6 Noninvasive Devices Used in Combination with Volumizing Summary Noninvasive and minimally invasive devices have become very attractive because of their lower risk, less downtime, and more gradual approach to aging. A new trend in combining or offering sequential noninvasive treatments, such as using fillers and lasers together, is gaining in popularity due to the short downtime. A review of the literature is necessary, because the amount of information regarding the use of fillers and other treatments, and the safety of such combinations, should be extensive. However, the information is sparse. This chapter provides some guidelines for patient selection and tips when performing multiple treatments. Keywords: Botulinum toxin type A, combination treatments, devices, fillers, lasers, noninvasive, resurfacing Key Points • The patient population is seeking more nonsurgical treatment options with less downtime, resulting in high demand for concomitant procedures. • The scientific literature is starting to demonstrate safety and efficacy of the concurrent use of various treatments. • Proper patient selection and consultation is imperative when determining the best combination and sequence of noninvasive or minimally invasive procedures. Facial aging is the result of a complex combination of multiple factors, and our professional understanding of this process continues to expand. The visible signs of aging are a combination of, among other factors, fat loss and redistribution, bony resorption, and collagen/elastic tissue denaturation. If all of these elements are not dealt with in proper combination, patients may be deprived of their optimal potential outcomes. Although the field of both invasive and noninvasive cosmetic procedures is growing exponentially, the most notable and recent advancements lie within the noninvasive and minimally invasive categories, which is reflective of patient demand. In fact, the American Society of Plastic Surgeons’ (ASPS) statistics for 20141 demonstrated the greatest rise since the prior year within the cosmetic minimally invasive procedures category. Within this category, botulinum toxin type A (Botox) and soft tissues fillers remain in the top two, but lasers such as those for resurfacing (both ablative and nonablative) continue to rise, increasing 6% from 2013 (see product Index and Video 2.3).1Patients are seeking procedures with lower risk profiles, less downtime, and a more gradual approach to enhancing the aging process. Patients are also undergoing procedures at an earlier age, leading to the demand for noninvasive procedures that produce more subtle, yet preventative results. If a procedure requires downtime, the emphasis is to minimize the duration, thus there is increased importance on completing multiple procedures in the same session. This new trend is changing the way many physicians address facial aging. There are several hesitancies that prevent a practitioner from performing sequential treatments, such as the possibility of changing the properties of the filler, leading to diminished effectiveness or potentiating the risk of both short- and long-term side effects. The package inserts approved by the U.S. Food and Drug Administration (FDA) for both filler substances and devices include warnings against using other procedures in conjunction with their products. For example, injectable poly-L-lactic acid (injectable PLLA, Sculptra Aesthetic) warns against the use of any laser or procedure based on “active dermal response” due to “possible risk of eliciting an inflammatory reaction at the implant site.”2 The insert of the microfocused ultrasound (MFUS) device Ulthera states that there has not been an evaluation of use over materials, therefore “treatment is not recommended directly over those areas with any of the following: mechanical implants, dermal fillers, implanted electrical devices” (see Product Index (p. 185) and Videos 2.1 and 2.2).3 There is no mention of a suggested time frame for using procedures in combination, except for recommendations to allow for complete healing and waiting until the effects are completely realized before proceeding with other procedures. Clinically, complete healing can take up to 6 months for certain treatments, making this timeline unrealistic and undesirable for patients with several cosmetic concerns to address. The question facing the practitioner is not if one can combine noninvasive treatments, but if and when it is safe to do so. As one can see, the combination of treatments is not black and white, and safety concerns from the FDA approvals have not been corroborated to date within the literature. Fortunately, investigations are slowly being published to help answer some of these questions, which may help guide the clinician. The scientific literature is beginning to explore the effectiveness and safety of sequential treatments, but concrete conclusions remain sparse. Our goal is to evaluate the existing evidence for these combinations and to create practical methods based on these scientific principles. When trying to conceive the ideal plan for combining noninvasive treatments, it is paramount to review the literature pertinent to these combinations. One of the earliest investigations of combining noninvasive treatments was conducted in 2005 by England et al4 to determine the effects of monopolar radiofrequency (RF) treatment over soft tissue filler in an animal model. Monopolar RF is known to have a depth of heating dependent on the geometry of the electrode, with the 1.5 cm2 hand piece penetrating up to 8 mm, making it one of the deepest modalities. At this depth, it is especially important to investigate its use over dermal fillers, because it would contact the filler substance placed more superficially. Using monopolar RF, they [England et al.] investigated, through histology, the effects on various filler substances when used either at the same time as the RF treatment or 1 month after treatment within a juvenile pig model.4 The five filler substances used were 1. Cross-linked human collagen. 2. Hyaluronic acid (HA). 3. Calcium hydroxylapatite (caHA). 4. Poly-L-lactic acid (PLLA). 5. Liquid silicone. The filler substance was injected from the middle to deep dermal layer down to the subcutaneous tissue, depending on the substance and placement typically employed during cosmetic applications. The monopolar RF treatment was performed at relatively high settings (1.5 cm2 treatment tip, 130 and 162 J, 3 passes). Histologic evaluations done sequentially up to 4 months after treatment did not demonstrate any decrease in filler persistence. Moreover, there were no increased adverse events seen clinically due to bulk heating. Therefore, in this animal model, the various filler substances did not change the conductivity of the RF treatment and cause unwanted thermal effects. Over the 4-month follow-up, histology demonstrated trends, although not statistically significant, toward an increased collagen response with HA, PLLA, and caHA when combined with the RF procedure. In a follow-up study, Shumaker et al5 found significant increases in the foreign body, inflammatory, and fibrotic responses associated with these fillers when treated sequentially with monopolar RF over those treated with RF alone at the 1-month follow-up. It is possible that these changes led to the trend toward increased collagen response seen in their previous study, but this is unable to be confirmed.4,5 Further, Kim et al6 found a greater change in the wrinkle severity score and an increase in procollagen production when RF was applied prior to HA filler placement in both a human model and an animal model, respectively. In human tissue, Alam et al7 injected HA and caHA filler to the upper arm and performed monopolar RF treatment (1.5 cm2treatment tip, 63.5 setting, 2 passes) to the same area 2 weeks later. A control subject did not receive the RF treatment over the injected filler. Within punch biopsy specimens obtained 3 days after the RF treatment, there were no differences seen with light microscopy and digital photomicrographs of the filler substance between areas treated with RF and those areas not treated with RF. There were no differences in signs or symptoms between the control and experimental groups, except a slight transitory pain reported when RF was delivered over the filler.7 Beyond RF treatments, Farkas et al8 examined the histologic effects of several light and laser-based technologies on filler substances in an animal model. HA filler was placed within the dermis of a pig model, and then 2 weeks later, the same area was given one of seven different lasers/light devices. These devices included (see Product Index (p. 176)) • Intense pulsed light (IPL) 560 nm filter (Sciton, Inc.). • Nd:YAG 1,064 nm (Sciton, Inc.). • Er:glass 1,540 nm (Lux1540, Palomar Medical Technologies, Inc.). • erbium 2,940 nm (ProFractional, Sciton, Inc.). • Er:YAG 2,940 nm (Palomar Medical Technologies, Inc.). • CO2 10,600 nm (ActiveFX and DeepFX, Lumenis). Within the 8 mm punch biopsies performed immediately after the laser treatment, there were no signs of interaction of the filler and laser when using the superficially reaching devices, but there was clear interaction when treating with the deep ablative systems (Er:YAG 2,940 nm and CO2). On histology, the microablative columns created by the laser were interspersed in the pool of filler. Some of the HA filler was seen to migrate into the ablated microchannels or was trapped within collapsed ablated columns in the reticular dermis. The filler substance itself did not show any denaturation or significant morphologic changes, even at higher energy settings.8 A similar study was performed on human skin by Goldman et al,9 who investigated the effects of HA filler followed by a laser or light device in a split-face study, randomized trial. Thirty-six patients received HA filler to the nasolabial folds and postauricular area, followed by either 1,320 nm Nd:YAG, 1,450 nm diode, monopolar RF, or IPL with a 560 nm cutoff filter on one side over the filler. After sequential biopsies over 28 days, there were no significant differences in histology demonstrating damage to the filler, although sampling was an issue within this study, because several biopsies did not demonstrate any filler on histology in either the group treated with an energy device or the group not treated with an energy device. There were no reported adverse events related to overlapping any of the devices over the filler on the same day.9 Another deeply penetrating device is the MFUS, which is frequently used for tissue tightening on the face, neck, and chest. MFUS is able to penetrate up to 4.5 mm while employing a commonly used treatment hand piece. Friedmann et al10 reported the efficacy and safety of using sequential IPL, then MFUS, followed by PLLA injection, in one treatment session on the face. The sequence of procedures, as noted, was chosen specifically to avoid potential increased energy absorption secondary to erythema from MFUS, if IPL was performed afterward. The authors did mention that if MFUS and IPL were not performed on the same day, they would wait 2 weeks before performing MFUS following any PLLA injection to allow for the swelling to subside. A case review by Hart et al11 demonstrated similar findings in which MFUS and PLLA were used in different areas (face, chest, and back) on the same day. They performed the MFUS procedure first to avoid the water from the PLLA displacing the tissue depth being targeted and to prevent blood contamination of the transducer. There were no increased adverse events from the combination treatment, even when treating the neck and chest. A larger dilution of PLLA, 16 cc in these cases, was used when treating the chest.10,11 In another study of the combination of device and filler treatment on human skin, Casabona and Michalany12 injected both HA and caHA into the inner thigh and studied the histologic effects of MFUS performed over the site. With a control area of filler without MFUS treatment, biopsies were compared at days 0, 15, 30, and 180. There were no significant differences in the inflammatory process or product migration. In comparing qualitative neocollagenesis and neoelastinogenesis, the retroauricular area of the same patient was injected and treated with MFUS, and a control area was left untreated with the device. Histologic samples stained with Masson’s trichrome stain and Verhoff von Giesen stain at day 60 showed an increase in density of the collagen fibers in the areas treated with both fillers and the device simultaneously as compared to the control area in this patient. There were no adverse events noted in the study, and there was no difference in the clinical appearances between the experimental and control areas.12 Park et al13 performed a split-face study of the use of HA filler (Teosyal, Teoxane Laboratories) alone to the nasolabial fold versus concomitant HA filler with a nonablative infrared (IR) device (Titan, Cutera, Inc.). Each of these modalities alone had been shown to improve the clinical appearance of these studied areas. The histologic findings on each side were similar, and there was preservation of filler at the deep dermal–subcutaneous junction. There were no increased adverse events among the 12 patients receiving combination treatment, yet there were also no significant clinical improvements using combination treatment over HA filler alone.13 Finally, more well-known, widely used, and important to acknowledge is the combination of botulinum toxin and laser. Treatment with the toxin in the same area treated by a laser has been shown to decrease the degradation of filler, which resulted in a higher volume remaining at the end of muscle paralysis in an animal model.14 With treatment on the hand, injecting toxin 1 week prior to resurfacing improved healing of the skin after resurfacing.15,16 A small study of 10 female patients showed that botulinum toxin injection to the glabella, forehead, and crow’s-feet to one side of the face 1 week prior to full-face laser resurfacing resulted in greater improvement on the combination-treatment side.16 Additional studies with botulinum toxin injection 1 day to 2 weeks prior to fractional resurfacing demonstrated similar results.17,18,19 Treatment with botulinum toxin injection immediately prior to IPL, nonablative lasers, and radiofrequency devices, in contrast, did not reveal any adverse events.19,20 On the other hand, the diffusion of botulinum toxin to the neighboring zygomatic muscle when treating periorbital rhytides with neuromodulator and CO2 ablative resurfacing same day has also been reported.21 We can see from the review of the literature that heat generated during a procedure does not change the basic morphology of the filler substance. Further, we know that collagen denaturation occurs at approximately 55 to 70 °C and that temperatures reached within the targeted tissue for devices are estimated to be 50 to 65 °C for neocollagenesis and the tissue-tightening effect.4 The HA fillers are sterilized during manufacturing at 120 °C, therefore enduring much higher temperatures without changes to its stability.9 It is equally important to note that the energy from the device and filler most often do not significantly interact. Theoretically, midface volumizers properly placed at the preperiosteal plane would be below the depth of penetration of the noninvasive devices, as would fillers placed in the deep reticular dermis (
6.1 Introduction
6.1.1 Literature Review of Combination Noninvasive Treatments
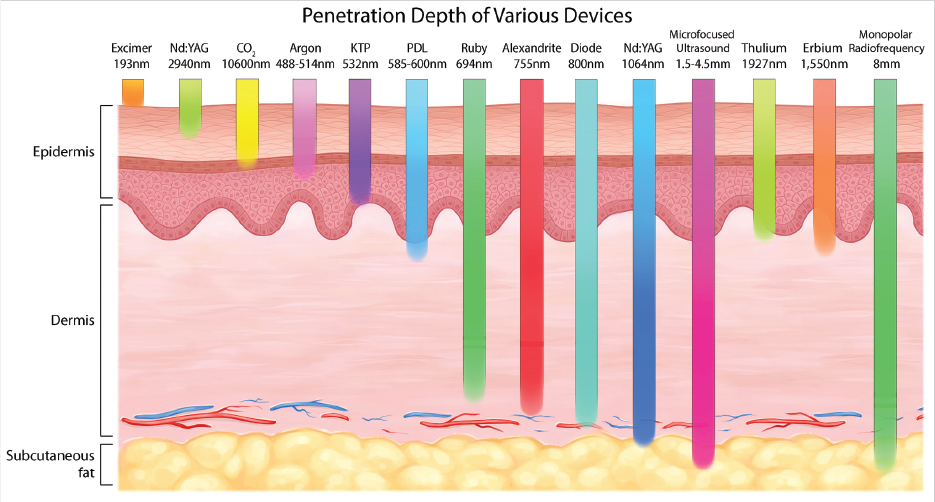
![]() Fig. 6.1). Further, what may be important to consider is the type of device, because the longevity of HA and caHA placed from the subcutaneous plane to the superficial dermis did not demonstrate decreased longevity over 6 months when used in combination with the MFUS device, yet dissolution of a caHA nodule inadvertently placed superficially in the dermis was witnessed with the CO2 device. Reddy et al22 described a case successfully employing a CO2 laser to dissolve a misplaced nodule of caHA. The patient experienced a visible nodule of caHA immediately after injection of this filler to the tear trough area, a location typically not injected with this filler substance. After one session of CO2 fractionated ablative resurfacing, performed 6 months after the initial injection, complete clinical resolution at the 2-week follow-up was seen.22 The depth of penetration for the CO2 device is more superficial than the MFUS device, and therefore greater interaction was noted in these examples. The extent to which placement depth impacts longevity of the product after a particular combination treatment requires further evaluation; however, safety does not seem to be affected.
Fig. 6.1). Further, what may be important to consider is the type of device, because the longevity of HA and caHA placed from the subcutaneous plane to the superficial dermis did not demonstrate decreased longevity over 6 months when used in combination with the MFUS device, yet dissolution of a caHA nodule inadvertently placed superficially in the dermis was witnessed with the CO2 device. Reddy et al22 described a case successfully employing a CO2 laser to dissolve a misplaced nodule of caHA. The patient experienced a visible nodule of caHA immediately after injection of this filler to the tear trough area, a location typically not injected with this filler substance. After one session of CO2 fractionated ablative resurfacing, performed 6 months after the initial injection, complete clinical resolution at the 2-week follow-up was seen.22 The depth of penetration for the CO2 device is more superficial than the MFUS device, and therefore greater interaction was noted in these examples. The extent to which placement depth impacts longevity of the product after a particular combination treatment requires further evaluation; however, safety does not seem to be affected.
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine