6 Nose
Summary
This chapter focuses on subunit reconstruction of nasal defects. Nasal subunits are important in preoperative planning for reconstruction and can guide treatment decisions. We discuss the importance of cartilage grafting as well as reconstruction of internal nasal lining in defects that involve such components. Specific attention is also given to larger defects that require transposition flaps such as melolabial and paramedian forehead flap reconstruction.
Keywords: nasal subunits, ala, paramedian forehead flap, septal lining, melolabial flap, composite graft, columella, skin graft harvest
 Introduction
Introduction
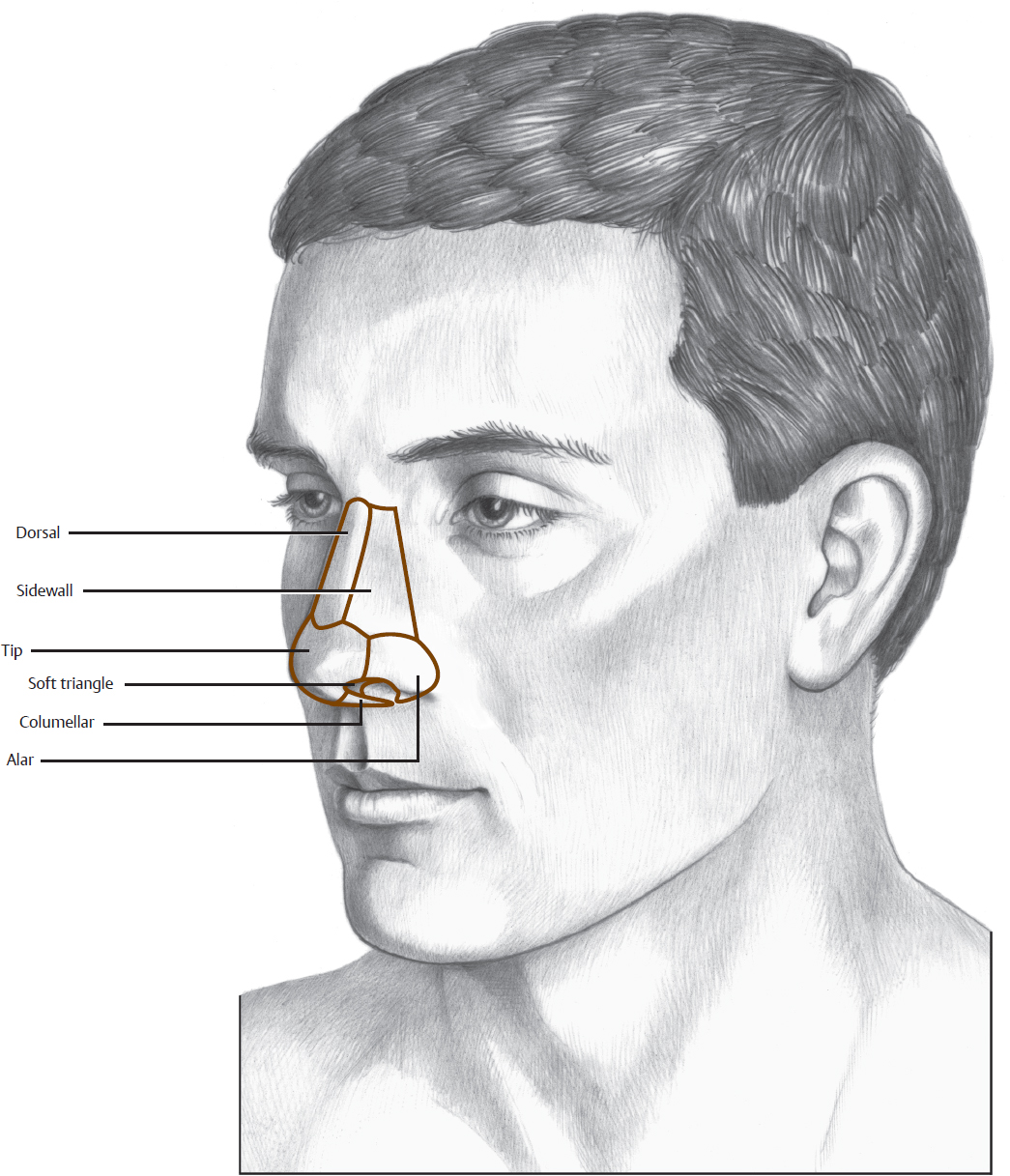
The complex contours of the nose reflect the underlying structure and variations in the thickness of the skin/soft tissue envelope. In general, the three layers of the nose—skin, bony or cartilaginous framework, and mucosal lining—should each be reconstructed separately. The skin itself is thick and sebaceous over the nasal tip and ala, and thin over the nasal dorsum and sidewalls. Th e skin is more mobile over the superior two-thirds of the nose. The shapes of the nasal bones, dorsal septum, and upper lateral cartilages define the shape of the upper two-thirds of the nose. The shape and strength of the lower lateral cartilages primarily define the shape of the tip. The summation of all these factors creates the nasal aesthetic subunits (Fig. 6.1).
These aesthetic subunits have shadowed valleys and lighted ridges at their natural boundaries. The nose can be divided into nine subunits: two sidewalls, dorsum, two alae, tip, two soft tissue triangles, and columella. The medial canthal area is considered in this chapter as the superior aspect of the sidewall subunit. Incisions in the subunit boundaries along relaxed skin tension lines or in the midline of the nose heal with less perceptible scars.
Because the subunits tend to be either somewhat convex or somewhat concave, reconstructions are least noticeable when they assume these same configurations. For example, the pincushioning frequently seen with melolabial flaps can be an advantage when reconstructing the convex ala. When defects assume most of an aesthetic subunit, it is better to resect the remainder and to reconstruct the entire subunit as a totality.
Defects frequently do not follow clear schemata and may involve parts of several subunits. It is occasionally desirable to combine different techniques for these complex defects, using a different flap or graft for each of two aesthetic subunits. In difficult cases, where the defect involves only skin and subcutaneous tissue, a full-thickness skin graft (FTSG) alone can be used to resurface a large area with an acceptable, though not optimal, result. The forehead flap, however, is used for reconstruction of most significant nasal defects.
Pincushioning or a “trapdoor deformity” can result from even well-designed flap repairs on the nose. Wide undermining of the nasal skin–soft tissue envelope in the plane just superficial to the periosteum and perichondrium, as well as flap incisions in the same deep plane, will help to avoid the problem at the time of primary surgery. If pincushioning does occur, it is treated early in the postoperative course with a subcutaneous steroid injection. A typical injection is 0.2 to 0.3 mL of triamcinolone acetate (10 mg/mL). These injections are begun as early as 3 weeks postoperatively and repeated at monthly intervals, as needed. In some cases, secondary revision with defatting and wide undermining may be necessary, but it is usually delayed for 6 months to allow maturation of the wound.
 Dorsal and Sidewall Subunits
Dorsal and Sidewall Subunits
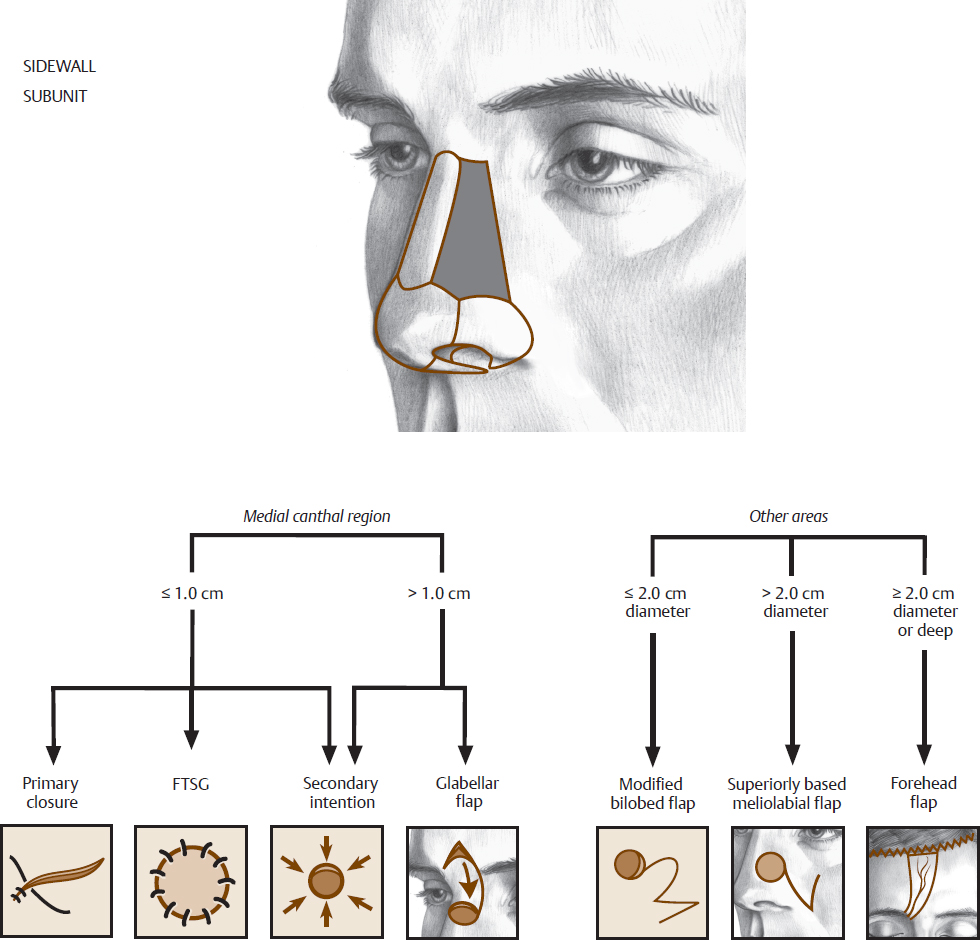
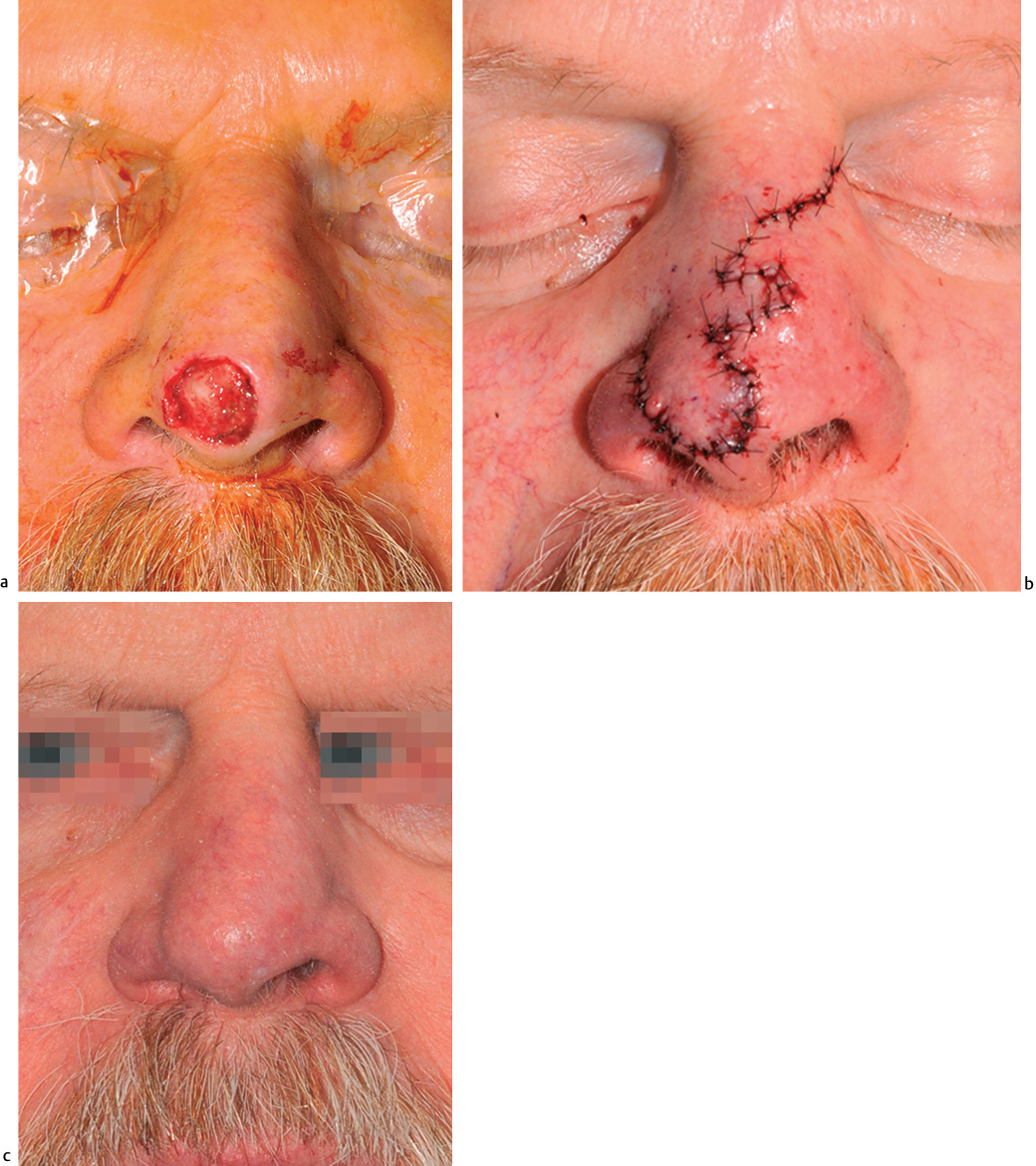
Skin-only defects of the dorsum and sidewall can be repaired using an FTSG with adequate, though sometimes suboptimal, results (Fig. 6.2 and Fig. 6.3). Healing by secondary intention works well only in the medial canthal area. Secondary intention healing is most appropriate for defects whose geometric center is approximately at the level of the medial canthus on the nasal sidewall. Defects that are centered below the medial canthus may heal with contraction of the lower lid. Similarly, defects centered above the medial canthus may heal with contracture of the upper eyelid.
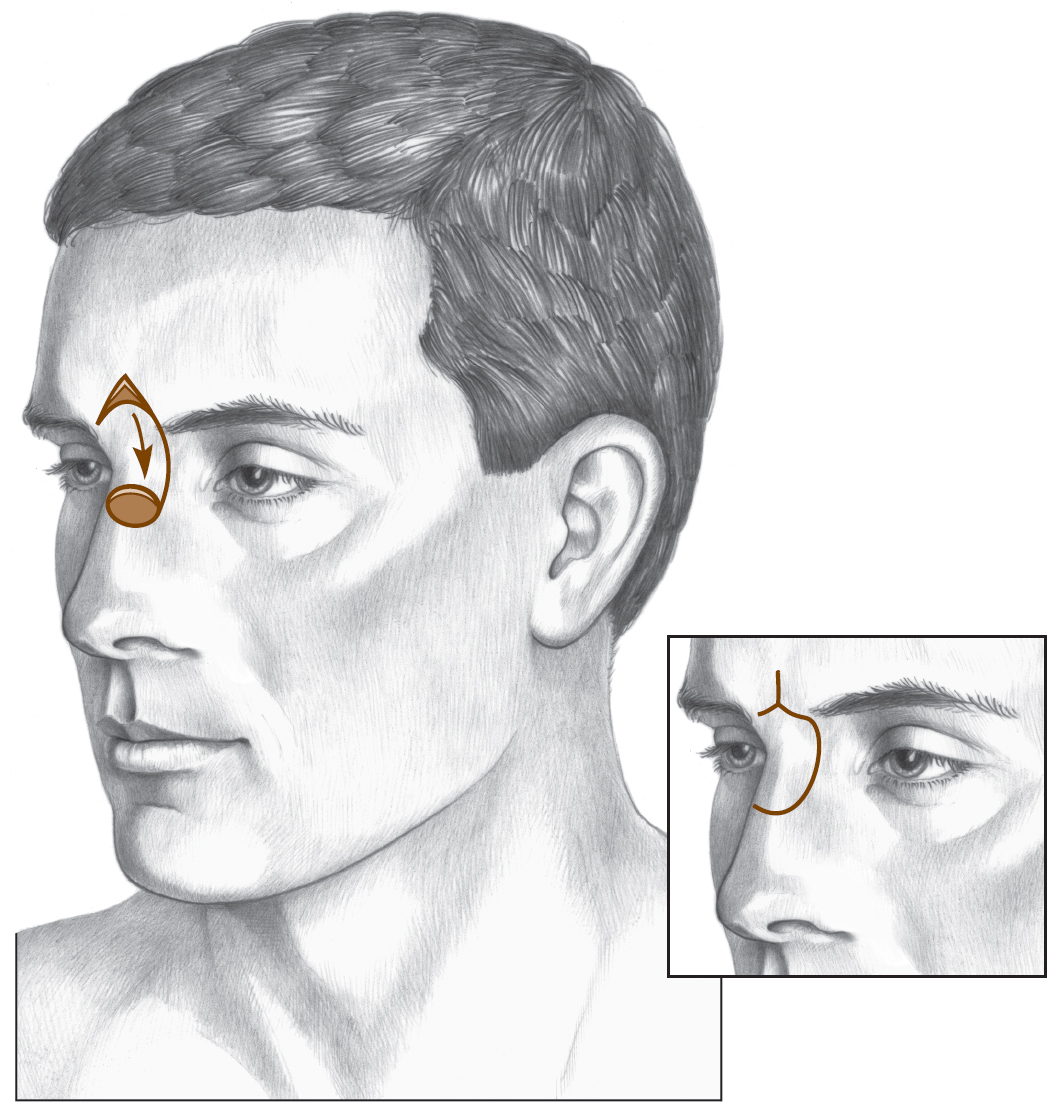
For defects that are more superior or horizontally oriented, the glabellar rotation flap can be used (Fig. 6.4 and Fig. 6.5). This flap requires significant length of incisions and a large mobilization of tissue for a relatively small defect, but the incisions are well camouflaged.
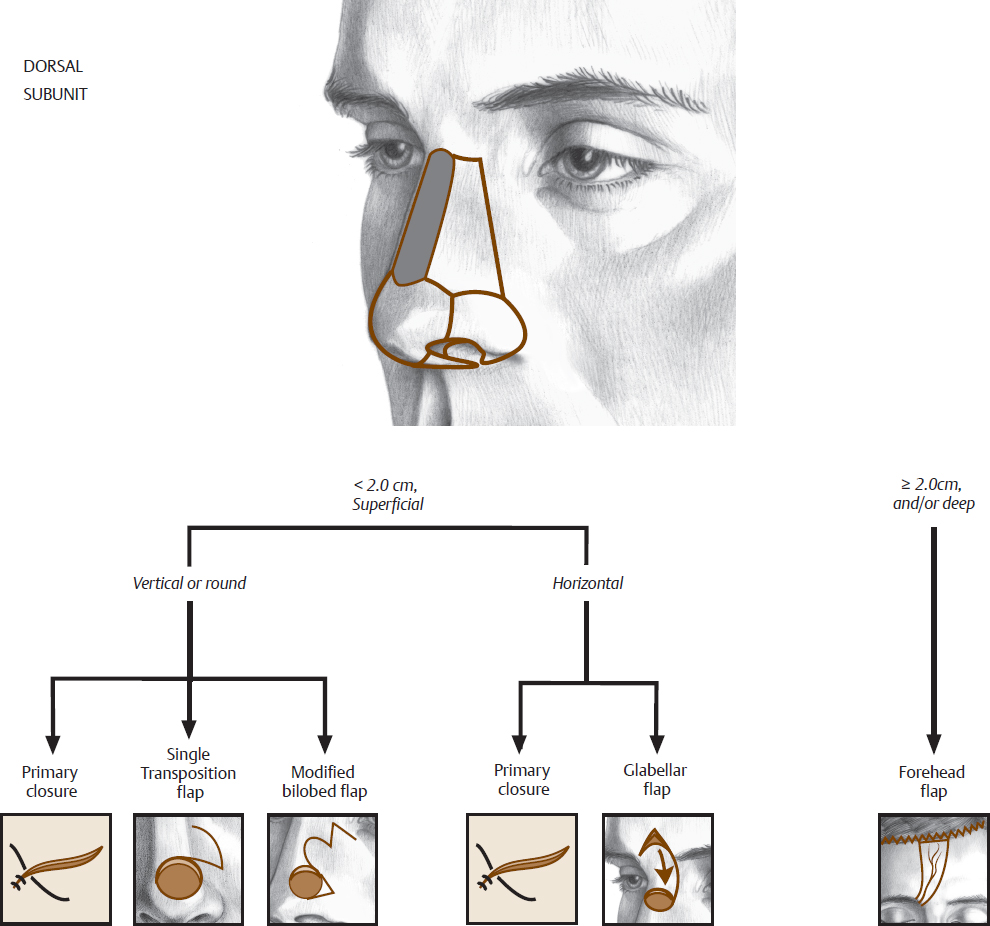

Small defects of the dorsal midline can be closed primarily or with single or double transposition flaps. Primary closure can be accomplished in either the vertical or the horizontal plane, as long as it does not result in distortion of the nasal tip or ala (Fig. 6.6). Single transposition flaps are planned so that the closure site is placed in the alar crease when possible (Fig. 6.7).
Flap closure can occasionally be facilitated by removing a preexisting dorsal hump after elevation of the skin–soft tissue envelope. If the closing tension of a single transposition flap causes alar elevation, then a double transposition flap (bilobed) is selected.
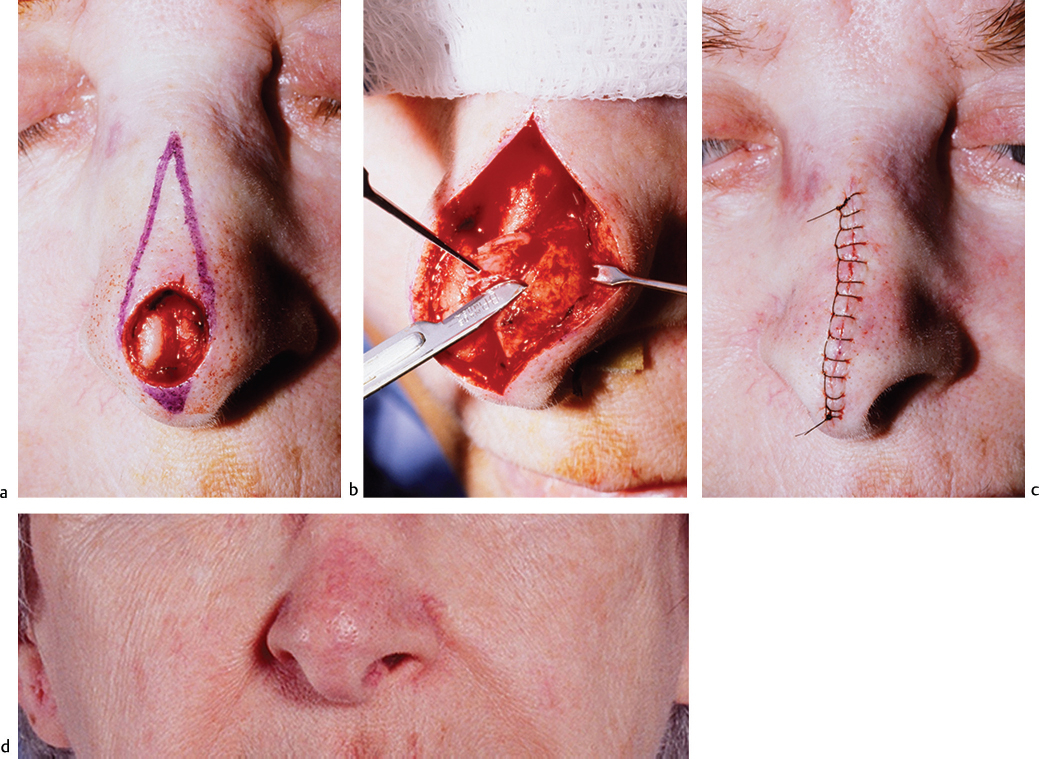
Fig. 6.6 (a) Planned primary closure of a midline nasal defect with dog-ear excisions. (b) Tip cartilages are shaved to facilitate primary closure. (c) After closure. (d) Late postoperative result.
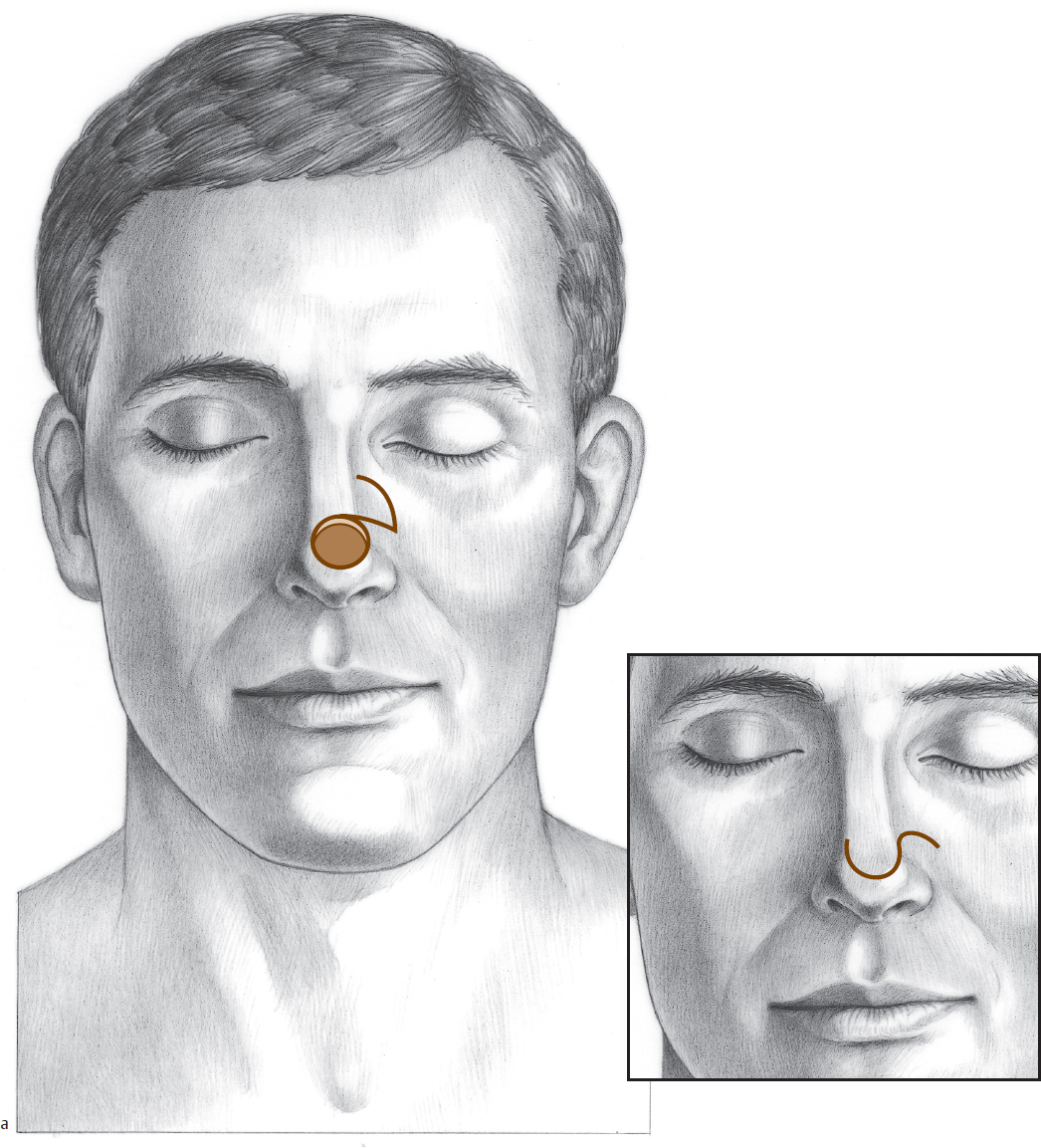
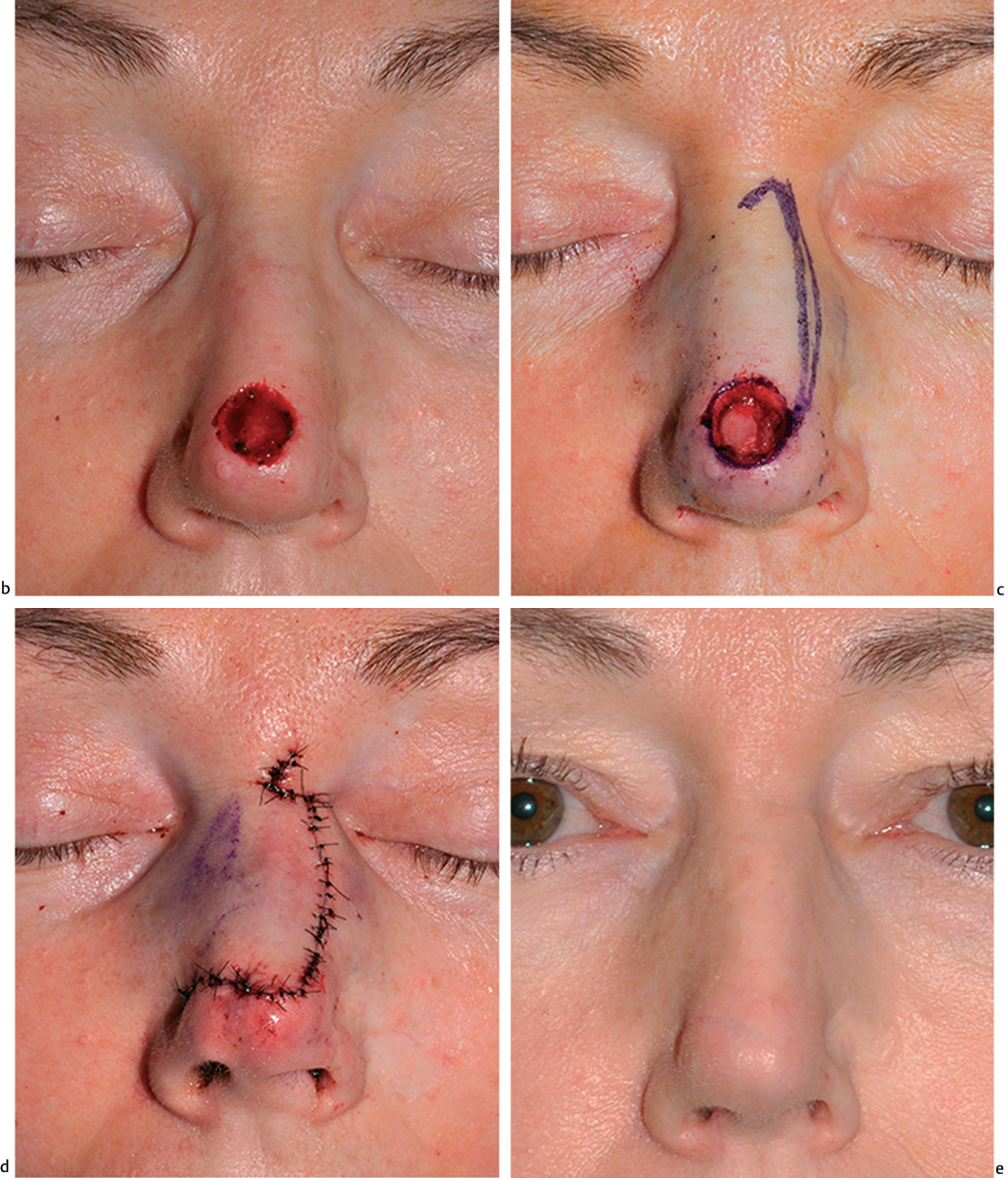
Fig. 6.7 (a) Single transposition flap to the nasal tip. (b) Nasal defect. (c) Defect with dorsal nasal sliding advancement flap template. (d) Flap closed. (e) Wound healed.
The modified bilobed flap is chosen for cases of nasal reconstruction because this design creates less of a standing cone formation than the standard bilobed design (Fig. 6.8, Fig. 6.9, and Fig. 6.10). The Zitelli-modified bilobed flap is designed with the total arc of rotation of 100 degrees or less, and each limb of the flap rotates 45 to 50 degrees. The flap can be either medially or laterally based. The first limb is designed the same size or just slightly smaller than the defect size, and the second limb is typically one-half to three quarters of the size of the primary limb. This flap design takes advantage of the less adherent skin and subcutaneous tissue of the dorsal and sidewall subunits for reconstruction of defects.
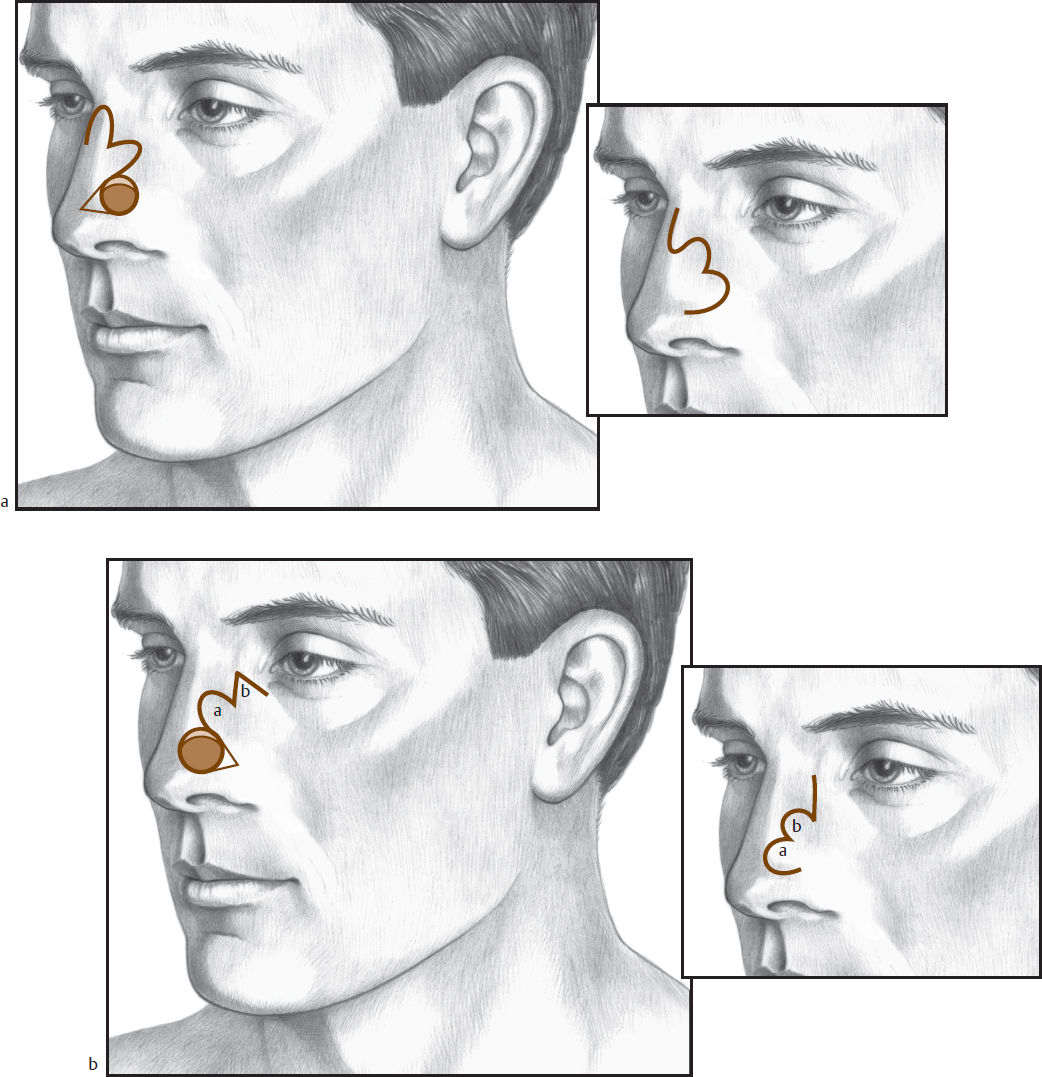
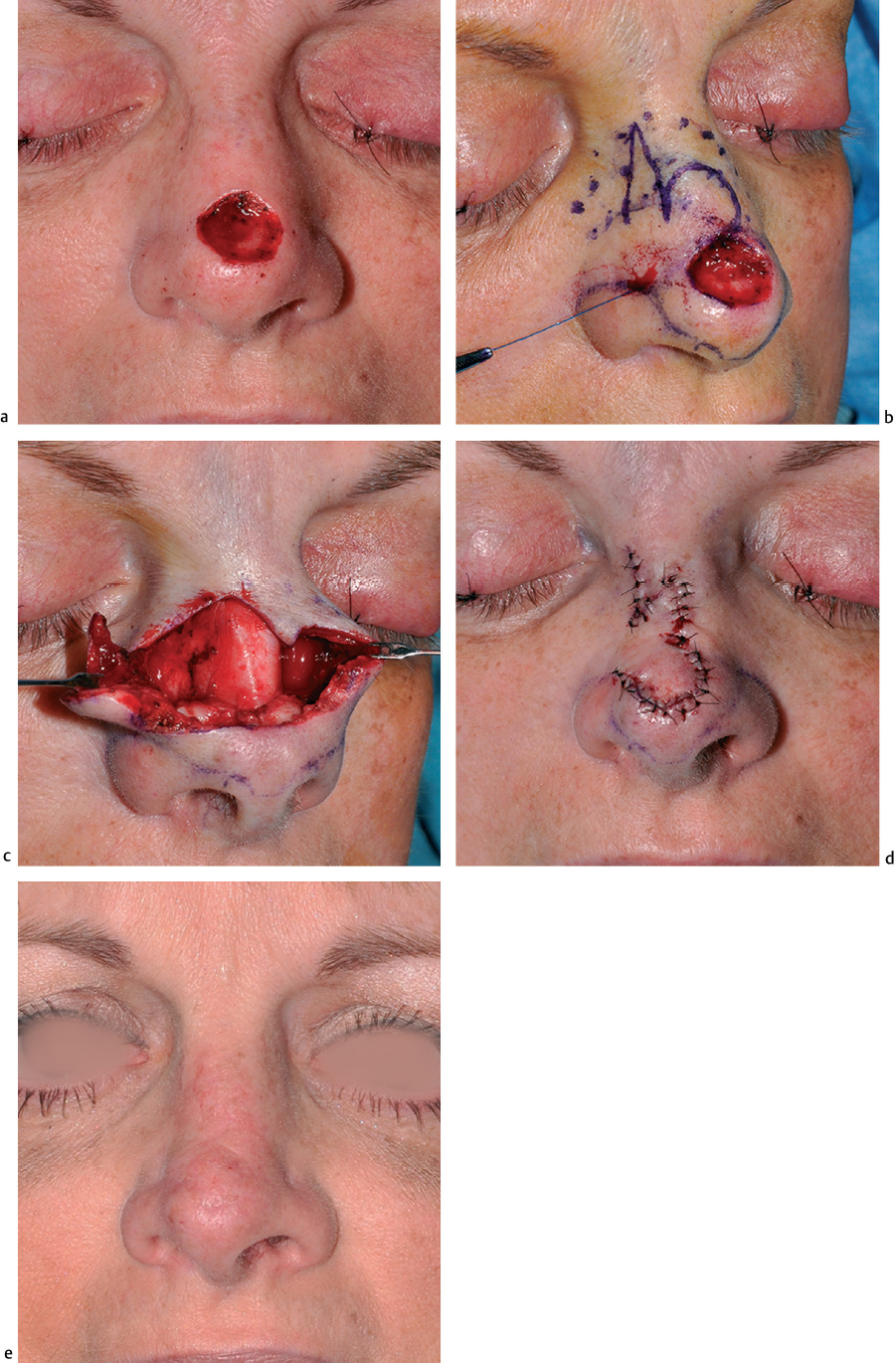
Fig. 6.9 (a) Nasal tip defect. (b) Superiorly based bilobed flap. (c) Flap elevated and widely undermined. (d) Flap closure. (e) Healed wound.
Large defects of the dorsum and combined defects of the dorsum and sidewall usually require a melolabial flap or a forehead flap for adequate closure. The nasal lining and structural framework of the nose also commonly demand reconstruction in these cases. Skin-only defects of the sidewall can be replaced with a melolabial flap with pexing sutures from the dermis of the flap to the underlying periosteum to re-create the nasofacial groove (Fig. 6.11 and Fig. 6.12).
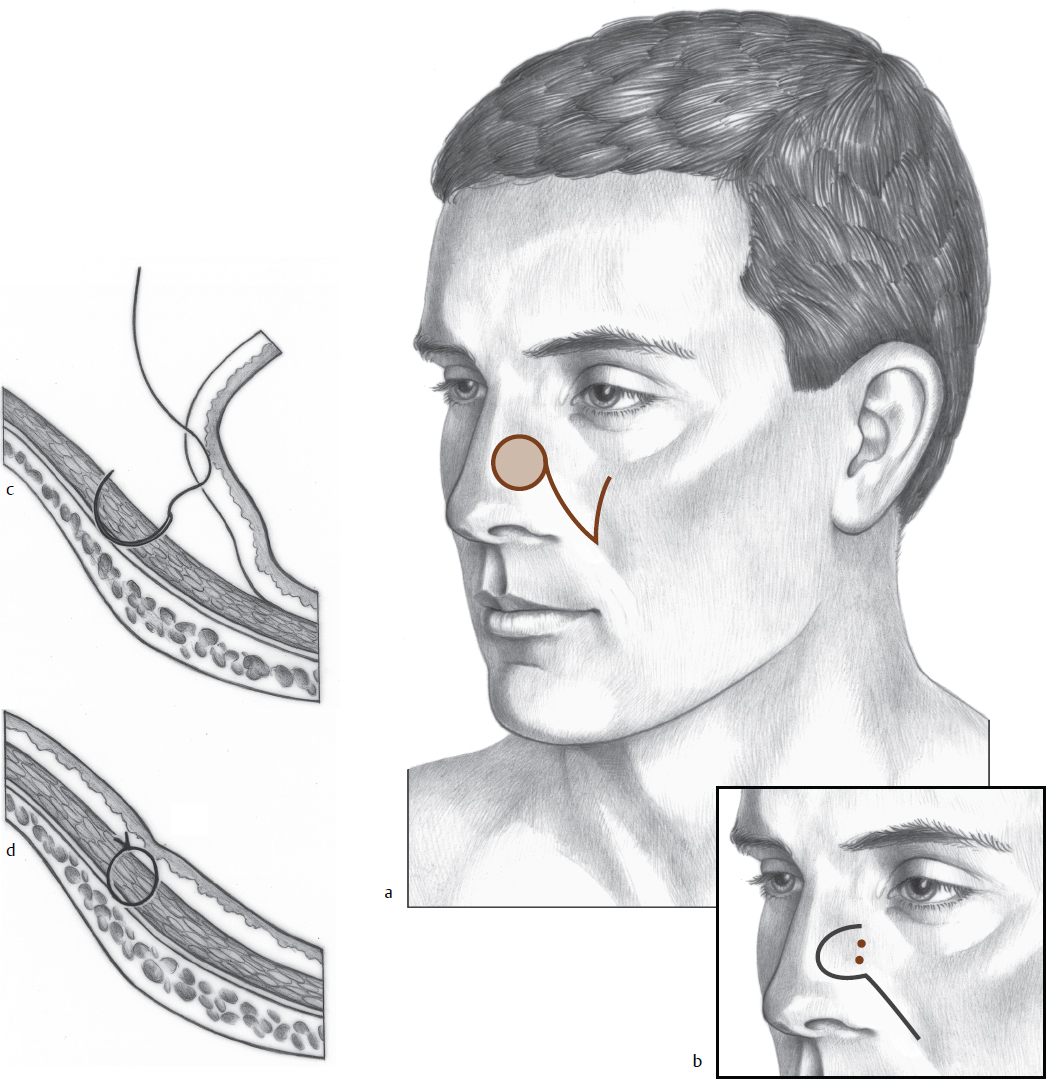

Fig. 6.12 (a) Right nasal defect and planned superiorly based transposition flap of cheek to nose. (b) Flap elevated. (c) Flap in place. (d) Late postoperative result.
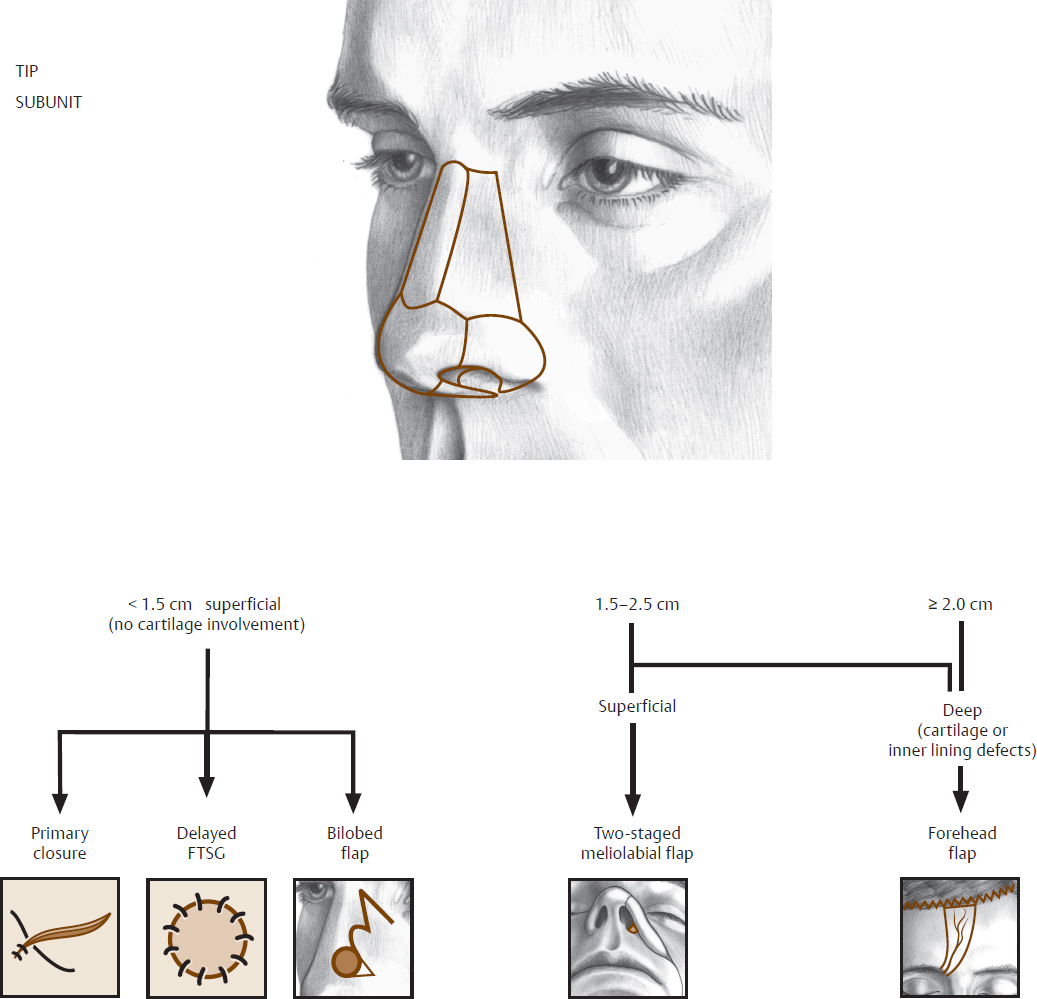
 Tip Subunit
Tip Subunit
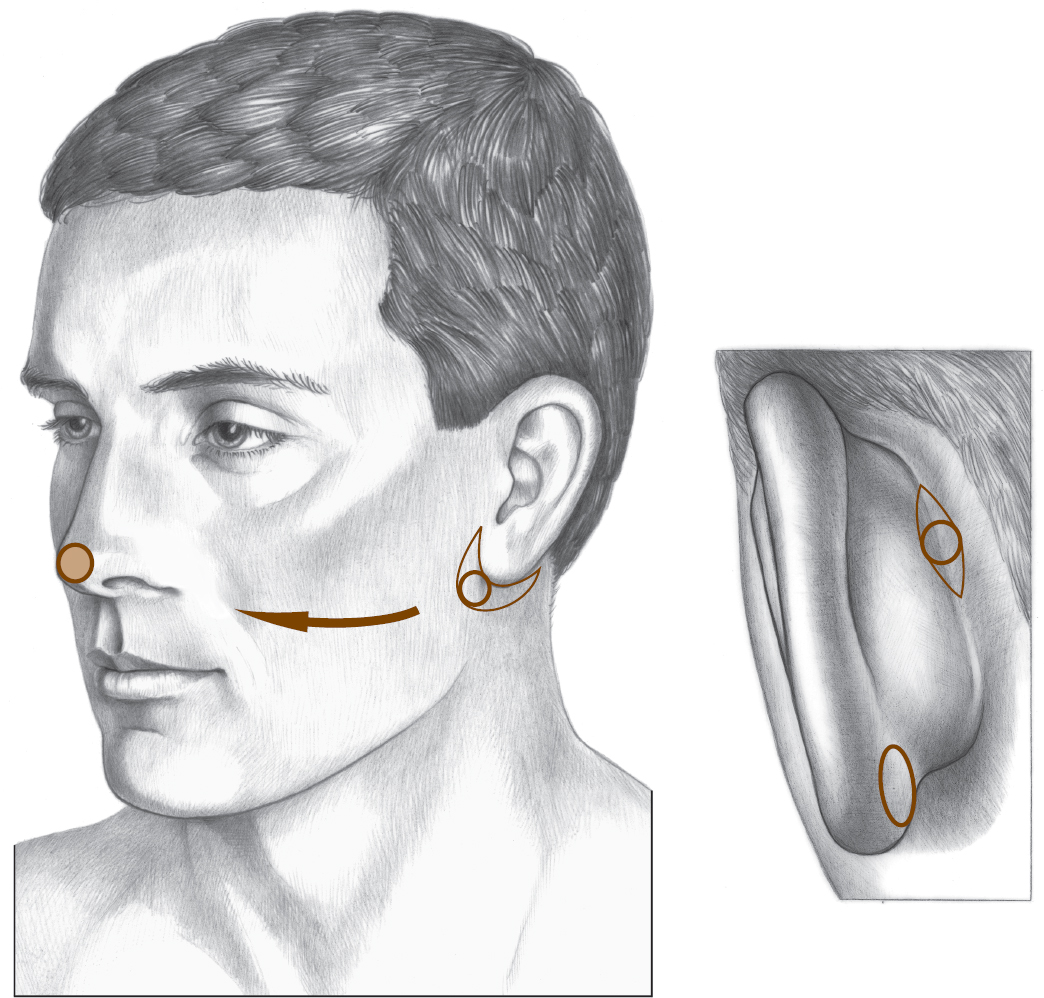
The skin in the tip is thicker, more sebaceous, and more tightly adherent to the underlying framework than the skin of the upper nose. Tissue can be transposed from the more mobile superior areas, but transposition flaps within the tip or alar subunits are not practical (Fig. 6.13). For small defects of the tip alone, an FTSG can be used with adequate results (Fig. 6.14 and Fig. 6.15). These results can be improved in deeper defects by allowing the bed of the wound to granulate for 2 to 3 weeks and thereby fill from below. Donor sites should be selected to match nasal skin thickness, color, and skin texture as closely as possible. Preauricular skin is a good choice, particularly in older individuals where the donor site can be closed in the preauricular crease. If the color match is good, the skin on the posterior aspect of the earlobe is elastic and has a texture similar to that of the tip.
Tip defects and those defects involving both the tip and adjacent supratip areas are best closed with a bilobed flap. The Zitelli modification is chosen because it transfers each lobe 45 to 50 degrees, rather than 90 degrees, thus minimizing standing cone formation. The flap can be either medially or laterally based, depending on the position of the defect.
Large defects involving the tip and ala, or the tip and part of the sidewall, can sometimes be repaired with a large melolabial flap, but they usually require a forehead flap (see Forehead Flap section). Superficial (skin-only) extensions of a defect from the tip onto the columella can be repaired with a large FTSG, but more extensive columellar defects require a staged, superiorly based melolabial flap or a composite graft (see the following section).