14 Minimally Invasive Techniques: Preventing and Managing Adverse Events Summary Preventing adverse events in minimally invasive blended aesthetic treatments begins with appropriate patient selection. It is critical to understand patient anatomy, the risks and benefits of the procedure, and to understand and master the techniques associated with optimal patient outcome. Managing adverse events requires recognizing them when they occur and understanding how to treat them. Complications include the inherent risk of bleeding, damage to important tissues and structures, wound closure difficulties, poor healing, and infection. Keywords: complications, deoxycholic acid, dermal filler, infection, intense pulsed light (IPL), laser resurfacing, micro-focused ultrasound, neurotoxin injection Key Points • Always take a comprehensive medical and cosmetic procedure history and speak to the patient about other potential lifestyle factors that may impact the aesthetic outcome. • Many complications can be avoided by making sure to only select appropriate patients. • When performing any procedure, it is critical to understand patient anatomy, the risks and benefits of the procedure, and to understand and master the techniques associated with optimal patient outcome. • Adverse events can occur with any procedure and at the hands of any clinician. It is critical, therefore, to prevent them whenever possible, recognize them when they occur, and understand how to treat them. • Informing the patient of every potential risk and complication inherent to a product or procedure is the moral and ethical duty of the provider. Blended aesthetic medicine is a sophisticated and personalized cosmetic approach that, by definition, uses a combination of procedures incorporating neurotoxin injections, injectable fillers, and devices, including both ablative and nonablative lasers, radiofrequency and microfocused ultrasound, chemical peels, absorbable lifting sutures, and/or surgery. The ideal blending of procedures combines the benefits of multiple modalities and result in a cumulative effect that no one method can accomplish alone. However, with the increased potential afforded in blended aesthetic medicine also comes the increased complexity of safety considerations and the increased risk of complications.1,2 A variety of complications can arise from aesthetic medical procedures. Well-known surgical complications include the inherent risk of bleeding, damage to important tissues and structures, wound closure difficulties, poor healing, and infection. Less frequently, secondary events due to an adverse reaction to anesthetics or sedatives can even be life-threatening. Although less invasive, even the modern nonsurgical cosmetic techniques that many patients actively seek and prefer are also certainly not without the risk of very minor or even rarely severe complications.2 If and when complications and adverse events occur while employing blended aesthetic medicine, a physician with a deeper understanding of each product, each technique, and the contributing factors involved will be more able to effectively prevent, perceive, and manage complications.3 In this chapter, we will discuss a variety of minimally invasive procedures that are commonly used in blended aesthetic medicine, such as neurotoxin injection, dermal filler, laser resurfacing, deoxycholic acid, and microfocused ultrasound. First, appropriate patient selection and common indications and contraindications will be listed, followed by the potential complications of each method and how one can effectively prevent, treat, and manage such adverse events. The selection of suitable patients and the exclusion of inappropriate patients is the first and perhaps the most important step in avoiding complications. For any cosmetic procedure, a thorough and comprehensive medical and cosmetic history must be elicited in order to avoid treating patients with preexisting conditions that are contraindicated to treatment. Obviously, it is also critically important to discuss realistic expectations of the aesthetic outcome, as well as the number of treatments required to reach personalized goals. Patients will undoubtedly be unsatisfied with the results if they are not sufficiently informed of the limitations of these minimally invasive techniques. Dermal fillers of all types are frequently used to replace lost volume, decrease the appearance of wrinkles, and improve the overall contour of the skin on the face. In addition, off-label use for the correction of facial depressions caused by prior surgery, as well as administration to other areas of the body to help treat volume loss, is also common.4 When considering any dermal filler injection, patients with evidence of active skin infection in the proposed treatment area should force a delay of the treatment, because the infecting organism can spread to deeper tissues with trauma induced through the needle. Examples of such cases include viral infections such as herpes simplex virus (HSV) and human papilloma virus (HPV), molluscum contagiosum, bacterial infections such as streptococci or staphylococci, and rarely fungal and yeast infections5 ( Fig. 14.1 (a) Lesions of the treated areas often indicate infection. Punched-out circular lesions are typical of herpetic infection. (b) Posttreatment appearance of common fungal infection.5 (Reproduced with permission from Bass L and Pozner J: Laser Facial Resurfacing. In Cohen M and Thaller S: The Unfavorable Result in Plastic Surgery: Avoidance and Treatment, Thieme Medical Publishers, St. Louis, 2017) Likewise, dermal fillers can exacerbate chronic preexisting skin conditions such as autoimmune and connective tissue diseases. Poor candidates for dermal fillers may include patients with history of hypertrophic and keloid scarring, discoid lupus erythematosus, active scleroderma or psoriasis, Marfan syndrome, and Ehlers-Danlos syndrome. In patients with systemic disease such as human immunodeficiency virus (HIV), diabetes mellitus, or scleroderma, treatment can cautiously be performed if the patient has displayed a history of normal wound healing. Therefore, immunosuppressed patients should be screened carefully to determine if they are good candidates for treatment.6,7 • Lipoatrophy • Rhytides and folds • Depressed facial defects • Cosmesis • History of multiple or severe allergies or anaphylaxis • Active skin infection in the treatment area • Isotretinoin for 6 months before or after treatment (controversial) • Autoimmune and connective tissue diseases • Pregnant or lactating women • Certain psychiatric conditions such as body dysmorphia Patients with dynamic rhytides and no static component will show the most impressive improvement from injection with botulinum toxin. Patients who have rhytides visible at rest will also benefit from this type of treatment, although peak improvement is likely to require numerous administrations. These deeper wrinkles may become softened over time, but combination treatment with dermal fillers or resurfacing procedures may be required to achieve the desired results. The most notable contraindications to botulinum toxin injection include patients with neuromuscular disorders such as myasthenia gravis, amyotrophic lateral sclerosis, Labert-Eaton myasthenic syndrome, and other myopathies that involve neuromuscular transmission. Relative contraindications include patients with impaired healing, bleeding abnormalities, a history of hypertrophic or keloidal scarring, and those with significant skin atrophy. A very unique contraindication to neurotoxin administration is the need for uncompromised facial expression. This can be found frequently in patients with occupations in the show business. As with any procedure, the clinician and the patient should discuss end treatment goals and realistic expectations.8,9 • Rhytides • Hyperhidrosis • Blepharospasm • Strabismus • Migraines • Platysma neck muscle bands • Dystonias (cervical, cranial, facial, oromandibular, laryngeal) • History of allergy or sensitivity • Pregnant or nursing women • Active infection or dermatoses in the treatment area • Bleeding abnormalities • Impaired healing • Hypertrophic or keloidal scarring • Skin atrophy • Body dysmorphic disorder • Dependence on uncompromised facial expression • Myasthenia gravis • Amyotrophic lateral sclerosis • Eaton-Lambert syndrome • Other neuromuscular disorders Recently, the FDA has approved deoxycholate treatment designed to reduce submental fat (SMF). Traditionally, SMF reduction can effectively be treated by liposuction and lower facelift and neck lift, with or without submentoplasty. However, patients continue to seek less invasive methods. A recent set of studies investigating injectable deoxycholic acid has met with very encouraging results (see Video 2.11).10,11 Deoxycholic acid is thought to act by disrupting the membranes of adipocytes through solubilization of the membrane lipids, causing the targeted destruction of fat cells.12 Future studies will hopefully look to explore a deeper understanding of this attractive modality (see Video 1.1). • Moderate or severe convexity associated with SMF • History of dysphagia • Facial neurapraxia • Loose skin or previous trauma in the submental area • Prominent platysma bands • Any localized swelling in the submental area • Infection in submental area Ablative laser resurfacing utilizing CO2 or erbium lasers can either be fractional or nonfractional. Proper patient selection is particularly important when considering any laser resurfacing. Most notably, it is critical to appreciate the patient’s Fitzpatrick skin type, because there exists significant risk for dyspigmentation with this methodology. For example, patients with higher Fitzpatrick skin types (darker skin types) are at increased risk for postinflammatory hyperpigmentation (PIH), which can prove extremely difficult to remedy. In addition, patients with a history of poor wound healing, hypertrophic scarring, or keloids are not candidates for aggressive treatment, and thus lower fluences should be utilized on these patients. As always, a detailed history should be obtained during cosmetic consultation to accurately predict the risk of known side effects.13 Among others, common indications for both fractional ablative and nonablative laser treatment include mild to moderate facial and periorbital wrinkles, acne scarring, dyschromias, and postburn and surgical scars. More dramatic improvement has been shown with fine rhytides as opposed to deeper creases, and again realistic expectations should be conveyed to these patients.14 • Perioral vertical furrows • Periorbital dynamic lines (crow’s-feet) • Mild dermatochalasis • Glabellar dynamic lines • Actinic damage • Facial elastosis • Scars, including acne scars • Epidermal lesions • Dyschromias • Mild photodamaged skin • Superficial and deep rhytides • Mild rhytides, photodamage • Acne scar • Postsurgical scar • Skin texture improvement • Reduced adnexal structures • Unrealistic patient expectations • History of keloid scars • Active acne • Deep acne pits • Isotretinoin treatment in the last 6 months • Recent radiation therapy Microfocused ultrasound is a recently developed technology used for noninvasive skin tightening and lifting. Microfocused ultrasound uses different frequencies of acoustic sound that converge and exert their effect below the epidermis, bypassing the need for invasive surgery. This modality focuses ultrasound waves to specific areas in both the dermal and subcutaneous tissues, creating tiny thermal coagulation points. Browlifting, improvement in wrinkles, and skin tightening can all be achieved by adjusting the energy and depth of the emitted sound. In addition to the potential benefits to the face and neck, microfocused ultrasound can also be used on regions including the thighs, upper arms, and knees. Microfocused ultrasound combined with imaging has also been shown to be beneficial in the removal of hyperactive sweat glands in patients with hyperhidrosis, the effects of which were shown to last more than 12 months.15,16 The ideal microfocused ultrasound patient has mild to moderate skin and soft tissue laxity. Because microfocused ultrasound patients have increased wound healing capacity, younger patients are favored. Similarly, patients with extensive photodamage, severe skin laxity, and dramatic platysma banding are poorer candidates and, comparatively, will require a more aggressive approach. Relative contraindications of microfocused ultrasound include infections/wounds, severe acne, or the possession of metallic objects within the treatment area such as cardiac pacemakers and defibrillators. Relative contraindications also include treatment areas containing keloids, permanent dermal fillers, or patients with risk factors that inhibit proper wound healing such as uncontrolled diabetes or chronic tobacco smokers.15 • Axillary hyperhidrosis • Soft tissue laxity • Mild to moderate rhytides • Photodamage • Platysmal banding • Infections • Open skin lesions • Severe acne • Metallic implants Intense pulsed light (IPL) uses a broad wavelength of noncoherent light to exert nonablative effects on many cell types. The photobiology is not as well understood, but the procedure appears to affect many more chromophores and cell types due to a wider spectrum. In theory, this may have a greater and more thorough potential for exerting a regenerative effect. IPL is ideal for photodamage-associated dyschromia and telangiectasia as well as mild rhytides and the improvement of large pores. IPL has many advantages compared to laser-based technologies. There is minimal downtime when undertaking an IPL procedure. It can be performed during the patient’s lunch break with the patient returning directly back to work after completion of a session. In addition to being used on the face, IPL can be used on the chest, neck, and hands. Moreover, IPL can penetrate deeper tissues than most laser-based technologies and yet maintains a reduced risk for purpura and hyperpigmentation. The benefit for using IPL to treat rhytides is modest when compared to laser-based therapies, but the relative safety profile of IPL is unmatched. More often, however, IPL is used to remove hair, treat telangiectasias, improve skin texture, and correct irregular pigmentation.17 The contraindications to IPL are fairly limited. • Hair removal • Vascular lesions • Spider angiomas • Port-wine stains • Broken facial veins • Rosacea • Pigmented lesions
14.1 Introduction
14.2 Patient Selection
14.2.1 Dermal Fillers
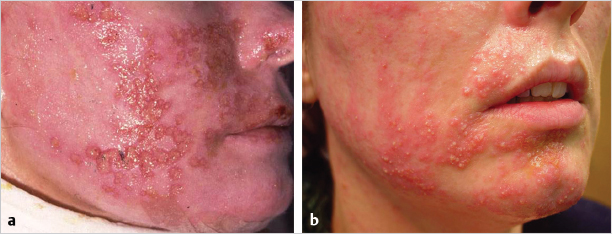
![]() Fig. 14.1). With evidence of any of these organisms, cultures should be obtained, treatment with an appropriate medication should be administered, and resolution should be confirmed before any injections are performed.
Fig. 14.1). With evidence of any of these organisms, cultures should be obtained, treatment with an appropriate medication should be administered, and resolution should be confirmed before any injections are performed.
Indications for Dermal Fillers
Relative Contraindications for Botulinum Toxin
14.2.2 Botulinum Toxin
Indications for Botulinum Toxin
Relative Contraindications for Dermal Fillers
14.2.3 Deoxycholic Acid
Indications for Deoxycholic Acid
Relative Contraindication for Deoxycholic Acid
14.2.4 Laser Resurfacing
Indications for Ablative Laser Resurfacing
Indications for Nonablative Laser Resurfacing
Relative Contraindications for Laser Resurfacing
14.2.5 Microfocused Ultrasound
Indications for Microfocused Ultrasound
Contraindications for Microfocused Ultrasound
14.2.6 Intense Pulsed Light
Indications for Intense Pulsed Light
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


