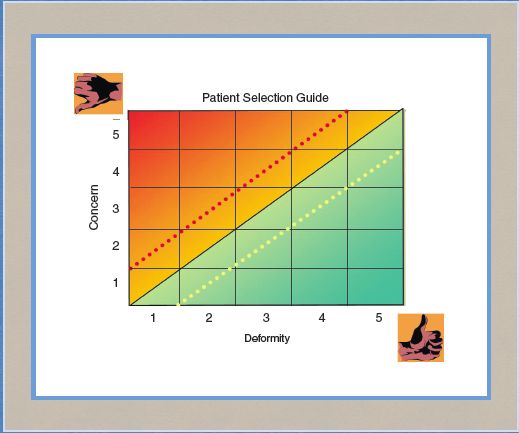
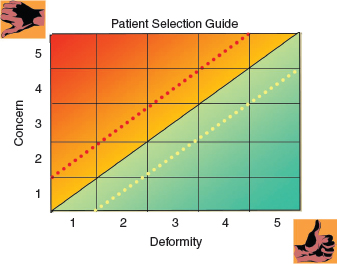
CHAPTER 3 • Appropriate patient expectations are essential. • Patient goals should be realistic for the procedure. • Informed consent is a process, NOT the signed paper. • Surgeons should be honest in their disclosure about the effects of new procedures. The basic medicolegal issues include elements of a tort, informed consent, the definition of damages, and specific financial and warranty issues. Most female patients seeking aesthetic surgery of their genitalia do so electively. This has an impact on tort law, which establishes four elements for a tort claim: • A duty to treat the patient • A breach of that duty • Proximate cause • Damages The first element to establish in a medical negligence claim is a duty to treat the patient. This duty may begin once a patient is accepted into the practice. Therefore realistic expectations and appropriate timing for surgery are essential. The second element is a breach of that duty. This may include what has been described as the battle of the experts. A standard of care is defined with difficulty and suggests the appropriate level of care that a reasonable physician would use to treat a patient. A standard of care comprises many methods, all of which are acceptable, although different physicians might select different methods. When choosing procedures and a treatment plan, it is always helpful to consider peer-accepted procedures. If a new procedure or method is contemplated, it should be fully discussed with the prospective patient so that it is not perceived as experimenting in a new area. The third element, proximate cause, establishes that the breach of action or inaction is directly responsible for damages. This is also known as the “but for” element in that but for the action or inaction, damages would not have occurred. The last element is damages. This can be confusing for physicians in that complications of healing may occur that resolve with no additional residual scarring, yet damages are claimed. Damages, depending on state law and jurisdictions, may include pain and suffering, loss of consortium, secondary and additional surgery, and delayed healing to name a few. It may be safe to assume that damages will be present should a breach of care occur. The more elective the surgery, the more careful the practice should be in accepting patients whose expectations and goals are reasonable and achievable. Failure to meet expectations and financial considerations are the main reasons lawsuits are filed. It behooves a practice to spend an appropriate amount of time explaining, demonstrating, and providing visual aids to help patients make an informed decision about proceeding. I have always suggested that physicians, when possible, accept patients they “like” and in whom they will be able to provide a desired result. This may be difficult to achieve after only one visit. Prospective patients should be accepted only after they are seen at least twice, and surgical decisions are made. Surgery in this anatomic area has many inherent risks and possible complications, which may occur even after the best care is provided. The general consent basically should include scarring, infection, bleeding, dyspareunia, nonhealing, the possible need for additional surgery and revisions, and less than desirable results. One trend of plaintiffs is to initiate a lawsuit because of an inherent risk such as a scar or a known complication. Surgeons should be careful beginning with the initial consult and throughout care to not imply, “This won’t happen to you, but I have to talk about it.” Evaluating and understanding additional patient risks that may interfere with care are essential. These include smoking, nutritional changes from dieting and weight-loss procedures, the effects from supplemental over-the-counter medications, and noncompliance with postoperative instructions and activity restrictions. Patients should be informed about the risks of noncompliance. Surgeons may say, “I can no longer be responsible for your outcome if you do not follow recommended instructions.” All patients should sign a revision policy. The consent should clearly state the requirement to comply with preoperative and postoperative instructions and explain that noncompliant patients will be responsible for the cost of any additional surgery. For instance, labiaplasty patients who smoke before or after surgery are at a very high risk for wound complications. These patients should sign a revision policy stating that they will be required to pay for any revision surgery. Surgeons who describe in advance a complication that occurs postoperatively are often thought to be very smart; however, the same information provided after the complication occurs is often seen as an excuse and is not well accepted. The best advice I can offer is to discuss the benefits of a procedure versus the inherent risks and complications that may occur, while ensuring the patient’s goals are realistic. This process should be carried out over the course of several patient visits. Informed consent is a critical component of a lawsuit and essential for patient happiness. Risk managers speak of informed consent, recognizing its importance, yet it is rarely the sole basis of a successful lawsuit. Cardiovascular studies suggested that patients understand and retain approximately 35% of what is discussed in a consultation.1 However, these data are old, and by presenting information in a manner to accommodate patients’ main learning styles—visual, auditory, and kinesthetic—rates of retention can be much higher. Through a collaborative effort of the surgeon, coordinator, nurse, and others, a practice can benefit by presenting a story of expectations for auditory learners, diagrams and photographs for visual learners, and specific examples of possible interactions for kinesthetic learners. The more all three are included in the informed consent process, the better a surgeon’s understanding of the patient’s expectations and the ability to achieve them, and the better the patient’s understanding of acceptable risks and complications. The informed consent process should be documented in an educational style and not in a legalese style. An appropriate amount of time should be allotted for questions and answers and to acknowledge that the patient understands what can, and especially what cannot, be achieved and that no results can be guaranteed. This cannot be accomplished in one visit, at the end of which the patient signs the reflection documentation, which is informed consent reflecting what has been discussed in this “process.” Some patients never understand the informed consent process, whereas others do so after the second practice interaction. For those who do not understand, wise surgeons will not schedule surgery, but rather continue providing “nonselling” information, helping the prospective patient balance her goals and understanding. The process must be explained in part by the surgeon who will perform the surgery. The practice nurse or coordinator can assist but cannot thoroughly discuss and answer surgical questions. Because of the varied anatomy of the genital area, new procedures, or more commonly variations of standard techniques, are necessary to achieve the best cosmetic results. Patients need to be informed of asymmetrical incisions such as those made for a unilateral double fold of the labia minora. A review of preoperative pictures (taken with the patient in a lithotomy position) is an important step with all cosmetic genital patients. The potential location of scars should be pointed out to patients before the surgery. Before performing a new procedure or a variation of a standard technique, an experienced surgeon might say to a patient, “I am relying on my clinical experience and training.” This is a reasonable statement, even though the procedure is one that is commonly performed. Often, such new procedures are variations of commonly performed, acceptable procedures that add a level of comfort for the surgeon and the patient. However, surgeons must disclose that this procedure is new. A suggested statement is: “This is a new and accepted procedure but certainly within my clinical training.” The procedure should be based on sound, peer-reviewed, and accepted knowledge and articles. Arguably, a totally new procedure should have the patient safety of an Institutional Review Board. Variations of procedures using acceptable surgical technique may not require IRB involvement. This does not, however, obviate the need for a well-documented discussion of the procedure, experience related to it, risks, hazards, realistic goals, and alternatives. Failing to include such a discussion may lead to a patient, now a plaintiff, saying, “I never would have agreed to the procedure if I knew it was experimental and the doctor had no experience.” The patient’s reasons and goals should be discussed. Failed expectations, a common reason for lawsuits, may arise when a patient does not thwart her husband’s affair, rekindle romance, or achieve marital bliss. Through frank and open discussions during the informed consent process such desires may be revealed. Rarely does a surgical intervention adjust or correct marital or relationship problems. If a patient discloses that her reason for desiring surgery is to improve her marital sex relationship and overall intimacy and nothing is documented to dispel such a goal, an implied warranty may inadvertently be created. Once surgeons or team members hear information about an expectation that may not be achieved, they have a responsibility to state “that may not happen,” and there are no warranties concerning the comment. Failing to dispel the stated expectation may create an implied warranty. Surgeons should be careful in advocating this new, exciting surgical field; appropriate patient selection with appropriate, achievable goals is essential. Additional issues relating to informed consent include financial considerations. A clearly written, explicit financial agreement is needed that outlines costs, including the surgeon’s fees, facility fees, anesthesia fees, lab pathology costs, and other expected and unexpected costs. A revision policy covering a finite period of time that the patient acknowledges in advance is advisable. I recommend that no additional surgical fees be included for necessary revisions within 1 year of surgery, provided that the patient complies with all scheduled follow-up instructions and visits. Additional fees for the facility and anesthesia may be necessary. This varies with each practice. What is important is that even if a surgeon waives revision costs, the patient may incur additional charges. Patients who do not follow instructions, miss appointments, smoke against medical advice, and create additional risks will not benefit from such a revision policy. Surgeons can benefit from understanding warrantee issues. Two types of warranties may be established: express and implied. An express warranty is an exhibit, such as a photograph, drawing, or something demonstrative included in the record. It establishes what a patient thinks will be her expected result. When this result is not achieved, this express portion of the medical record possibly creates a breach of warranty. Therefore care is required in using visual aids to describe incisions, scars, and handling of issues to avoid implying that it is the expected result. When discussing photographs and schematics of results, surgeons should not imply that they show how all patients heal and results all patients achieve. Schematics showing a range of results and scarring should be discussed with patients to help them understand possible results, as opposed to implying results. An implied warranty may be established if a patient discloses a specific goal or desire, and the surgeon knows that it may be difficult to achieve. For example, a patient discloses she has a very important business trip to a beach resort 2 weeks after surgery. Hearing this goal and not documenting a discussion with the patient of the difficulty of achieving it and the need to reschedule the surgery may establish an implied warranty that the patient will be able to attend this business meeting. Breach of warranty usually is not covered by general malpractice insurance, and it does not require negligence for a successful claim. The requirement is that a warranty is established and was not met. At least with a medical negligence claim, the defendant has an opportunity to prove that care was not negligent. A warranty should not be established, because only the warranty failure is needed to prove the claim. Expectations and goals are critical in understanding a patient’s desires and outside influences from partners and others. This surgery involves a large emotional component. A discussion with patients about their reasons for seeking such a surgery helps to determine their possible reaction if areas of nonhealing or additional scarring occurs. Surgeons should be very careful with patients who demand procedures or results that are either unrealistic or outside of an acceptable range. Accepting a patient, taking the patient’s money, and operating on the patient for what may be a substandard result only because the patient wanted it is not acceptable. I have often stated that a patient cannot consent to a negligent procedure. A surgeon’s responsibility and duty are to protect patients sometimes from themselves. Occasionally, a young labiaplasty patient will request a labiaplasty even though in a physical examination she has small labia minora. These patients should not undergo surgery, because the scarring and risks outweigh the potential cosmetic improvement. This may even result in not accepting patients regardless of how willing and demanding they are. We earn our living by patients we care for and our reputation by those we do not. Surgeons must be mindful of having a chaperone always present during an examination. This even applies to female plastic surgeons and female patients. A patient’s family member, female or otherwise, is not an acceptable chaperone. Should any abnormal or false complaint arise, it becomes their word against yours. Privacy and communication issues have risen to a much higher concern in protecting patients’ information data and confidentiality. Having a communication agreement that outlines how patients may be contacted, including via mail, email, home phone, work phone, cell phone, and/or social media, is essential. This consent for communication should be updated frequently and patient requests followed. If a patient’s result is suitable to show to prospective patients, not only a HIPAA general consent is needed, but also a commercial HIPAA consent. This commercial consent should describe specifically where the photograph will be used, in what context, and for how long. It is absolutely necessary that the data embedded in the photograph be scrubbed, preventing any internal knowledge of the patient’s identity. Ongoing privacy concerns should apply throughout the office, including all staff protecting the medical record, and even in public, should a patient be encountered in a social setting. I have told my patients that I will not be rude but will not acknowledge I know you to protect your privacy. There are risks in every area of plastic surgery. Gorney and Martello2 wrote significantly about balance between deformity and risks. His “Gorneygram” in Fig. 3-1 shows higher risks in treating patients with minimal deformities. Prospective patients with greater deformity and less concern (represented in the right lower side of the chart) tend to do much better than patients perceiving their minimal deformity as huge (represented in the upper left area of the chart). Caution is suggested when caring for patients whose balance of deformity and concern lies in this upper left area. This should be considered when counseling and treating patients seeking cosmetic improvement of the female genitalia. Although patients may have significant underlying emotional pressures, the proper procedure with improved results can be most satisfying.
Informed Consent and Liability in Cosmetic Genital Surgery
Neal R. Reisman
Key Points
Basic Medicolegal Issues
Medicolegal Issues Inherent in Surgery of the Female Genitalia
Related posts:
 Fractional Erbium Laser for Vaginal Rejuvenation
Fractional Erbium Laser for Vaginal Rejuvenation
 Labia Majora Reduction Surgery: Majoraplasty
Labia Majora Reduction Surgery: Majoraplasty
 Anatomy and Classification of the Female Genitalia: Implications for Surgical Management
Anatomy and Classification of the Female Genitalia: Implications for Surgical Management
 Psychological Issues and Social Mores in Female Genital Aesthetic Surgery: What Is Normal?
Psychological Issues and Social Mores in Female Genital Aesthetic Surgery: What Is Normal?
 Transcutaneous Temperature-Controlled Radiofrequency for Vulvovaginal Rejuvenation
Transcutaneous Temperature-Controlled Radiofrequency for Vulvovaginal Rejuvenation
 Anatomy and Classification of the Female Genitalia: Implications for Surgical Management
Anatomy and Classification of the Female Genitalia: Implications for Surgical Management
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine
