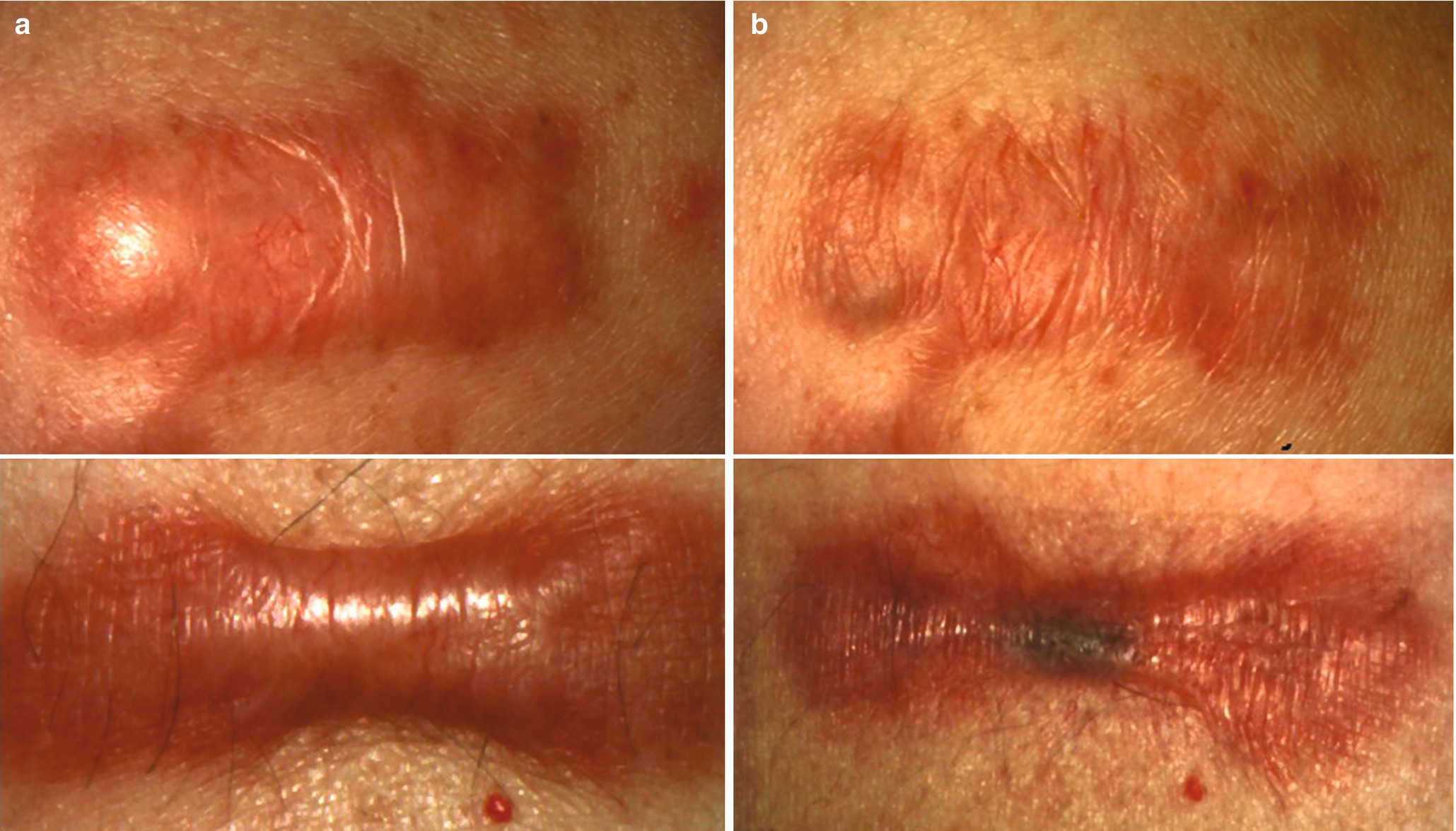
Keloids (upper row) and h ypertrophic scar (bottom row) before (a) and 6 months after (b) four sessions of open spray cryotherapy (two passes of 10 s each) followed by intralesional injection of triamcinolone acetonide (TAC) 40 mg/mL until a blanching effect was reached
Side effects of the TAC injection include dermal atrophy, telangiectasia, and pain at the injection site while cryotherapy is associated with permanent hypo- and hyperpigmentation , blistering, and postoperative pain [1].
38.5.2.2 Intralesional 5-Fluorouracil Injections
5-Fluorouracil (5-FU) has been used for the treatment of hypertrophic scars for decades and positive results were first reported by Fitzpatrick in 1999 after years of use [57]. It is a pyrimidine analog, which is commonly used as an antimetabolite for chemotherapy. In scar tissue, research showed that 5-FU directly increases fibroblast apoptosis by inhibiting the DNA synthesis in rapidly proliferating and metabolizing cells, thus drastically decreasing scar growth [3, 58].
Both high (40–50 mg/mL) and low dose (1.4–3.5 mg/mL) regimens showed positive results in studies evaluating the effects of 5-FU in keloid treatment [59–61]. 5-FU has also been evaluated in combination with TAC. One prospective study including 69 patients showed that a combination of TAC (40 mg/mL) and 5-FU (50 mg/mL) in a concentration of 1:9 injected intralesionally once per week over the course of 2 months, combined with pulsed dye laser treatment, resulted in greater improvements than intralesional TAC (40 mg/mL) alone [62].
Another double-blind, prospective study showed that the aforementioned intralesional regimen was more effective in reducing hypertrophic and keloid scar size and erythema [63]. A current meta-analysis compared the efficacy of combined intralesional 5-FU and TAC to TAC alone and found that 5-FU treatment for hypertrophic scars and keloids resulted in better treatment efficacy, as well as higher patient satisfaction and fewer side effects as TAC treatment alone [64].
Based on current research, intralesional therapy with 5-FU is a safe and effective approach for the treatment of hypertrophic scars and keloids and provides significant scar flattening and symptom control. Erythema and telangiectasia can be treated through adjuvant PDL treatment. Adverse effects include pain at the injection site, hyperpigmentation, skin irritation as well as ulceration, which is mostly seen in darker skin types and commonly resolves within weeks.
Keloids before (a) and 12 months after (b) four sessions of 5-FU (50 mg/mL) and TAC (40 mg/mL), 3:1
38.5.2.3 Laser Therapy
A lot of different laser technologies are available for the treatment of pathological scarring. Nonablative lasers target physiological (hemoglobin, melanin) or artificial (tattoos) pigments while ablative lasers transfer a large part of their energy into water, thus vaporizing tissue and allowing for the controlled ablation of it [65]. Among nonablative lasers, the pulsed dye laser (PDL) has been around for years and its effects have been well researched for a variety of different applications. By targeting oxyhemoglobin, use of the PDL results in capillary destruction, thus inducing tissue hypoxemia which leads to a suppression of profibrotic processes and a supposed upregulation of dermal matrix remodeling through matrix metalloproteases [66, 67]. In a landmark study in 1995, Alster et al. described PDL treatment as an effective option to significantly improve color, height, pliability, and texture in keloids within two to six treatment sessions [68]. These results however could not be reproduced in subsequent studies and follow-up case control studies even reported no discernible differences between treated and untreated scars [69, 70]. Ultimately, further studies revealed that while PDL treatment might not be sufficient to achieve full scar remission, it can be a useful treatment option for fresh, severely erythematous and symptomatic scars or as an adjunct to primary treatment options like intralesional TAC and cryotherapy [35–37].
Side effects of PDL treatment are usually mild and include purpura that last for 1–2 weeks, vesicles, and crusting. Hyperpigmentation can sometimes be observed in darker skin types, but occurrence thereof is less likely with 595 nm wavelength PDL lasers than with units employing a wavelength of 585 nm [37, 65].
The 1064 nm neodymium-doped yttrium aluminum garnet (Nd:YAG) laser has also been suggested for the treatment of keloids and hypertrophic scars [71]. While its mode of action is similar to that of the PDL, the Nd:YAG’s wavelength allows for deeper tissue penetration and its energy is less absorbed by melanin, thus suggesting greater efficacy in darker skin types [65]. In thicker lesions, however, the therapeutic effect might be reduced, as the efficacy decreases with the thickness of the scar [71]. Nevertheless, preliminary studies showed significant improvement pigmentation, vascularity, pliability, and scar height in keloids and hypertrophic scars after five to ten treatments at 1–2 week intervals [72]. A study comparing PDL to Nd:YAG treatment regarding keloids and hypertrophic scars showed both options were effective. Significant differences between the two treatment modalities, however, could not be found [73]. Side effects were usually mild and included a prickling sensation within the treated area and post-treatment erythema [72]. Current research also showed that permanent hyper- and hypopigmentation were less likely with the 1064 nm Nd:YAG than with the PDL in darker skin types [74, 75]. Ultimately though, the effects of Nd:YAG laser treatment on hypertrophic scars and keloids are not well documented enough, yet, thus requiring further research to warrant guideline recommendations for the treatment of excessive scarring [2].
Ablative laser therapy allows for the controlled ablation, excision, and reshaping of tissue. The most common ablative laser is the carbon dioxide or CO2 laser with a wavelength of 10,600 nm. Its energy is strongly absorbed by water and as skin cells are rich in water, the CO2 laser can vaporize tissue in a controlled manner. During treatment, significant heat energy is also transferred into the surrounding tissue. This allows the treating physician to coagulate blood vessels, thus allowing for more extensive tissue ablation. The regeneration and remodeling of heat-damaged matrix proteins also leads to significant skin tightening [65].
Another ablative laser therapy option is the erbium-doped yttrium aluminum garnet laser, also known as the Er:YAG laser. It employs a wavelength of 2940 nm, which leads to significant energy absorption through water. This effect is much more pronounced than with the CO2 laser which results in little to no heat transfer to the surrounding tissue. This effect is sometimes dubbed as “cold ablation.” Thus, tissue ablation with the Er:YAG is less effective, as coagulation of blood vessels is not possible and the heat-induced effects on matrix regeneration and remodeling are much less pronounced [65, 76].
While originally most lasers employed continuous wave technology, that was later replaced in favor of pulsed devices that resulted in strongly reduced heat damage to surrounding tissue, recent modernization of laser technology has led to the development of fractional laser treatment [65]. In fractional laser treatment, the laser beam is divided into a large number of individual laser columns. This creates a pattern of so-called microthermal treatment zones (MTZs), which can reach depths of over 3 mm with the latest laser units. They are interspersed with untreated skin islets. While this results in slightly decreased treatment efficacy, downtime after laser treatment has been greatly decreased through fractional laser treatment [77, 78]. Deep fractional photothermolysis was also shown to significantly influence heat-shot proteins, TGF-β subtypes, and matrix metalloproteases, thus leading to regeneration of a physiological dermal matrix architecture and correction of pathological collagen profiles in scarred skin [79, 80].
Side effects of ablative laser treatment include swelling, erythema, skin infection, scarring, hypopigmentation as well as demarcation between treated and untreated skin.
In scar treatment, fractional ablative laser treatment can be considered as an option to ablate burnt-out linear hypertrophic scars as well as for the loosening of contractures [37, 81]. Studies suggest that the CO2 laser provides superior results than the Er:YAG laser, possibly due to heat-derived effects on dermal matrix remodeling [65]. While this is not critical for the ablation of hypertrophic scar tissue, it significantly limits the lasers ability to improve contractures where modulation of dermal matrix architecture is vital to achieve the desired effects.
Widespread hypertrophic scarring, such as burn scarring, has become a new field for fractional ablative CO2 laser treatment.
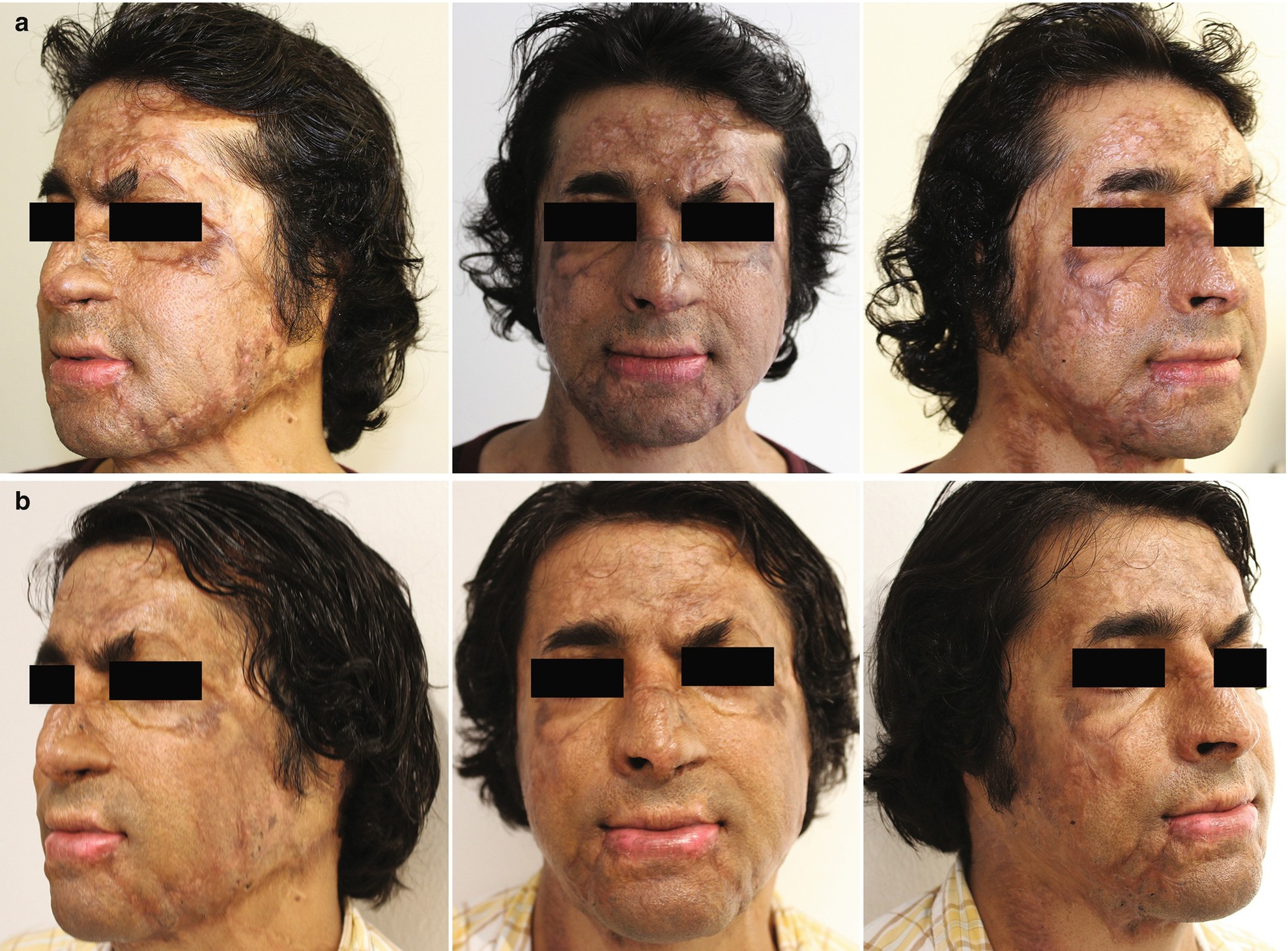
Widespread facial hypertrophic burn scars, before (a) and after (b) three sessions of fractional ablative CO2 laser treatment (Lumenis Ultrapulse Encore) using the aforementioned parameters
Even though recent studies have helped establish the fractional CO2 laser as a safe and efficacious option for the treatment of widespread hypertrophic scarring, further investigation into this method’s potential is necessary to devise standardized treatment paradigms, to elucidate the optimal treatment settings and to determine the ideal point in time for laser intervention.
Keloid treatment with ablative lasers is rarely recommended. Not unlike surgery, monotherapy with ablative lasers results in high recurrence rates. Thus, ablative laser therapy is only recommended for the debulking of large lesions or for the treatment of therapy refractory scars, but only when combined with appropriate adjuvant measures such as intralesional TAC injections or pressure therapy [2].
38.5.2.4 Intralesional Cryotherapy
Intralesional cryotherapy is a relatively new approach for the treatment of hypertrophic scars and keloids. After making a small incision into the scar, the cryoneedle (CryoShape, Etgar Group Ltd., Kfar Saba, Israel) is inserted into the lesion and liquid nitrogen is pumped through the needle resulting in inside-out freezing of the scar tissue.
Initial studies demonstrated significant volume reduction of keloids on the ears, upper back, shoulders, and chest following a single treatment session while also alleviating symptoms like pain and pruritus [95–97]. Additionally, intralesional cryotherapy was reported to be superior to externally applied cryotherapy [98]. Van der Leeuwen et al. report favorable scar reduction and symptom relief, noting, however, that complete scar flattening could not be observed and that both recurrences as well as persistent hypopigmentation in darker skin types were observed [99]. Intralesional cryotherapy requires special equipment and the ability for sterilization of the needles after treatment, thus generating high costs. As its clinical efficacy still requires elucidation through further studies, no clear recommendations on its use for the treatment of hypertrophic scarring and keloids can be made thus far.
38.5.2.5 Surgery
Surgical excision remains a standard option for the treatment of hypertrophic scars and keloids. It should however be considered carefully. As hypertrophic scars often show spontaneous regression without further treatment, care should be taken to avoid unnecessary surgery [50]. On the other hand, hypertrophic scarring caused by excessive tension can be operated on early to treat the origin of the hypertrophy by employing tension-relieving techniques such as z-plasty, w-plasty, skin grafting, or local flaps [1, 2]. Hypertrophic scar recurrence after revision surgery is rarely observed [100, 101]. Keloids on the other hand should not be operated on without adjuvant therapy like intralesional TAC injections, pressure therapy, or radiotherapy, as recurrence rates for surgical monotherapy range from 50 to 100% [18]. Patients treated with keloid excision are at danger of developing an ever larger keloid post-surgery [55]. Therefore, surgery is usually only recommended as a last resort option or for the debulking of larger lesions when combined with proper adjuvant measures. Good results are generally reported for the surgical excision of ear-keloids when treated with pressure earrings immediately after full reepithelialization is reached. Cosmetic results are usually satisfying and recurrence rates are low [1, 3, 102].
38.5.2.6 Radiotherapy
Radiotherapy has mainly been used as an adjuvant treatment option after surgical removal of keloids. Its mode of action is based on the inhibition of vascular budding and fibroblast proliferation, which results in decreased collagen synthesis, thus limiting the growth of fresh scar tissue.
Employing X-rays, electron beam, low- or high-dose-rate brachytherapy after surgical excision, good results regarding recurrence rates could be observed in a number of studies [103–105]. Van der Kar et al. however concluded that surgical excision of keloids in combination with postoperative radiotherapy should be reserved as a last resort option as their prospective study observed a recurrence rate of over 70% [106]. A meta-analysis on the efficacy of radiotherapy treatment for keloids concluded that radiotherapy after surgery was more effective than radiotherapy alone, while brachytherapy resulted in the lowest recurrence rates (15%) when compared to electron-beam or X-ray radiotherapy [107].
Common side effects of radiotherapy include hypo- and hyperpigmentation as well as erythema, telangiectasia, and skin atrophy [108]. In regard to the potentially carcinogenic side effects of ionizing irradiation, radiotherapy should be considered carefully, especially in younger patients and in sensitive areas [101].
38.5.2.7 Bleomycin
Bleomycin sulfate is a glycopeptide and commonly used as a systemic chemotherapeutic agent. Since bleomycin inhibits collagen synthesis by decreasing TGF-β1 levels, it has been adapted for the intralesional treatment of excessive scarring.
A number of studies have since shown significant improvement of scar parameters like height, pliability, erythema as well as symptoms like pain and pruritus in hypertrophic scarring and keloids after three to five treatment sessions [109–111]. Combination of TAC and bleomycin for intralesional keloid and hypertrophic scar treatment also revealed significant effects in a small case series [112].
Side effects include long-term depigmentation and dermal atrophy and when applied systemically, its high toxicity may lead to serious effects on the pulmonary, renal, and hepatic organ systems among others. As with intralesional 5-Fluorouracil injections, however, systemic side effects have rarely been reported and are extremely unlikely in strictly intralesional use [101]. Overall, however, research data on bleomycin treatment for excessive scarring is still scarce, thus necessitating further investigation of its therapeutic efficacy to establish its role in the treatment of hypertrophic scars and keloids.
38.5.2.8 Interferon
Interferon (IFN) has been considered for the treatment of excessive scarring based on its antiproliferative effects that lead to decreased synthesis of collagen subtypes I and III. Interferon-α2b has been identified as the most promising compound for its properties that may help improve dermal fibrosis directly or by antagonizing the effects of TGF-β1, -β2 and histamine [113, 114].
Systemic administration of IFN-α2b could be shown to improve clinical appearance of hypertrophic burn scars and lowered serum levels of TGF-β were observed following treatment, while intralesionally applied IFN-α2b (1.5 million international units, injections twice per day over the course of 4 days) resulted in a 50% reduction of keloid size within 9 days in one study, with researchers claiming superior efficacy of IFN- α2b when compared to intralesional TAC [114, 115].
IFN treatment, however, goes along with frequent side effects including flu-like symptoms and injection site pain [101]. IFN therapy is also significantly more costly than other, more common forms of scar treatment. So far, while remaining a promising treatment option, guidelines for the treatment of pathological scarring have not yet included IFN treatment, as sufficient research data on its efficacy is currently not available.
38.5.2.9 Recombinant TGF-β3
Recombinant TGF-β3 was initially believed to be a potent upcoming option for the treatment of excessive scarring. While adult skin tissue is characterized by a balance of TGF-β isotypes with higher levels of fibrosis stimulating TGF-β1 and TGF-β2, fetal skin tissue shows heightened expression of TGF-β3 which induces anti-fibrotic changes during wound healing, as well as dermal matrix remodeling. This is assumed to play a pivotal role in the ability of fetal skin to heal almost scarlessly [116, 117]. But while initial results of placebo-controlled, double-blind phase I and phase II studies on the effects of recombinant TGF-β3 reported promising results, the subsequent phase III trial failed to hit its endpoints and development of the drug was ultimately halted [118]. While no treatment options based on recombinant TGF-β3 are available right now, research on this promising aspect of wound healing and its potential clinical applications continues [119–121].
Summary Box
Pathological scarring includes a variety of different subtypes that go along with tantalizing aesthetic and functional impairments and that remain difficult to treat successfully. As surgical interventions become more common in the developed world and trauma is ubiquitous, physiological as well as disturbed scarring is a global occurrence. Therefore, physicians require a basic understanding of the pathophysiology of scarring and knowledge about the most common therapeutic options, their potential as well as their side effects. While many of the most established interventional regimens like surgery and intralesional corticosteroid injections have been tried and tested throughout years of clinical application, a variety of once promising emerging options have now become established as standard forms of therapy and earned their place in treatment guidelines [36, 37]. Among them are the intralesional injection of 5-Fluorouracil for keloid treatment as well as the fractional ablative carbon dioxide laser treatment for widespread hypertrophic scarring. Undoubtedly, more options will follow, as researchers continue to evaluate new forms of scar treatment all the while reevaluating established treatment paradigms to reassess their role in current scar therapy. In this regard, the role of objective imaging and questionnaire based scar evaluation is becoming more and more important to ensure optimum treatment efficacy for every patient [122].
Related posts:
 of Burn Patients to the Burn Center Including Burn Wound Evaluation
of Burn Patients to the Burn Center Including Burn Wound Evaluation
 Care of the Burned Patient
Care of the Burned Patient
 Management of Facial Burns, Acute Versus Long-Term, Surgical Versus Non-surgical Face Transplant
Management of Facial Burns, Acute Versus Long-Term, Surgical Versus Non-surgical Face Transplant
 Management of Burn Patients and Fluid Resuscitation
Management of Burn Patients and Fluid Resuscitation
 Care in Burns
Care in Burns
 Reconstruction: The Role of Integra in the Dorsum Hand and Wrist Reconstruction
Reconstruction: The Role of Integra in the Dorsum Hand and Wrist Reconstruction
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


