Seroma formation is one of the major postoperative complications of abdominoplasty. Progressive tension sutures have been proposed as an adjunct procedure to combat this problem. Apart from being a simple addition to abdominoplasty, the sutures also eliminate other complications, such as postoperative drains, and increase the patient’s mobility.
Seroma is one of, if not the most frustrating problem that plagues abdominoplasty. Many theories have been proposed as to the cause of seroma, and various techniques have been suggested to control this complication. These techniques range from operative variations, such as limitation of undermining, elimination of concurrent liposuction and tissue glues; to postoperative practices such as extended bed rest, limitation on upright posture, and use of compressive garments. All of these methods have their limitations and none have eliminated seromas.
The authors first described the concept of progressive tension sutures (PTS), an advancement of the abdominal flap that affixes the superficial fascia to the deep fascia in an advanced position. This technique permits the elimination of postoperative drains, increases patient mobility, and permits early resumption of an erect posture while preventing seromas and reducing other local complications. The technique has been refined for abdominoplasty and extended to various procedures (browlift, facelift, latissimus donor site) that use an advancement flap.
The use of sutures to coapt 2 tissue surfaces and close the intervening dead space is not a new concept. Mladick noted in a commentary that Georgiade, in his textbook, described the use of “tacking sutures” to advance the flap and prevent fluid collection in abdominoplasty. Mladick has said “that this is an important step that should be used in every abdominoplasty.” Baroudi and Ferreira reported the use of “quilting sutures” to close dead space in the prevention and treatment of seromas in abdominoplasty. The authors acknowledges the similarity of tacking, quilting, and PTS as variations on a theme, and the significant contribution of Baroudi, Georgiade, and other investigators in the evolution of this concept. In the authors’ experience, PTS is a simple and efficient adjunct procedure that can be easily integrated into most current abdominoplasty techniques to reduce local complications. In addition, the logic of PTS is easily understood and patients have enthusiastically accepted the elimination of postoperative suction drains.
In this article, the concept of PTS and the theories behind their effectiveness is reviewed, the technique is elucidated, and the related literature is reviewed. The authors share their practices and clinical data supporting the use of PTS.
Concept and function of PTS
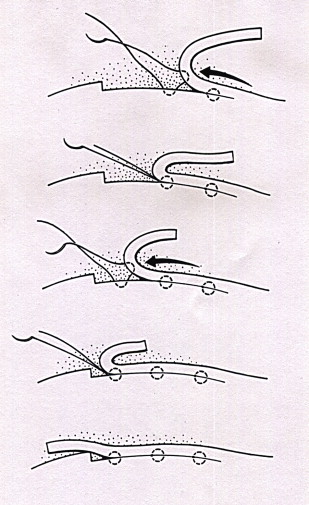
A PTS procedure is not an operation, but simply an adjunct to the abdominoplasty procedure that can be used with most current techniques. As the abdominal flap is advanced, it is secured in an advanced position by sutures placed between the superficial and the deep fascia. As each suture is placed in succession, tension is transferred distally and the flap is advanced ( Fig. 1 ). Tension is placed on the superficial fascial system and not on the skin and its underlying subdermal plexus. The tension is distributed not only at the vulnerable distal flap but over the broad area of the flap.
The concept of PTS is simply an adaptation of basic surgical principles, which include reduction of dead space and the facilitation of wound healing by minimizing tension, and secure fixation of the wound surfaces. The methods by which PTS may act to control complications can be understood by examining the various aspects (dead space, flap tension, and shearing forces) in relation to the abdominoplasty procedure.
Dead Space
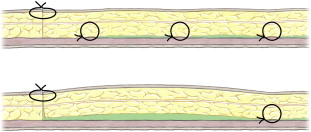
Dead space is often considered as the root cause of seroma formation in abdominoplasty. The large cavity that is created in abdominoplasty and other procedures that use advancement flaps plays a definite role in seroma formation. The placement of PTS divides this dead space into smaller areas or compartments and limits fluid accumulation ( Fig. 2 ). Several recent studies using ultrasonography demonstrate this compartmentalization.
Tension
In the standard abdominoplasty approach, the tension of advancement is placed on the distal portion of the flap, which is most vulnerable to circulatory compromise. PTS secure the superficial fascia with the deep fascia, distributing the tension over a broad surface area and transferring the tension to these 2 strong layers. The important subdermal plexus is superficial to the level at which tension is applied and thus, the circulation to the distal flap is theoretically protected. That there is excellent dermal bleeding and therefore clearly adequate circulation is apparent to the surgeon when the excess skin is excised following advancement with PTS. The observation that distal circulation is protected by PTS warrants further study. Further, minimizing tension on the skin incision potentially improves the quality of the scar and minimizes superior migration of the scar and the mons pubis.
Shearing Forces
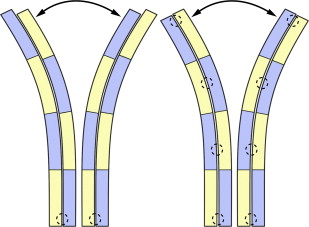
In the standard abdominoplasty, the advanced flap and the muscle fascia are attached only at the level of the incision and are free to move relative to each other as the patient moves. Sliding movement between these two tissues can occur with change of patient position, ambulating, coughing, or even breathing. It is likely that this repeated disruption of early healing and increased inflammation may be the primary cause of seroma formation. The addition of PTS provides a secure fixation of the superficial fascia to the deep fascia, producing a single structural unit and eliminating disruption of early healing because of patient movement ( Fig. 3 ). It is the authors’ opinion that this is the chief mechanism by which PTS prevent the formation of seromas in abdominoplasty.
Aesthetic Results
Many surgeons limit undermining and liposuction procedures because of fears of complications such as necrosis and seroma. The final result is therefore compromised or the patient is required to undergo a second procedure for abdominal liposuction. The addition of PTS permits adequate undermining and allows for liposuction to be performed at the time of abdominoplasty. A further aesthetic benefit is the midline contouring seen in the PTS abdominoplasty. The suture placement and flap tension primarily placed on the midline create a distinct contour ( Fig. 4 ).

Another aesthetic benefit regarding the insetting of the umbilicus is that when PTS are used the umbilicus may be inset from the undersurface, in continuity with flap advancement. Three-point sutures are used to affix the dermal edges of the umbilicus and abdominal skin down to the muscle fascia, which draws the scar into the depths of the neo-umbilicus and securely splints the scar. The sutures create an attractive umbilical dimple, hide the scar, and prevent its contracture.
Technique
PTS are simply an adjunct to the abdominoplasty procedure and can be adapted to most current techniques. The stress is on the principles of closing or minimizing of dead space and firmly affixing the flap to the deep fascia to prevent shear. Individualization based on patient’s aesthetic needs and surgeon’s judgment dictate operative details such as degree of undermining, amount and location of liposuction, and even whether or not to place drains. A general description of PTS technique follows, which varies depending on patients.
Liposuction can be performed before flap elevation or at the end of the case. Liposuction of the flap itself is limited to below Scarpa’s fascia. Epigastric suctioning is done with caution because of concerns for injury to the blood supply to the flap and aesthetic oversuctioning. What appears as a thick epigastrum before advancement thins significantly once the flap is advanced. The extent of undermining is limited to the amount needed to achieve the aesthetic needs of the individual patient. Likewise, rectus diastasis repair is dictated by patient needs. Repair is done in 2 layers; the first interrupted, then with running 0-0 braided nylon.
The use of a continuous local anesthetic infusion pain catheter using 0.25% marcaine without epinephrine has been very helpful in postoperative pain control. The catheters are inserted in the subxyphoid area in a retrograde fashion and can therefore be reused ( Fig. 5 ). The same retrograde technique is used to place the catheters into the rectus sheath on either side of the umbilicus. Care should be taken to avoid damage to the catheter with later placement of PTS. The fascia is generously infiltrated with marcaine and the catheters are primed with about 5 mL of marcaine at the end of the case.
PTS are conceptually easy to place but do require some practice to increase ease and speed of placement. Coordination between the surgeon and an assistant is the key to simplicity of placement of sutures and decreased operative time ( Fig. 6 ). The surgeon uses the nondominant hand to advance the flap. A large Richardson-type retractor in the upper abdomen held by the assistant may aid this procedure. The first suture is placed in the midline at the highest point of the dissection. Care is taken to place the suture deep enough to include Scarpa’s fascia. A bite of tissue closer to the dermis is not a concern in the midline, as this may produce a midline crease that may be aesthetically desirable. In the lateral aspects of the flap, superficial suture placement may result in dimpling and should be avoided. With the suture placed in the flap, the surgeon advances the flap with the nondominant hand to the spot where it is to be secured. The exact degree of advancement is based on the surgeon’s judgment. The suture is then place in the deep fascia at this spot or slightly (1 cm) distal, to account for fascia mobility. This procedure is repeated until the umbilical stalk is encountered. Above the umbilicus, only 2 to 3 midline sutures are typically placed. Commonly, 0-0 vicryl is used on a large needle but 2-0 vicryl may be sufficient if the skin flap is thin. The CTX (Ethicon) needle is especially helpful.
Related posts:
 Anatomic Considerations in Abdominoplasty
Anatomic Considerations in Abdominoplasty
 Editorial Comment on “Traditional Abdominoplasty”
Editorial Comment on “Lipoabdominoplasty: The Saldanha Technique”
Editorial Comment on “ SAFECircumferential Liposuction with Abdominoplasty”
Editorial Comment on “Concepts on Correction of the Musculoaponeurotic Layer in Abdominoplasty”
Revision Abdominoplasty and Proper Umbilical Positioning
Editorial Comment on “Traditional Abdominoplasty”
Editorial Comment on “Lipoabdominoplasty: The Saldanha Technique”
Editorial Comment on “ SAFECircumferential Liposuction with Abdominoplasty”
Editorial Comment on “Concepts on Correction of the Musculoaponeurotic Layer in Abdominoplasty”
Revision Abdominoplasty and Proper Umbilical Positioning
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


