11 Nonsurgical Salvage and Enhancement of a Surgical Result Summary The principle of thermal disruption of collagen fibers is the basis for many nonsurgical aesthetic treatments, such as intense pulsed light (IPL), radiofrequency (RF), high-intensity focused ultrasound (HIFU), and skin care with peeling agents. All of these treatments cause skin tightening. Understanding wavelength, power, spot size, pulse width, and cooling help optimize outcomes and reduce unfavorable results. Keywords: ablative, downtime, CO2 laser, Er:YAG laser, facial rejuvenation high-intensity focused ultrasound (HIFU), intense pulsed light (IPL), microthermal zones (MTZs), nonablative, radiofrequency (RF), skin laxity, soft tissue deflation Key Points • Proper patient selection and realistic expectations are key for optimal nonsurgical results. • Thermal energy is responsible for skin tightening. • Patients should be treated at the lowest energy able to produce a response. • All nonsurgical devices carry risk for significant complications. Nonsurgical aesthetic medicine continues to be a growing field, with an increase of 22% in the number of nonsurgical procedures performed in 2015.1 Demand for minimally invasive options is increasing due to the increase in the popularity of nonsurgical procedures and the industry’s focus on direct-to-consumer marketing. The nature of these types of procedures allows for patients to continue to cycle through a practice and may ultimately lead to surgical conversion for some patients in the future. Techniques such as nonablative and ablative lasers, intense pulsed light (IPL), radiofrequency (RF), high-intensity focused ultrasound (HIFU), and skin care with peeling agents may also be used in conjunction with surgery to optimize the patient’s overall aesthetic results. Each of these technologies relies on a similar principle of thermal disruption of collagen fibers. Collagen is a polymer held together by hydrogen bonds, and it is these cross-links that attribute to the collagen strength. Thermal energy causes a denaturing of the collagen while the heat-stable intramolecular cross-links are preserved.2 Skin tightening occurs due to a physical shortening of the collagen fibers with preservation of the intramolecular hydrogen bonds, possibly increasing the elastic properties of the skin.3,4 With increased delivery of thermal energy (i.e., increased tissue temperature), there is a greater degree of collagen denaturation and thus resultant tissue tightening. Thermal injury also induces local fibroblasts to produce new collagen as a part of the wound-healing response. Balancing appropriate thermal injury without causing tissue necrosis remains the greatest challenge as the demand for improved efficacy and reproducible treatments rise. Changes within the collagen occur in a time- and temperature-dependent manner, meaning that both short exposures to high temperatures or prolonged exposure to lower temperatures will both create a degree of collagen shortening. Bozec and Odlyha5 demonstrated that denaturing of collagen fibrils occurs at approximately 65 °C, with initial collagen injury occurring around 58 °C. Additional studies agree that disruption and denaturing of collagen occurs in the 60 to 65 °C range, with a greater degree of denaturation occurring at higher temperatures.2,3,6,7 It is this initial collagen insult along with the resulting neocollagenesis that triggers the healing response responsible for the observed thermal tightening. However, the burn literature suggests that extensive cell membrane breakdown begins to occur at temperatures above 45 °C.8 As with any device, the user must understand the parameters of the device not only to optimize outcomes, but also to reduce possible treatment-related complications. Understanding and manipulation of five key parameters allow the user to master the laser device at hand instead of being at the mercy of preset manufacturer protocols.9 Five Parameters for Operating a Laser Device 1. Wavelength: determined by the target chromophore and its location within the tissue 2. Power: the amount of energy delivered to the tissue target 3. Spot size: used in correlation with the power to determine the power density 4. Pulse width: the delivery or exposure time of selected energy delivered to the tissue target 5. Cooling: allows for maximal depth of injury without harming more superficial tissue Only through a complete understanding of the interplay of these five parameters is the user able to adequately treat the target tissue with lasers without unnecessarily damaging the collateral tissue in the process10 ( Nonsurgical laser devices may be divided into two categories, nonablative and ablative, which share a similar goal of making skin-surface changes. When evaluating patients for laser or light therapy, the correct device needs to be chosen to address the specific skin disorder being treated, the target chromophore, and it must have acceptable downtime ( • Fractionated 10,600 nm CO2. • 2940 nm erbium:yttrium-aluminum-garnet (Er:YAG) laser. • Full-field Er:YAG. • 1064 nm neodymium-doped:yttrium-aluminum-garnet (Nd: YAG) laser. • 532 nm potassium titanyl phosphate (KTP) laser. • IPL device. When using laser and light therapy, there are three main target chromophores within tissue: hemoglobin, melanin, and water. Hemoglobin has three peaks at 400 nm, 532 nm, and 577 to 600 nm, with 577 nm being the most selective for this chromophore. Melanin is found in a wider spectrum—between 400 to 1100 nm of light—with the ranges of 400 to 475 nm and 630 to 810 nm being the most selective. Ablative lasers rely on water molecules stored within the tissue target ( Table 11.2 Choice of Devices Based on Treatment Issue and Associated Downtime
11.1 Introduction
![]() Table 11.1). With each subsequent treatment, the patient’s tissue is uniquely changed and will thus present differently for each subsequent treatment. This leads to a need for slight modifications to the treatment parameters with each procedure.
Table 11.1). With each subsequent treatment, the patient’s tissue is uniquely changed and will thus present differently for each subsequent treatment. This leads to a need for slight modifications to the treatment parameters with each procedure.

11.2 Laser and Intense Pulsed Light Therapies
![]() Table 11.2) The most commonly used nonablative, ablative, and light-based devices in our practice are the
Table 11.2) The most commonly used nonablative, ablative, and light-based devices in our practice are the
![]() Fig. 11.1).
Fig. 11.1).
Downtime | ||
| Hours | Weeks |
Pigment | IPL, KTP (532) | Erbium |
Redness | IPL, YAG (1064), KTP (532) |
|
Wrinkles | Botox, Fillers | TCA, Erbium, FCO2 |
Acne | Fillers | Excision, Erbium, FCO2 |
Laxity | Ultrasound, RF | Surgery |
In our hands for skin resurfacing, the full ablative 2940 nm Er:YAG laser has the most dramatic effect on skin resurfacing at the cost of increased downtime. The Er:YAG laser has largely replaced the previous generation of CO2 lasers because of the Er:YAG’s precise depth of ablation without the undesirable collateral tissue heating commonly seen with traditional CO2 devices. Total ablative Er:YAG resurfacing has a much more significant recovery than any of the nonablative lasers. However, the Er:YAG is able to provide very predictable results with visible end points. This is in part due to the Er:YAG’s high absorption by water, which is 13 times greater than that of the CO2 laser. Heating of this water with suprathreshold fluences leads to immediate cellular heating, resulting in instant tissue vaporization. A high absorption by water allows for a more precise suprathreshold ablation, with less subthreshold collateral damage to the surrounding tissue. The main downside to the Er:YAG is the prolonged recovery, usually requiring 7 to 10 days for complete re-epithelialization as compared to nonablative modalities. Patients typically have prolonged redness for at least 2 to 3 months posttreatment, and it may persist for up to 6 months. This may be shortened by use of IPL vascular treatments to reduce redness after a few weeks postresurfacing.
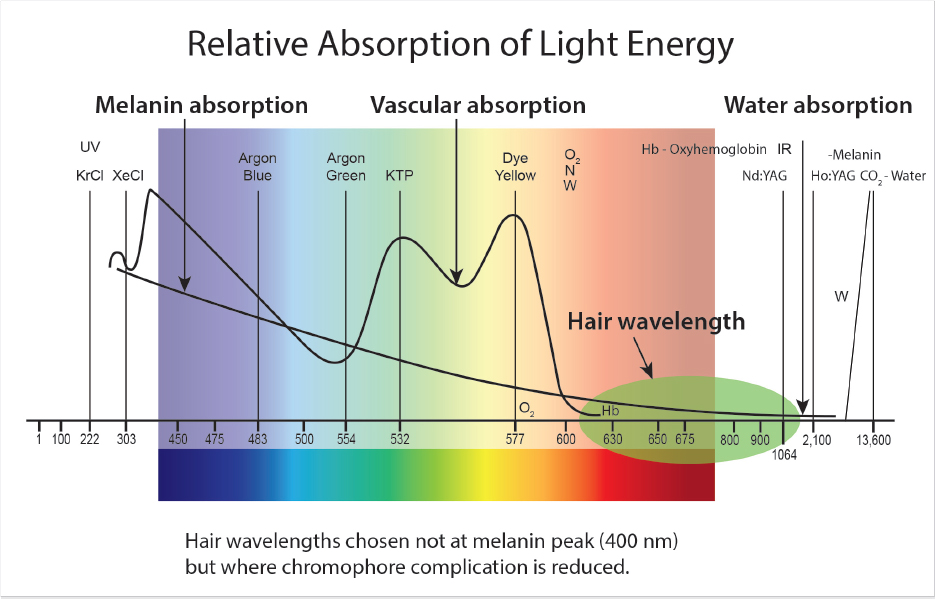
Fig. 11.1 The wavelengths chosen for hair reduction are not at the melanin absorption peak (400 nm) but at longer wavelengths to minimize complications.
Fractionated lasers were developed with the hope of achieving an end result similar to that of the fully ablative CO2 and Er: YAG lasers while allowing the patient a quicker recovery with less downtime. Fractionated devices use extremely high fluences to deliver focused columns of energy into the tissue, resulting in microthermal zones (MTZs) of injury. Areas surrounding these MTZs only reach sublative temperatures, yet they still undergo significant protein denaturation, tissue coagulation, and apoptosis.11 The thermal injury sustained generally extends 200–300 μm, although it can go deeper, into the dermis, leading to the previously mentioned cascade of heat-induced collagen shortening and neocollagenesis. By delivering a discontinuous, segmental injury to the tissue, reservoirs of healthy tissue remain to speed healing and to act as a source of keratinocyte migration.12 Theoretically, these MTZs should produce sufficient injury to create a tissue response similar to that of the fully ablative CO2 and Er:YAG lasers, yet this has not been the results experienced in our clinic.13,14
Doubling the frequency of a 1064 nm laser by way of a KTP crystal is what makes the higher-energy 532 nm KTP laser possible. One specific advantage of 532 nm over 1064 nm are that treatment energies for 532 nm are one order of magnitude less for the same chromophore (arteries or oxygenated hemoglobin), meaning that when treating superficial telangiectasias located in the superficial dermis, less energy is needed to see a response. Whenever treating patients, the goal is to use the minimum effective dose of energy at which a desired clinical end point is still evident, which prevents the delivery of excess energy into target tissue and lessens the risk of subsequent adverse events.14,15,16 A downside of the 532 nm laser is that it only has a very superficial absorption length and is typically much less effective for vessels larger than 500 μm.17 Additionally, the use of the 532 nm laser in darker skin types must be approached very cautiously, because melanin competes with hemoglobin at this wavelength.
The 1064 nm, on the other hand, is able to adequately treat deeper tissue and larger vessels, to a depth of 5 to 6 mm and a diameter up to 2 to 3 mm. However, this comes at the cost of increased fluences caused by a decrease in the absorption coefficient, resulting in more discomfort for the patient.
Although surgery remains the gold standard for facial rejuvenation, surgery alone is only able to address skin laxity and soft tissue deflation. Global facial rejuvenation must address the skin surface as well. Years of sun exposure may result in static and dynamic rhytides, poor skin texture, and multiple dyschromias. Although initially there was some hesitancy to perform laser skin resurfacing at the same time as or as an adjunct to surgery, it has since been shown to be safe in select patients using moderate settings.18,19,20 Despite its safety, many practitioners still prefer to wait 3 to 6 months after surgery before performing full-face laser skin resurfacing.
11.2.1 Intense Pulsed Light
IPL is our most commonly performed office procedure and has high patient satisfaction. Although commonly referred to as a laser, IPL is a flash lamp device, not a laser. This technology works by generating a polychromatic light and most commonly has an output spectrum between 400 nm to 1400 nm within the electromagnetic spectrum. What differentiates IPL from a laser is that a laser most often emits a single wavelength, whereas IPL delivers an entire spectrum of light at the same time. IPL works by passing light through specific filters to block unwanted wavelengths, thus tailoring the emitted wavelengths for a desired chromophore. Although the perception remains that because this is not a laser it is inherently a safer device, the opposite is true, because it emits up to 1,000 different wavelengths and the precise treatment of every chromophore is sometimes difficult to control. Simply put, this is a device that scans for every chromophore due to the spectrum of light emitted, and wavelength-limiting filters are used in an effort to regain some control. These filters are commonly high-pass filters that block wavelengths below the number indicated on the filter while allowing longer wavelengths to pass through to tissue. Shorter wavelengths are absorbed in the more superficial targets, and this allows targeting the deeper dermis without damaging upper skin structures. IPL therapy may be used for the correction of photoaging and the treatment of pigment of vascular lesions, erythema, or acne.
11.3 Patient Selection for Laser And Light-Based Devices
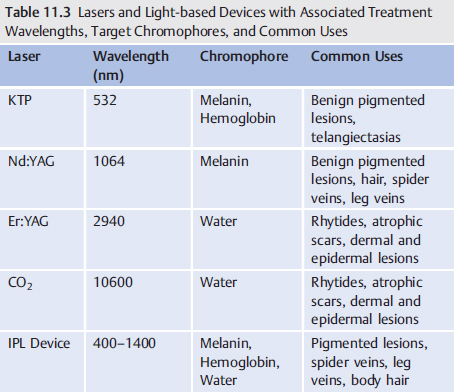
532 nm KTP lasers are best suited for the treatment of small veins, pigment, tattoos, port-wine stains, and for nonablative dermal remodeling.21 Similar to the KTP laser, the 1064nm Nd:YAG is commonly used for nonablative facial resurfacing, hair removal, treatment of acne, leg veins, pigmented lesions, and vascular anomalies.22,23,24,25,26,27,28,29,30 Patients needing aggressive skin resurfacing for select pigments, skin texture, or rhytides are best treated with Er:YAG.31,32,33,34,35 IPL is the most versatile of the devices due to the broad range of wavelengths it produces. It may be used for the treatment of telangiectasias, dyschromias, and hair reduction24,36,37,38,39 (![]() Table 11.3).
Table 11.3).
An excellent way to enhance facial rejuvenation is through the placement of adipose or hyaluronic acid fillers with the addition of concomitant facial resurfacing (see Video 1.1).40 Facial fat grafting can restore lost facial volume, whereas laser resurfacing addresses superficial and deep rhytides, improving facial contours and skin texture. We have performed upper lid surgery, facial fat grafting, and simultaneous laser resurfacing with excellent results. Laser resurfacing has also been shown to be safe and effective when performed at the same time as lower lid blepharoplasties.41
11.4 Technical Steps and Treatment Plan
Many patients undergoing more aggressive in-office procedures may require pretreatment with an anxiolytic agent in addition to an oral narcotic. We commonly use 0.25 to 0.50 mg alprazolam (Xanax, Pfizer Inc.) and oral hydrocodone containing medications such as Norco (Allergan, Inc.) or Lortab (Akorn, Inc.; UCB, Inc.). Pretreatment continues with the application of a topical compound containing benzocaine, lidocaine, and tetracaine (BLT) to all treatment areas. Although topical anesthesia is seemingly innocuous, care must be taken when treating large areas due to the potential risk for lidocaine toxicity.42,43 Regional nerve blocks are sometimes required depending on the pain associated with the procedure and the pain threshold of the patient. Nerve blocks are typically placed using 0.25 to 1% Xylocaine (lidocaine HCl) plain mixed with bicarbonate. Intraocular shields are often placed for corneal protection when the periorbita is being treated. Procedures such as aggressive fractionated CO2 and erbium are challenging to manage in the office, so these patients are most comfortable under heavy sedation/anesthesia in a monitored setting.
11.4.1 1064 nm (Nd:YAG) Laser for Vascular Lesions
1. ![]() Table 11.1 Use the least amount of energy to effectively close vascular targets.
Table 11.1 Use the least amount of energy to effectively close vascular targets.
2. Use contact dynamic (PPP) cooling at 10 to 20 °C for safety.
3. Start at 80 J/cm2 and titrate energies in increments of 10 J/cm2 until a desired response is achieved (stasis).
4. Using a 6-mm spot, regardless of vessel diameter, will ensure that the vessel falls within the effective treatment zone. For 200 um and less and when treating over bone or competing targets such as beard hair in the area, use a 3-mm spot and double-treatment energy range starting at 160 J/cm2.
5. Keep handpiece 90° to tissue plane.
6. Position patient in supine position to equalize pressures.
7. Use sapphire cooling in light contact. The use of optical coupling gel helps step index the light into the skin and draws heat out postdelivery.
8. You should find that a range of 80 to 120 J/cm2 for 6 mm spot and 160 to 240 J/cm2 for 3 mm spot will be sufficient to effectively close most vessels regardless of color and or location.
9. Change only one parameter at a time.
10. Once the fluence (J/cm2) has been established, pulse width is your key
parameter on remaining vessels.
11. Goal:
• Raise blood above 70 °C.
• Damage intima.
• Contract Type I & Type III collagen surrounding vessel.
• Achieve vessel stasis (no purge and refill).
*Treatment range for 6 mm spot: 80 to 120 J/cm2
*Treatment range for 3 mm spot: 160 to 240 J/cm2
11.4.2 Fractionated CO2
Most fractionated devices have several variables one can control including spot size, density, and fluence. Unfortunately, there are no visible endpoints to determine adequacy of treatment. It should be noted that higher-density treatments should be used with caution in darker skin types.
1. Apply a topical anesthetic of choice.
2. Consider regional and local blocks with lidocaine as desired.
3. If a stamp pattern is used, one should plan for a minimum of two passes to eliminate any gaps or overlap in treatment. For example, if a 20% density is desired, two passes at 10% are recommended.
4. A rolling pattern accounts for density and the number of passes are dictated by the software.
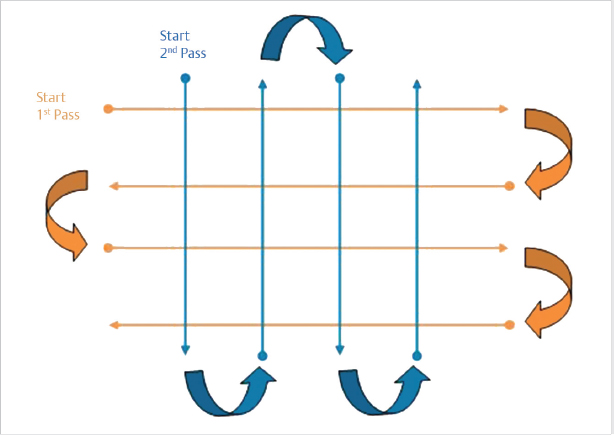
5. A crosshatch pattern should be applied for multiple passes to avoid gaps and stacking of treatments (![]() Fig. 11.2)
Fig. 11.2)
6. Following treatment, a light moisturizer is applied and used two to three times a day until peeling is complete.
11.4.3 Er:YAG Technical Steps (Micropeel)
1. Apply topical anesthetic 1 hour before procedure. Additional topical may be reapplied but there is a risk for lidocaine toxicity with additional applications.
2. Using wet 4X4’s, thoroughly remove topical and pat dry.
3. Set ablation to desired depth, typically 15 to 50 um (no coagulation).
4. 15 um initial peel accomplishes several goals:
• Allows assessment of individual erythema response. If patient has strong response, the treatment can be adjusted to match the promised recovery time.
• Removal of stratum corneum decreases topical uptake time while increasing the depth of topical penetration.
• A second application of topical helps eliminate the need for oral medication in ablations < 100 um.
• Doing two to three passes will give a more even coverage and ablation.