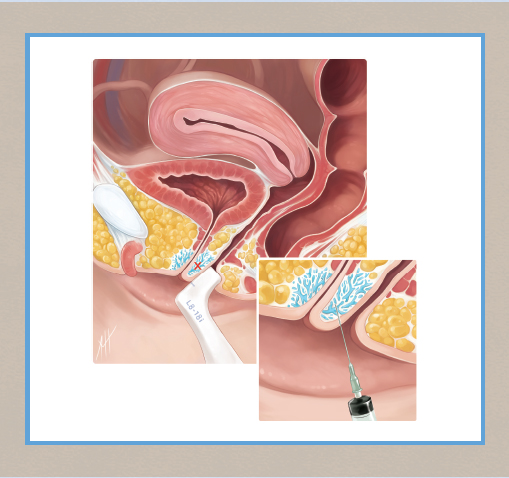
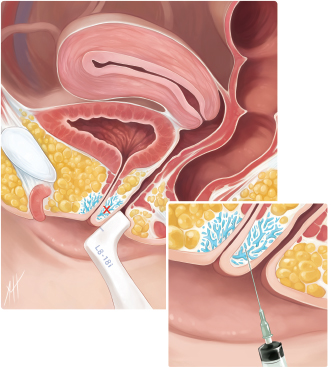
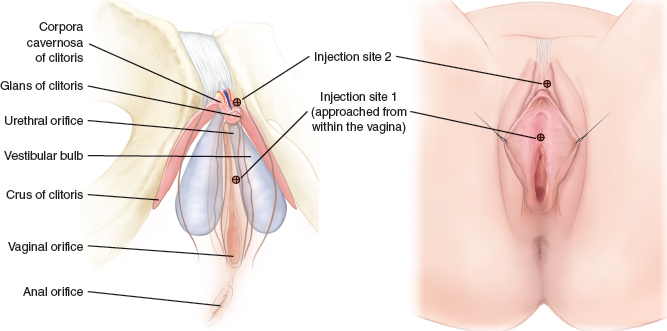
CHAPTER 15 • The treatment of female sexual dysfunction calls for new therapies that directly affect the female genitalia. • Specifically placed injections of platelet-rich plasma (PRP), the O-Shot® procedure, offer promise for female sexual dysfunction, lichen sclerosus, and urinary incontinence. • Because the definition of the “G-spot” by some authors can be nebulous or functional rather than anatomic, and because anatomic descriptions may describe an area different from what we intend for the location of the injection, we propose the name “O-spot,” for the most distal place between the urethra and vaginal wall, as a way of unequivocally defining one of the locations for the injection of PRP. • The treatment of female sexual dysfunction has advanced so that the same systems analysis used to understand pathophysiology for other systems (such as respiration and digestion) seems warranted. Therefore the term “female orgasm system” is proposed as a useful concept. • As more effective sexual therapies become available, the ethics of who can decide when “good” is “good enough” could become relevant. Approximately 40% of women have psychological distress from female sexual dysfunction, whereas only 14% of women—during their entire lifetime—will consult a physician about sex.1 The main reason for the lack of communication about sex between women and their physicians may be that physicians avoid the conversation, thinking that solutions are few; therefore discussions are futile.1 As late as the 1980s, researchers advised urologists to become “primary [psycho-] therapists” to treat erectile dysfunction (ED), because “most instances of acquired impotence” were thought to be “psychogenic.”2 The FDA approved more than 20 drugs to help men with ED, after research demonstrated that most cases of ED arose not from psychological causes, but instead from neurovascular and endocrine disorders.3 Or, did new therapies addressing neurovascular causes of ED facilitate better understanding of the cause?3 Conversely, for women, the class A drug therapies for FSD currently include only “short-term” testosterone and the one drug approved by the FDA for FSD, flibanserin.1,4 No FDA-approved drug for FSD directly targets the female genitalia.1 Flibanserin affects women by altering serotonin and dopamine levels with no direct effect on the genitalia, placing the drug in the same class as an antidepressant. Furthermore, no form of testosterone for women is currently approved by the FDA. Because the clitoris is analogous to the penis in anatomy and physiology,5 and because men have sexual dysfunction secondary to penile pathology (for example, from autoimmune disease, decreased circulation, or loss of sensation), then future treatments for women that might directly address pathology of the genitalia are plausible. Because phosphodiesterase inhibitors (PDEIs) help men with sexual dysfunction, the same strategy could seem plausible for women. However, on closer examination of the benefits PDEIs provide men, the crossover seems less promising with this class of drugs. Although PDEIs improve firmness of the penis by altering hemodynamics, they do little to correct the pathophysiology that necessitates their use.6 This shortfall prompted a call for therapies that correct the primary causes of erectile dysfunction.6 Moreover, the simple achievement of the mechanical state of rigid cavernosi through increased tumescence would directly solve a problem for men (the need for a penis rigid enough for sexual intercourse) but at best would only secondarily correct female sexual dysfunction, because a rigid clitoris solves no particular female sexual dysfunction. Nor do rigid corpus cavernosi primarily solve the male sexual dysfunctions that are analogous to those found in women (decreased libido, decreased sensation, pain with intercourse, or decreased ability to orgasm). Nevertheless, even though erect corpi would not directly solve any particular female sexual dysfunction, the idea showed promise in some studies, although they showed “significant increases in adverse events compared to placebo.”7 Furthermore, even though the treatment of FSD often requires the use of psychological and endocrine modalities, the extension of that idea—that therapies directly affecting the female genitalia offer little benefit—seems limiting and unlikely. For example, a woman may not enjoy benefit from a drug directed toward the brain if she has scarring from an episiotomy or from lichen sclerosus, pain from pelvic floor tenderness, or anorgasmia from diabetes with neurovascular compromise of the clitoris. Therefore more class A therapies (drugs and procedures) for women directed to the pathology of the female genitalia are needed. A subset of women with FSD (1 of 20) has female orgasmic disorder: either difficulty achieving or complete inability to experience orgasm.1 Successful treatment of orgasmic disorder not only improves a woman’s sexual pleasure but also can improve her emotional bonding, mental health, and relationships.4 Although testosterone therapy can facilitate female orgasm (partly by maintaining the integrity of the vaginal nerve fiber network and muscularis volume while enhancing genital blood flow and mucification), women who cannot use testosterone or who already have normal levels of the hormone have only psychotherapy as their primary class A treatment.1,8–10 All drug strategies, including flibanserin and testosterone, are off label—not approved by the FDA—for the treatment of female orgasmic disorder. Medications provide few options for improving female orgasm; thus the available procedures are considered. Hyaluronic acid (HA) gel and collagen have been injected into the G-spot to enhance orgasm in women by facilitating increased pressure on the G-spot during sexual intercourse; but these therapies were not designed to treat sexual dysfunction (only to improve normal function) and are not known to propagate the repair of tissue.11,12 Moreover, because erosion, urinary obstruction, and pulmonary embolus are risks in women undergoing HA enhancement of the G-spot, the American College of Obstetrics and Gynecology published a position paper to discourage physicians from providing the procedure.13–15 Similarly, the FDA approved calcium hydroxyapatite crystals (Coaptite) for injection near the urethra for the relief of urinary stress incontinence, but such use risks foreign body granuloma formation resulting in erosion or obstruction, requiring surgical correction in about 1 in 40 women.16,17 Although still FDA approved for urinary incontinence, Coaptite is neither indicated nor suggested as a treatment for FSD.18 The idea of injecting material near the urethra to improve sexual function or to stop urinary incontinence has been discussed for more than a decade. The challenge has been to find a material that provides therapeutic benefits without unacceptable adverse effects.19 A new and exciting treatment involves the use of PRP to enhance female sexual function.20 In contrast to the above-mentioned synthetic materials, PRP has been shown to have no serious adverse effects and to be effective in multiple studies for the treatment of soft tissue wounds and joint injury and for orthopedic and dental surgery and a variety of cosmetic procedures.21–23 Pluripotent stem cells exposed to PRP activate and develop into new tissue—nerve, collagen, and blood vessels.24–26 Moreover, the medical literature contains many articles demonstrating the safety of PRP, with no reports of granuloma formation, infection, or any other serious adverse effects when the laboratory equipment used has been approved by the FDA for the preparation of PRP for use in the body.26,27 PRP is even used to treat scarring and to restore atrophied tissue; the possibility of causing scarring from PRP is theoretically impossible.28,29 Because PRP is aqueous, it flows easily through a small-bore needle (for patient comfort with only local anesthesia) and is evenly distributed (which prevents the need for the meticulous positioning of the needle required for injecting an HA gel or a calcium hydroxyapatite crystal slurry).30 A pilot study was conducted to determine the effects of specifically placed, localized injections of PRP for the treatment of FSD, the O-Shot procedure.30 As described in this chapter, the in-office procedure takes about 15 minutes. First, a topical anesthetic is applied to the introitus and clitoris. Whole blood is then drawn from the arm and processed at the bedside to extract PRP using a kit approved by the FDA for PRP preparation for injection back into the body.31,32 With the woman in a lithotomy position, 4 ml of her PRP is activated with 0.2 ml of 10% calcium chloride and injected into the O-spot—the space between the urethra and the vaginal wall, most distally, in the area of the periurethral glands (Figs. 15-1 and 15-2). One milliliter of activated PRP is injected into the clitoral corpus cavernosum, near the glans clitoris. Fig. 15-2 Endovaginal placement of the hockey-stick–shaped 18 MHz ultrasound probe shows a urethral curvilinear echo, with circumferential periurethral smooth muscle and areolar tissue between the urethra and vagina in the area of the O-spot (X). Ultrasound images obtained during and after the O-Shot procedure demonstrated hyrodissection of the area by the injected PRP.
O-Shot®
Charles Runels
Key Points
Injection of Autologous Platelet-Rich Plasma for Female Sexual Dysfunction
Orgasms: More and More Intense
Related posts:
 Augmentation of the Labia Majora With Fat Grafting
Augmentation of the Labia Majora With Fat Grafting
 Augmentation of the Labia Majora With Fillers
Augmentation of the Labia Majora With Fillers
 Perineoplasty and Vaginoplasty
Perineoplasty and Vaginoplasty
 Informed Consent and Liability in Cosmetic Genital Surgery
Informed Consent and Liability in Cosmetic Genital Surgery
 Transcutaneous Temperature-Controlled Radiofrequency for Vulvovaginal Rejuvenation
Transcutaneous Temperature-Controlled Radiofrequency for Vulvovaginal Rejuvenation
 Anatomy and Classification of the Female Genitalia: Implications for Surgical Management
Anatomy and Classification of the Female Genitalia: Implications for Surgical Management
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


