then stratified into an epithelial graft that is similar to human epidermis [122]. The resulting graft may be utilized as a temporary covering for wounds until an alternative or permanent coverage is possible. This method is currently undergoing initial experimental testing. Alternatively, stem cells can be co-delivered with skin composites or delivered in other ways [123].
Review of stem cell nomenclature
Cell | Source | Potency | Advantages | Disadvantages | Examples of utility |
|---|---|---|---|---|---|
Embryonic stem cells | Inner cell mass of blastocyst | Pluripotent | Pluripotent Clonogenic | Teratogenic ethical controversy | Knockout mouse |
Umbilical cord blood stem cells | Umbilical cord blood | Pluripotent | Pluripotent Non-immunogenic clonogenic | Limited supply with low yield | Bone marrow transplantation |
Mesenchymal stem cells | Bone marrow stroma, blood | Multipotent | Autologous Accessible Clonogenic | Require time to culture Harvest invasive limited supply | Parkinson’s, myocardial remodeling, wound healing |
Adipose-derived stem cells | Adipose tissue | Multipotent | Non-immunogenic abundant supply accessible Clonogenic | Processing required | Wound healing, tissue engineering |
Resident progenitor cells | Numerous tissues/organs | Unipotent | Accessible Potential for transdifferentiation | Limited potency and clonogenicity | Re-epithelialization of wounds from hair follicular cells |
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


