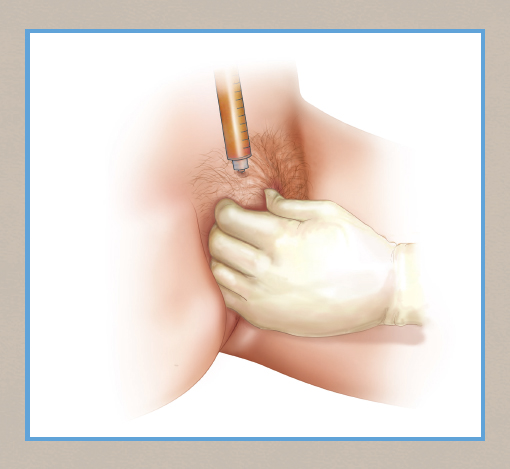
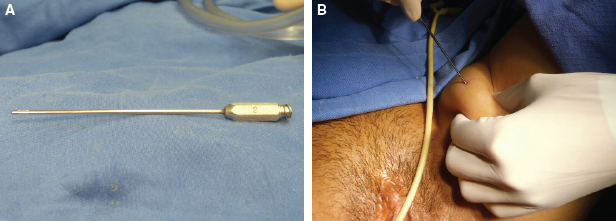
CHAPTER 8 • The main indications for augmentation of the labia majora are hypoplasia, loose skin, or both. • If the labia majora are very “baggy” with significant excess skin, then excisional labia majora reduction should also be considered. Treatment options include autologous fat grafting and the use of dermal fillers. • When performing only fat grafting in patients with a lot of loose skin, surgeons should not place too much fat in the inferior third of the labia majora. Patients who desire a lot of fullness should be informed that more than one procedure needs to be performed. The aim of this chapter is to describe a nonsurgical approach to labia majora augmentation with autologous fat transfer. This procedure may be performed alone or in conjunction with other aesthetic external genital surgical procedures to enhance results. In today’s society we are more aware of genital appearance because of the current vogue for the minimal pubic hair appearance and the increased discussion in the media and popular press.1 In particular, smooth and prominent labia majora may provide a more youthful appearance to the female genitalia. Women today mostly seem to desire the youthful appearance of concealed labia minora and full, smooth labia majora. Techniques that return fullness to the labia majora are therefore important in cosmetic surgeons’ armamentarium for addressing the external genital. Autologous fat transfer, through lipomodeling, is a well-described technique to enhance the appearance of the labia majora and an important procedure in vulvar plastic surgery.2,3 The main indications for augmentation of the labia majora are hypoplasia, loose skin, or both. Labia majora hypoplasia and/or laxity has several causes, and these may be classified as congenital or acquired. Acquired causes include changes secondary to trauma or tumors but also physiologic causes such as aging and those associated with menopause or changes during pregnancy. Massive-weight-loss patients may also present with significant bagginess and loss of volume. Many younger patients with otherwise seemingly “normal” labia majora may desire only puffier, fuller labia majora, because this may be perceived as an aesthetic ideal. There are no significant contraindications for augmentation to this area. Surgeons must warn patients of potential infection, but this risk is no greater than with any other female genital surgery. In very thin patients with minimal fat deposition, lack of a good donor area may be considered a relative contraindication, and surgical planning and discussion with the patient is paramount in these circumstances. The anatomy of the female external genitalia has been described in Chapter 1. Embryologically, the labia majora in women are derived from the genital swellings that, in the male fetus, develop into the scrotum.1 They are two cutaneous specialized skin folds that extend posteriorly from the mons pubis; they become wider than the labia minora anteriorly and start to narrow posteriorly.3 They enclose the internal structures of the female genitalia, especially in nulliparous women, although the anatomic appearance may vary widely. The labia majora have a hairy outer face and an inner face that lacks hair and has a finer skin for cutaneous annexes and semimucosal glandular cover. The labia majora are naturally filled with subcutaneous fatty tissue to varying degrees. The blood supply to the labia majora is from the posterior labial artery and the perineal artery, both branches of the internal pudendal artery. The nerve supply arises from the pudendal nerve. Cosmetic genital surgery is no different from the rest of our aesthetic plastic surgery practice; thus listening to patients is of paramount importance. The motivation for presentation should be discussed in detail, including perceived expectations and understanding of the complications. The examination is then performed. We recommend patients use of a mirror while in the lithotomy and standing positions so that their concerns can be pointed out and conveyed effectively. Careful documentation of the anatomy, including any variations, should be encouraged for medicolegal purposes. If the labia majora are very “baggy” with significant excess skin, then excisional labia majora reduction should also be considered (see Chapter 6). The discussion and decisions about the degree of filling with fat should be similar to those involving breast implant sizing. The decisions should be made after listening carefully to the patient to understand the end result she desires. We must always inform patients that some amount of fat will be resorbed after labia majora lipomodeling. The Coleman fat transfer technique has been well described.4 Surgeons often have their own personalized technique for harvesting, preparing, and injecting fat according to available equipment and personal preference. The procedure can be performed with the patient under local anesthesia in an office setting, depending on local regulations in each country. No blocks are needed. If fat grafting alone is performed, then we recommend marking the area with the patient in the lithotomy position. A long, oval-shaped outline is drawn, starting at the level of the outer introitus and extending to the level of the pubic prominence (2 to 3 cm above the distal upper part of the clitoral hood). The fat graft can be taken from an area where it is available in excess. Areas such as the inner thighs and inner knees are easily accessed, because they are in the proximity of the area to be filled. The area to be liposuctioned for obtaining the fat graft is also marked, and tumescent solution may be injected in the subcutaneous tissue, according to normal practice. Our tumescent solution is prepared using 500 ml saline solution, 1 adrenaline ampule (1:1000), and 25 ml 1% lidocaine (Fig. 8-1). Usually, about 80 to 120 cc of fat may be obtained by liposuction using 10 ml syringes or approximately three times as much fat as planned for use in the fat graft. We prefer to use a 1.8 to 2.0 mm cannula for extracting fat. This same cannula can be used to apply the tumescent solution if required. Several techniques have been described to harvest and process the fat such as centrifuging, washing and straining, and decantation (Fig. 8-2).
Augmentation of the Labia Majora With Fat Grafting
Lina Triana, Paul E. Banwell
Key Points
Why Perform Augmentation of the Labia Majora?
Indications and Contraindications
Anatomy
Clinical Evaluation and Planning
Surgical Technique
Markings
Harvesting the Fat Graft
Related posts:
 Fractional Erbium Laser for Vaginal Rejuvenation
Fractional Erbium Laser for Vaginal Rejuvenation
 Augmentation of the Labia Majora With Fillers
Augmentation of the Labia Majora With Fillers
 Perineoplasty and Vaginoplasty
Perineoplasty and Vaginoplasty
 Informed Consent and Liability in Cosmetic Genital Surgery
Informed Consent and Liability in Cosmetic Genital Surgery
 Transcutaneous Temperature-Controlled Radiofrequency for Vulvovaginal Rejuvenation
Transcutaneous Temperature-Controlled Radiofrequency for Vulvovaginal Rejuvenation
 Anatomy and Classification of the Female Genitalia: Implications for Surgical Management
Anatomy and Classification of the Female Genitalia: Implications for Surgical Management
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine
