7 Microneedling and Platelet-Rich Plasma Summary Platelet-rich plasma (PRP) contains concentrated platelet-derived growth factor (PDGF), transforming growth factor-beta (TGF-β), vascular endothelial growth factor (VEGF), epidermal growth factor (EGF), and insulin-like growth factor (IGF), all of which promote local tissue repair. PRP is created by centrifuging autologous whole blood collected from a peripheral vein. PRP is applied as a topical or injectable adjunct to microneedling for synergistic augmentation of collagen production, angiogenesis, and tissue regeneration. PRP by itself has shown beneficial effects in the literature across various fields including orthopedic, cardiac, plastic, and oral and maxillofacial surgery. The process of microneedling creates microchannels into the dermis while stimulating collagen production and remodeling through the PDGF release. Microneedling is a successful treatment modality for several skin conditions including postacne atrophic scars, androgenic alopecia, and alopecia areata. Keywords: platelet-rich plasma (PRP), microneedling, platelet-derived growth factor (PDGF), transforming growth factor-beta (TGF-β), vascular endothelial growth factor (VEGF), epidermal growth factor (EGF), insulin-like growth factor (IGF), percutaneous collagen induction (PCI), collagen induction therapy, fibroblast growth factor (FGF), microchannels, alopecia Key Points • Platelet-rich plasma (PRP) is concentrated by centrifuging autologous whole blood collected from a peripheral vein. • PRP contains highly concentrated platelet-derived growth factor (PDGF), transforming growth factor-beta (TGF-β), vascular endothelial growth factor (VEGF), epidermal growth factor (EGF), and insulin-like growth factor (IGF), all of which promote local tissue repair. • Microneedling creates microchannels into the dermis while stimulating collagen production and remodeling through PDGF release. • PRP is applied as a topical or injectable adjunct to microneedling for synergistic augmentation of collagen production, angiogenesis, and tissue regeneration beyond either modality alone. Microneedling, also known as percutaneous collagen induction (PCI) or collagen induction therapy, was first described in the 1990s as a novel method of skin resurfacing.1,2,3 Microneedling utilizes direct mechanical trauma to modify tissues and requires very little downtime and a shorter healing phase when compared to ablative modalities such as laser or dermabrasion. Microneedle devices create controlled microchannels within the skin that close within minutes. Skin penetration stimulates platelets to release chemotactic factors causing invasion of other platelets, neutrophils, and fibroblasts. These cells release numerous growth factors including PDGF, fibroblast growth factor (FGF), TGF-α and TGF-β, all of which stimulate the migration and proliferation of fibroblasts, promote collagen production, and promote regeneration of a normal collagen lattice structure.4,5 Microneedling has also been reported as a successful treatment modality for several skin conditions including postacne atrophic scars, androgenic alopecia, and alopecia areata.6,7,8 More recently, microneedling technology has been augmented with additional modalities. One promising adjunct takes advantage of the temporary microchannels to directly introduce growth factors and cytokines in the form of PRP into the dermis. PRP is defined as the portion of the plasma fraction of autologous blood with higher-than-baseline platelet concentrations. This is achieved by centrifugation of whole blood drawn from a peripheral vein. High-speed centrifugation concentrates platelet levels fivefold to eightfold per volume of plasma.9 The most common and important growth factors found in PRP include • PDGF • TGF-β • VEGF • EGF • IGF These factors are chemotactic and mitogenic, promoting angiogenesis and subsequence migration of macrophages. Macrophages supplement the healing environment with additional growth factors and cytokines producing local tissue repair and continuous regeneration. Other affected cells include fibroblasts, stem cells, endothelial cells, osteoblasts, smooth muscle cells, and keratinocytes, which contribute to collagen production and angiogenesis.10,11 Given these effects, the addition of PRP to a treatment modality is sometimes advertised with the descriptive term vampire in reference to the creature of ancient folklore who sustains its immortality by drinking the blood of the living. PRP by itself has shown beneficial effects in the literature across various fields including orthopedic, cardiac, plastic, and oral and maxillofacial surgery.12 Multiple in vitro studies of PRP since 2007 have demonstrated increase in endothelial cell, stem cell, procollagen, fibroblasts, growth factor, and Type 1 collagen proliferation. Animal studies of PRP have also shown clinical benefit including increased wound healing, enhanced neurotrophic effects, increased fat grafting survival in rabbits and rats, reduction in wrinkling with increased fibroblasts, and increased bone formation in skull defects. Conversely, some studies have shown equivocal or deleterious effects of PRP including increased inflammation, diminished bony repair, and no effect on free fat graft survival in mice. In human trials, studies have been more consistently positive, with decreased edema and ecchymosis after facelifts, increased wound-healing rates, more rapid epithelialization of skin graft donor sites, decreased erythema after laser treatments, increased skin elasticity and collagen promotion, increased hair count in alopecia, improved diabetic wounds, and improved appearance of acne scars.13,14,15,16,17 In a review by Sommeling et al,18 36 out of 40 studies consisted of randomized controlled trials and case-control studies that demonstrated favorable outcomes with PRP use in plastic surgery. Because both microneedling and PRP are relatively new technologies in aesthetic medicine, the currently available literature evaluating the efficacy of the combined modalities is sparse but consistently positive. Akcal et al19 reported increased skin flap survival (p < 0.01) when PRP was combined with microneedling of ischemic skin flaps in a rat model. The increase in flap survival when compared to the control and microneedling-only groups suggests a benefit from PRP growth factors beyond microneedling alone.19 Similarly, in a split-face comparative study of microneedling with PRP versus microneedling with Vitamin C, Chawla20 found the PRP group to have significantly higher patient satisfaction after rolling and boxcar acne scar treatment, although Vitamin C provided more benefit for post-inflammatory hyperpigmentation. Given the known and similar benefits of microneedling and PRP, it is reasonable to expect that the combination of these two regenerative modalities can provide a synergistic effect on the regeneration and rejuvenation of skin (see Video 1.1). The patient selection criteria for microneedling with PRP are similar to those of microneedling alone. Beyond skin rejuvenation, patients who can benefit from microneedling with PRP include patients with surgical or postacne scarring, aging or sun-damaged skin, and hair disorders. Extra caution should be taken in patients with excess superficial vascularity, active skin inflammation or disease, sensitive or eczematous skin, diminished healing, or anticoagulant history, because recovery may be extended or complicated. Prior to treatment, patients should avoid prolonged sun exposure or sunburns for at least 24 hours to avoid excessive inflammation and injury. Topical products are discontinued 12 hours prior to treatment, and the skin must be clean and free from cosmetic products. Any patient with active or resolving infection should have treatment delayed until resolution. 1. All makeup and jewelry is removed, and standardized patient photos are taken. 2. The skin is degreased with alcohol prep, and a topical anesthetic cream composed of 20% benzocaine, 6% lidocaine, and 4% tetracaine is applied to the planned treatment areas. This cream is allowed to penetrate the skin for 30 to 45 minutes. 1. Using sterile technique, 10 mL of autologous whole blood is drawn from a peripheral vein into tubes containing the anticoagulant, acid citrate dextrose (ACD). 2. Tubes are gently and manually inverted and turned 5 to 10 times prior to placement into a centrifuge. 3. Tubes are centrifuged 3,500 rpm for 15 minutes at a room temperature of 22 °C to obtain a platelet count at least 4.5 times higher than baseline. a) Using an 18-gauge needle, serum is extracted and placed into separate 3-mL syringe vials for use. 4. The supernatant platelet-poor plasma (PPP) can be partly removed and partly used to resuspend the platelets or, preferably, the entire serum volume can be used to resuspend and minimize the loss of platelets. 5. Although calcium gluconate can be added as an activator 1:0 (i.e., 1 mL of calcium gluconate in 9 mL of PRP), platelets will become activated upon contact with dermis or blood during microneedling.10 Early activation of PRP with calcium may create clumping or gelling and could prevent penetration into the dermal microchannels. 1. After 45 minutes or when the patient is sufficiently numb, the face is wiped clean and cleansed with a gentle cleanser and sterilized with alcohol. Sterile saline is used to wipe the skin, and the skin is pat dry. 2. The face is divided into sections (cheeks, perioral, periocular, and forehead). 3. The forehead and upper lip are the most sensitive areas and are therefore treated first while they are still numb. PRP is applied to the skin with the needleless syringe and spread evenly in the section to be treated. Appropriate needle depth selection should allow sufficient penetration of the PRP. Alternatively, intradermal injection of PRP can be performed. 4. Needle depth is chosen according to the section to be treated: a) Forehead: 1.0 to 1.25 mm. b) Periocular: 1.0 to 1.25 mm. c) Perioral: 1.5–2.0 + mm × 3 to 5 passes in each direction AND 0.5–1.0 mm × 2 passes in each direction. 5. Cheeks: 1.5–2.0 mm + × 3 to 5 passes in each direction AND 0.5–1.0 mm × 2 passes in each direction. 6. Three horizontal passes and 3 vertical passes (more if tolerated) are made per section, while additional PRP is added throughout the process to keep the skin from drying and to allow penetration into the skin. Needle depth is decreased if purpura is observed. Extra, superficial passes on the cheeks and mouth are used to maximize textural change by targeting different depths. 7. Once the microneedling is complete and all of the serum is used, the skin is gently wiped with a wet, nonwoven gauze pad and a biocellulose mask composed of aloe vera, Argireline (acetyl hexapeptide-3, Lipotec SA), glycerin, and hyaluronic acid is applied and left on for 15 minutes. The mask decreases erythema and recovery time, and it provides a cooling effect. An ice roller can be used alternatively or concurrently on the mask for added patient comfort. 8. After removing the mask, hyaluronic acid serum can be applied if desired, and a thin layer of occlusive moisturizer can be placed for skin protection. (
7.1 Introduction
7.2 Patient Selection
7.3 Technical Steps and Treatment Plan
7.3.1 Patient Preparation
7.3.2 Platelet-Rich Plasma Preparation
7.3.3 Treatment
7.4 Results
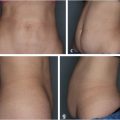
7.4.1 Case 1
![]() Fig. 7.1)
Fig. 7.1)
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine