The Clinical Problem
See Fig. 33.1 .

The Aesthetic Problem
A patient will present at surgery with a number of perceived concerns about their abdominal area. Often, this is a surplus of unwanted subcutaneous fat, visceral fat, loose skin, lack of definition, a so-called muffin top overhang in clothing, and a general dislike of the midsection. It is usual for more than one issue to present itself, especially if the patient is female and postchildbirth. where separation of muscle and stretch marks can also contribute to the general paunch in this area.
The aesthetic concern is that the patient is fed up with how the midsection looks. She or he dresses to hide the perceived figure flaw, wearing loose clothing or avoiding some styles of clothing altogether (e.g., bikini, swimwear) for fear of exposing the problem area to others. Patients explain that they cannot buy clothes that fit properly because the midsection area is proportionally larger than the rest of them, so they take to dressing to disguise the area. Behavioral changes such as these are a sign that this is affecting them psychologically and that their concerns are genuine and warrant assessment and possible action.
During a consultation, a physical assessment of the patient will take place so that the area can be assessed and treatment options given. It is important to understand that the patient may struggle to verbalize the concerns and, instead, prefer to grab at the midsection to highlight what they do not like. Understanding their concerns and what they see as aesthetically pleasing for this area is vital at the consultation stage to ensure that their expectations are managed and to give a realistic visual of any expected outcome following treatment. The midsection will show loss of definition, with a layer of unwanted subcutaneous fat covering the abdominal wall and causing a swollen look. There may or may not be loose sagging skin and, in some cases, a combination of both these factors causes an apron or overhang effect. The patient will be able to grab fat and will talk of wanting a flatter, smoother silhouette. The consultation will take into consideration the patient’s anatomy, what they present with, and an outcome of fat reduction and skin tightening that is realistic and achievable.
Surgical Preparation and Technique
Management and Treatment Options
It may be that you can offer surgical and nonsurgical treatments to give the patient the outcome they desire. Explaining the risks and benefits of both types of treatment is key at this stage. A better outcome may be possible surgically for some patients, but they may not wish to risk the complications that can accompany surgery, such as the risk of being anesthetized, downtime, long recovery period with the necessary time off work, and even the cost of the procedure. Sometimes, the patient may believe that aesthetic surgery carries a stigma and is frowned on by friends and family.
At this stage, discussions about more discrete noninvasive treatments can take place, along with discussing any risks associated with these treatments and any limitations that they may have. There are systems that use ultrasound for noninvasive fat loss, but downtime may be increased with such treatments. Studies have shown that the use of multipolar radiofrequency (RF) can cause apoptosis of fat cells without damaging surrounding tissue, with no downtime. A course of treatments using BTL Vanquish ME (BTL Industries, Framingham, MA), which is a system that uses noncontact multipolar RF to treat subcutaneous fat, may be better suited to these clients. Once again, managing patient expectations and ensuring that they are aware of the type of end result they can expect is a priority.
With noninvasive fat reduction, we are trying to reduce the amount of subcutaneous fat without causing any damage to surrounding tissue, such as nerve endings, blood vessels, and skin. Devices that freeze fat will often cause necrosis of not only fat cells, but blood vessels and nerve endings in the treated area, causing possible side effects. These may include swelling, bruising, numbness, tingling, or burns, and an approximate wait time of 3 months before final results are seen. For some, this downtime is suboptimal, despite the fact that fat cell death is permanent in the treated areas. Using multipolar RF reduces the risk of side effects because a device such as BTL Vanquish ME is tuned to the subcutaneous fat. Only fat cells are targeted; there is no damage to surrounding tissue, blood vessels, or nerve endings, so there is no downtime, swelling, pain, or bruising. A simplified operator protocol with zero consumables ensures that results are consistent and deliverable; therefore, a successful outcome with 60% of fat cell death in the treated area is achievable.
Treatment and Operative Technique
The ideal patient for applying the BTL Vanquish ME system has mid to moderate adipose tissue and is within 20 pounds of the ideal weight. Treatments last between 30 and 45 minutes, and a course of four to six treatments is advised for optimal results, spaced 7 to 10 days apart. Sometimes results can be seen as soon as after the first treatment, but the final result is seen 2 to 4 weeks after the last treatment.
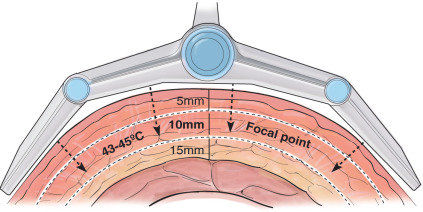
In regard to the depth of penetration, the focal point is approximately 10 mm below the surface. It uniformly heats approximately 5 to 15 mm to 43°C to 45°C (109.4°F to 113°F), causing the apoptosis of fat cells ( Fig. 33.2 ).