Key Words
nevi, malignant melanoma, atypical nevus, dysplastic nevus, blue nevus, speckled lentiginous nevus, halo nevus, moles, ABCDs of melanoma, lentigo, dermatofibroma
Melanocytic Nevi
Nevi, or moles, are benign tumors composed of nevus cells that are derived from melanocytes. Many myths surround moles, for example, that hairs should not be plucked from moles or that moles should not be removed or disturbed.
Nevus Cells.
The nevus cell differs from melanocytes. The nevus cell is larger, lacks dendrites, has more abundant cytoplasm, and contains coarse granules. Nevus cells aggregate in groups (nests) or proliferate in a non-nested pattern in the basal region at the dermoepidermal junction. Nevus cells in the dermis are classified into types A (epithelioid), B (lymphocytoid), and C (neuroid). Through a process of maturation and downward migration, type A epidermal nevus cells develop into type B cells and then into type C dermal nevus cells.
Incidence and Evolution.
Moles are so common that they appear on virtually every person. They are present in 1% of newborns and increase in incidence throughout infancy and childhood. The incidence peaks in the fourth to fifth decades. Nevi then diminish in number with advancing age.
Size and pigmentation may increase at puberty and during pregnancy. Nevi may occur anywhere on the cutaneous surface. There is a strong correlation between sun exposure and the number of nevi. Acquired nevi on the buttocks or female breast are unusual.
Nevi Versus Melanoma.
Nevi exist in a variety of characteristic forms that must be recognized to distinguish them from malignant melanoma. Except for certain types, such as large congenital nevi and atypical moles, most nevi have a very low malignant potential.
Nevi vary in size, shape, surface characteristics, and color. The important fact to remember is that each individual nevus tends to remain uniform in color and shape. Although various shades of brown and black may be present in a single lesion, the colors are distributed over the surface in a uniform pattern.
Melanomas consist of malignant pigment cells that grow and extend with little constraint through the epidermis and into the dermis. Such unrestricted growth produces a lesion with a haphazard or disorganized appearance, which varies in shape, color, and surface characteristics. The characteristics of uniformity cannot always be relied on to differentiate benign from malignant lesions because very early melanomas may appear quite uniform, having a round or oval shape with a uniform brown color.
Examination With a Hand Lens and Dermoscope.
Careful inspection of suspicious lesions with a powerful hand lens and dermoscope will reveal a number of features that cannot be appreciated with the naked eye. Dermoscopy is discussed at the end of the chapter.
Common Moles
Nevi may be classified as acquired or congenital, but a clinical classification based on appearance and conventional nomenclature is used here. Common acquired nevi appear after 6 months of age. They enlarge and increase in number through the third and fourth decades and then slowly disappear. Most are less than 5 mm in diameter. Fifty-five percent of adults have between 10 and 45 nevi greater than 2 mm in diameter. Nevi tend to be concentrated on sun-exposed sites.
Classification.
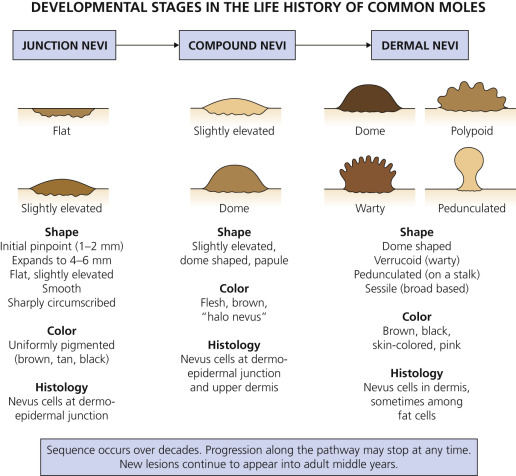
Common moles are subdivided into three types – junction, compound, and dermal – based on the location of the nevus cells in the skin ( Fig. 22.1 ). The three types represent sequential developmental stages in the life history of a mole. During childhood, nevi begin as flat junction nevi in which the nevus cells are located at the dermoepidermal junction. They evolve into compound nevi when some of the cells migrate into the dermis. Migration of all of the nevus cells into the dermis results in a dermal nevus. Dermal nevi usually form only in adults, but this evolution does not consistently occur. Nevi with cells confined to the dermoepidermal junction area tend to be flat, whereas those with cells confined to the dermis are usually elevated.
Junction Nevi.
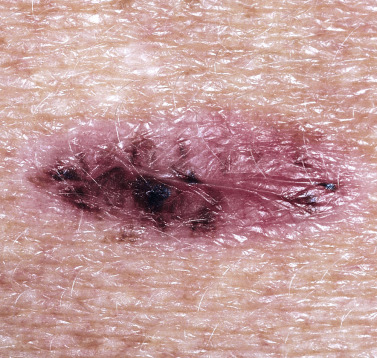
Junction nevi are flat (macular) or slightly elevated, and they are light brown to brown-black with uniform pigmentation that may be slightly irregular ( Fig. 22.2 ). The surface is smooth and flat to slightly elevated, and the border is round or oval and symmetric. Most lesions are hairless. Junction nevi vary in size from 0.1 to 0.6 cm; some are larger. Junction nevi may change into compound nevi after childhood, but they remain as junction nevi on palms, soles, and genitalia. Junction nevi are rare at birth and generally develop after the age of 2 years. Degeneration into melanoma is very rare.

Compound Nevi.
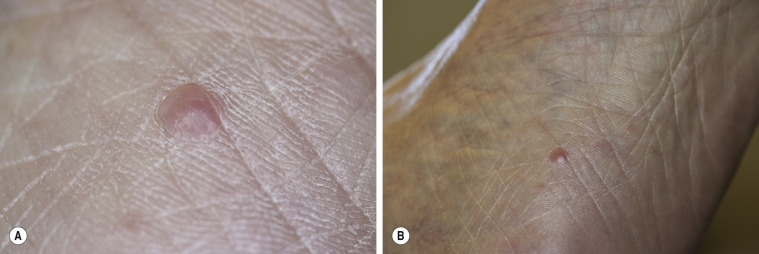
Compound nevi are slightly elevated and skin-colored or brown. They are elevated and smooth or warty and become more elevated with increasing age ( Fig. 22.3 ). They are uniformly round, oval, and symmetric. Hair may be present. If a white halo appears at the periphery of the lesion, it is referred to as a halo nevus.

Dermal Nevi.
Dermal nevi are brown or black, but may become lighter or skin-colored with age. Lesions vary in size from a few millimeters to a centimeter. The variety of shapes reflects the evolutionary process in which moles extend downward with age and nevus cells degenerate and become replaced with fat and fibrous tissue.
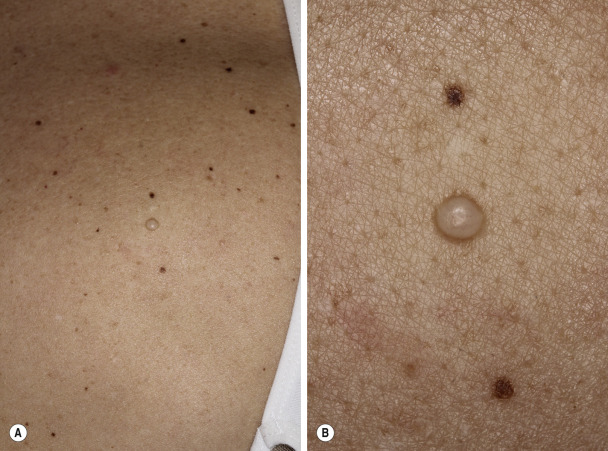
Dome-shaped lesions are the most common ( Figs. 22.4 to 22.6 ). They generally appear on the face and are symmetric, with a smooth surface. They may be white or translucent, with telangiectatic vessels on the surface mimicking basal cell carcinoma. The structure may be warty ( Fig. 22.7 ) or polypoid ( Fig. 22.8 ). Pedunculated lesions with a narrow stalk are located on the trunk, neck, axillae, and groin. They may appear as a soft, flabby, wrinkled sack ( Fig. 22.9 ). Solitary cutaneous mucinosis, spiradenoma, eccrine poroma, and palisaded encapsulated neuroma can mimic dermal nevi ( Figs. 22.10 to 22.13 ![]() ).
).








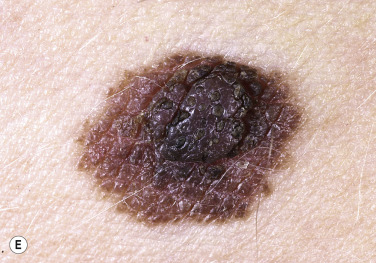
Elevated nevi are exposed and are prone to trauma from clothing and other stimuli, often causing them to bleed and inflame, making some patients suspect malignancy. A white border may appear, creating a halo nevus. Degeneration to melanoma is very rare, but dermal nevi may resemble nodular melanoma (NM); therefore knowledge of duration and a history of recent change is important.
Management
Suspicious Lesions.
Any pigmented lesion suspected of being malignant should be biopsied or referred for a second opinion. Suspicious lesions should be completely removed by excisional biopsy down to and including subcutaneous tissue.
Nevi.
Patients frequently request removal of nevi for cosmetic purposes. It is good practice to biopsy all pigmented lesions; therefore total removal by electrocautery should be avoided. Nevi are removed either by shave excision or by simple excision and closure with sutures. Most common nevi are small and shave excision is adequate.
Recurrent Previously Excised Nevi (Pseudomelanoma).
Weeks to months after incomplete removal of a nevus, brown macular pigmentation may appear in the scar ( Fig. 22.14 ). Some nevus cells remain with shave excision and partial repigmentation is possible. Residual pigmentation may be removed with electrocautery or cryosurgery. An unusual histologic picture resembling melanoma (pseudomelanoma) may follow partial removal of nevi. If the repigmented area is excised, the pathologist should be notified that the submitted tissue was acquired from a previously treated area. Histologically, the melanocytes appear atypical but are confined to the epidermis, and there is no lateral spread of individual melanocytes as is seen in melanoma.
Nevi With Small Dark Spots.
A small percentage of small dark spots within melanocytic nevi (MNs) are due to melanoma. These roundish areas of brown or black hyperpigmentation measure 3 mm or less in diameter and are located peripherally. Biopsy specimens of nevi with small dark dots should be sectioned to ensure histologic examination of this focus of hyperpigmentation.
Special Forms
Special forms of pigmented lesions include congenital nevus, halo nevus, speckled lentiginous nevus, Becker nevus, Spitz nevus, blue nevus, labial melanotic macules, and atypical nevi (dysplastic nevi, Clark nevi).
Congenital Melanocytic Nevi.
It is estimated that between 1% and 6% of the population have a congenital melanocytic nevus (CMN). Congenital melanocytic nevi (birthmarks) are present at birth and vary in size from a few millimeters to several centimeters, covering wide areas of the trunk, extremity, or face. Some lesions first become apparent during infancy. Not all pigmented lesions present at birth are CMNs; café-au-lait macules and neurofibromas may also be present at birth. Congenital nevi may contain hair; if present, it is usually coarse. Such nevi are uniformly pigmented, with various shades of brown or black predominating, but red or pink may be a minor or sometimes predominant color. Most are flat at birth but become thicker during childhood, and the surface becomes verrucous and sometimes nodular. Scalp CMN may lighten with time. Table 22.1 summarizes clinical considerations for CMN.
| Clinical Considerations | Small or Medium CMN | Large CMN |
|---|---|---|
| Size categories | Small: >1.5 cm Medium: M1 – 1.5 to 10 cm, M2 – 10 to 20 cm | Large: L1 – 20 to 30 cm, L2 – 30 to 40 cm Giant: G1 – >40 to 60 cm, G2: >60 cm |
| Risk factors for neurocutaneous melanosis (NCM) | More than 2 medium-sized CMN Multiple satellite nevi | Posterior axial CMN greater than 40 cm |
| Location of melanoma development within the CMN | Dermoepidermal junction | Dermis and deeper tissues, may arise in CNS or retroperitoneum |
| Risk of melanoma | Average risk of 0.7% | Risk increases with the size of the CMN (greatest risk – posterior axial, >60 cm with multiple satellite nevi Lifetime risk of melanoma with CMN larger than 20 cm likely less than 5% |
| Melanoma age of onset | At or after puberty | 70% are diagnosed before the age of 10 |
| Other clinical complications | Cosmetic or psychosocial issues | Cosmetic or psychosocial issues, itching, bulkiness, fragile skin, liposarcoma, rhabdomyosarcoma, and malignant peripheral sheath tumors |
| Methods of excision | Simple or staged excision depending on the size and location of the CMN | Removal of LCMN of the trunk, scalp, and forehead; staged excision to the fascia with previous local tissue expansion for flap reconstruction. Plastic surgery without tissue expanders within the first 1 or 2 years of life can provide good aesthetic and functional results |
| Nonexcisional intervention | Laser therapy can be considered Dermabrasion for superficial CMN Curettage during neonatal period | Laser therapy can be considered Dermabrasion for superficial CMN Curettage during neonatal period |
| Removal considerations | Hypertrophic scarring is possible Laser-induced scarring can occur on extremities and anterior trunk Speckled repigmentation after laser treatment is possible | LCMN can lighten over time, so a scar from removal may end up being more cosmetically noticeable. Repigmentation after superficial removal may result in the same coloration that would have occurred naturally over time. Hypertrophic scarring is possible Laser-induced scarring on extremities and anterior trunk Speckled repigmentation after laser treatment is possible |
| Methods of clinical observation | Visual inspection and dermoscopy, palpation, baseline photographs with measurements | Visual inspection and dermoscopy, palpation for indurated areas, baseline photographs with measurements |
| Considerations whether to observe or excise the CMN | Ease of monitoring the CMN Factors include location of the lesion, degree of hypertrichosis, pigmentation, degree of thickness and topography Size Developmental history of the lesion Anxiety about the CMN Cosmetic or functional concerns | Complete excision of LCMN can be very difficult or impossible depending on the involvement of deeper structures, such as the fascia or muscle, location and size of the CMN. Surgery to remove CMN in a patient with symptomatic neurocutaneous melanosis should be deferred |
| Imaging and consultation considerations for patients with suspected NCM | MRI recommended for patients at risk for NCM with multiple medium CMN or satellites | MRI recommended for patients at risk for NCM with CMN larger than 40 cm and especially if the patient has more than 20 satellites. Consult with a neurologist for patient with signs/symptoms of NCM Consult with a psychologist can be helpful |
Classification.
The diameter of CMNs serves as the major criterion for determining risks of adverse outcomes such as melanoma. Other factors such as diameter, satellite nevus count, anatomic localization, color heterogeneity, surface rugosity, hypertrichosis, and dermal or subcutaneous nodules should be considered when examining CMNs.
Size.
CMNs are divided into groups according to their projected size in adulthood. For example, a 1-cm CMN on the scalp of an infant may enlarge in adulthood to 1.6 cm and is best classified as medium-sized CMN. CMN size categories include small (<1.5 cm); medium (M1: 1.5 to 10 cm, M2: >10 to 20 cm); large (L1: >20 to 30 cm, L2: >30 to 40 cm); and giant (G1: >40 to 60 cm, G2: >60 cm). Satellite nevi (smaller nevi associated with a large or giant CMN) may be grouped by number: S – 0; S1 – <20; S2 – 20–50; S3 >50. Most grow in proportion to the somatic growth of the child. CMNs on the head will increase in size by a factor of 1.7, trunk and extremities 2.8-fold, and lower extremities 3.3-fold.
CMN may be further classified based on 6 anatomical sites: bolero (upper back and neck), back (central back, spares buttock and shoulders), bathing trunk (genital area and buttock, not extending to shoulders or neck), breast/belly (isolated to breast and/or abdomen), body extremity (extremity only), and body (most of body with overlap with bolero and bathing trunk).
Histologic Characteristics.
Nevus cells occur (1) in the lower two thirds of the dermis, occasionally extending into the subcutis; (2) between collagen bundles distributed as single cells or cells in single file, or both; and (3) in the lower two thirds of the reticular dermis or subcutis associated with appendages, nerves, and vessels. Some CMN do not have these microscopic features. Large CMN usually show these classic microscopic findings, whereas small CMN oftentimes do not. Medium-sized congenital nevi may or may not show these classic microscopic features. Large CMN may develop benign proliferative nodules within them. These nodules are very difficult to differentiate clinically and histologically from malignant melanoma.
Malignant Potential.
Melanoma can develop in any CMN and the risk may correlate with the size of the nevus. The malignant potential of congenital nevi may be dependent on the histologic pattern of the lesion rather than the clinical size. Small congenital nevi frequently lack melanocytes in the deeper dermis. The increased risk of melanoma formation in large congenital nevi may be a result of transformation of cells residing deep in the dermis. Melanomas may develop in large CMNs before puberty; melanomas in small and medium CMNs generally develop at or after puberty.
Small Congenital Melanocytic Nevi.
The incidence of malignant degeneration in small congenital nevi (<1.5 cm in diameter) is extremely low and prophylactic removal is not recommended ( Fig. 22.15 ). Melanomas arising within a small CMN occur superficially and may be detected visually at an early stage. In most cases, prophylactic excision is performed after puberty, since melanoma does not tend to occur within the early childhood years. Multiple factors must be considered in the management of small CMN (see Table 22.1 ).

Medium-Sized Congenital Melanocytic Nevi.
The risk of the occurrence of malignant melanoma in medium-sized (1.5 to 19.9 cm in diameter) CMN is the subject of controversy ( Figs. 22.16 and 22.17 ). Management is determined on a case-by-case basis. Banal-appearing medium-sized CMN may be observed for changes and should not be prophylactically removed. Individual medium-sized CMN should be monitored for change with photographs. Changing or suspicious areas within the nevus should be biopsied or the entire CMN should be surgically removed (see Table 22.1 ).


Large Congenital Melanocytic Nevi (LCMN).
LCMN may undergo malignant transformation (see Table 22.1 ; Figs. 22.18 and 22.19 ). The incidence ranges from 1.8% to 7.1%. Approximately half of the melanomas occur by 3 to 5 years of age. Many of the melanomas arise within the deeper tissues and therefore are detected at advanced stages. Melanoma occurs less often in the head and neck location and has not been detected within satellite nevi. Management of large CMN requires a multidisciplinary approach to care (see Table 22.1 ).


Dermoscopy of Congenital Melanocytic Nevi.
The most commonly observed dermoscopic features are globules (79.7%), reticular networks (70.3%), hypertrichosis (68.9%), milia-like cysts (52.7%), and perifollicular hypopigmentation (32.4%).
Neurocutaneous Melanosis (NCM).
Proliferation of melanocytes in the leptomeninges and CNS may occur in patients with CMN. Patients at greatest risk for NCM are those with large CMN >40 cm, multiple satellite nevi, and more than two medium-sized CMN. MRI with gadolinium is the best test to detect NCM (see Table 22.1 ). The median age of presentation is 2 years of age. Patients may have developmental disabilities and seizures. Death occurs in up to 34% of patients with symptomatic NCM. Patients with NCM must be followed closely by a neurologist and have serial MRI examinations (see Table 22.1 ).
Management of Congenital Melanocytic Nevi.
Risk assessment and treatment options are considered for each patient. Medical and psychosocial concerns need to be discussed. Management goals are to decrease the risk for developing melanoma by surgical removal and to produce good cosmetic results. Removal of a small CMN, with a low risk for developing melanoma, may result in a disfiguring scar and would not be acceptable. Removal of a large, thick CMN that leaves a large, dense scar may be acceptable. Timing of surgery is a consideration. The best surgical scars result from surgery performed early in life; however, it may be best to delay surgery until after age 2 when the full extent of the nevus is evident. Very large lesions may require multiple procedures. CMNs should be removed down to the fascial layer.
Prophylactic Treatment.
Prophylactic removal is considered for thick lesions in which it is difficult to detect melanoma. Dense nevi with a wrinkled (rugous) surface have the greatest risk. Growths that appear in covered areas (e.g., scalp, medial buttocks, perianal, genital areas) that are difficult to examine and follow are considered for early excision.
Speckled Lentiginous Nevus.
Speckled lentiginous nevus (nevus spilus) is a common hairless, oval or irregularly shaped brown lesion that is dotted with darker brown-to-black spots. They may appear at any age. Lesions can appear at birth or in early infancy as lightly colored café-au-lait macules. Pigmented macules and papules then develop over a period of months to years. Lesions may be very large. It has been suggested that speckled lentiginous nevus is a subtype of CMN. The brown area is usually flat, and the black dots may be slightly elevated and contain typical nevus cells ( Fig. 22.20 ). The spots range from 1 to 3 mm in diameter and may be lentigines, junctional, compound, or intradermal nevi. The background hyperpigmentation histologically has the features of a lentigo or café-au-lait macule. There is considerable variation in size, ranging from 1 to 20 cm. The anatomic position or time of onset is not related to sun exposure. Transformation into melanoma is rare. The risk of transformation may be similar to that for classic congenital nevi of similar size. Examine lesions periodically and educate the patient regarding the clinical signs of melanoma. Routine excision is not necessary. Biopsy suspicious areas. Speckled lentiginous nevus is flat and necessitates excision and closure if the patient desires removal. Lasers have been used to treat both the background hyperpigmentation and the speckles of speckled lentiginous nevi.
Becker Nevus.
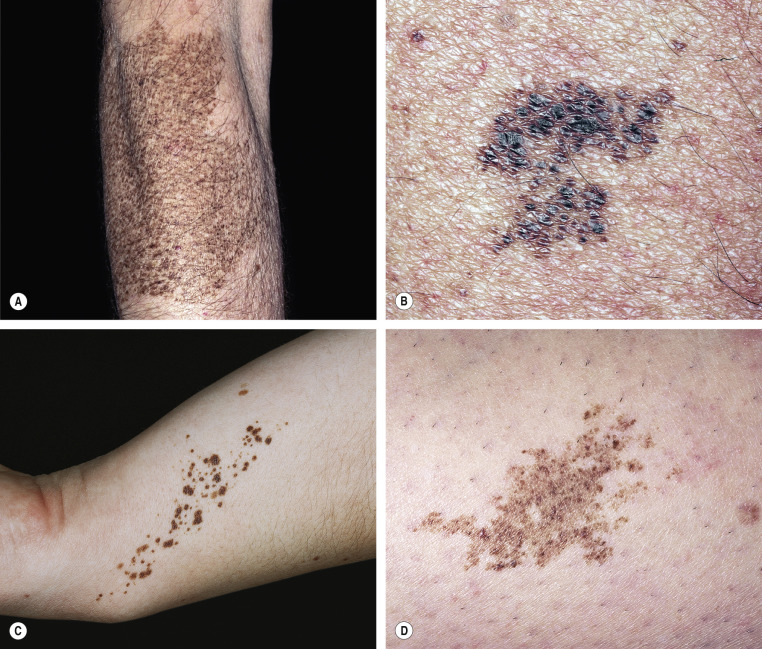
Becker nevus is not a nevocellular nevus because it lacks nevus cells. The lesion is a developmental anomaly consisting of either a brown macule ( Fig. 22.21 ) or a patch of hair ( Fig. 22.22 ), or both ( Fig. 22.23 ). Nonhairy lesions may later develop hair. The lesions appear in adolescent men on the shoulder, submammary area, and upper and lower back; they rarely appear on the lower limbs. Becker nevus varies in size and may enlarge to cover the entire upper arm or shoulder. The border is irregular and sharply demarcated.



Becker nevus syndrome is the presence of an epithelial nevus showing hyperpigmentation, increased hairiness, and hamartomatous augmentation of smooth muscle fibers as well as other developmental defects such as ipsilateral hypoplasia of the breast and skeletal anomalies, including scoliosis, spina bifida occulta, or ipsilateral hypoplasia of a limb. The Becker nevus syndrome usually occurs sporadically.
Dermoscopic features of Becker nevus include network, focal hypopigmentation, skin furrow hypopigmentation, hair follicles, perifollicular hypopigmentation, and vessels.
Becker nevus is usually too large to remove by excision. The hair may be shaved or permanently removed. Laser removal of hair and pigmentation is reported.
Halo Nevi.
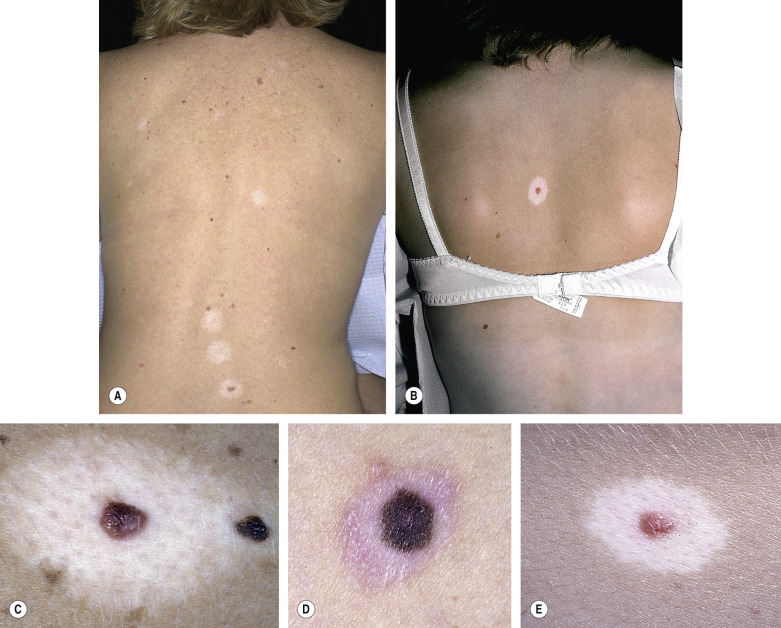
A compound or dermal nevus that develops a white border is called a halo nevus. The incidence in the population is estimated to be 1%. Halo nevi are found most commonly in children. The average age of onset is 15 years. Halo nevi typically persist for a decade or longer. The depigmented halo is symmetric and round or oval with a sharply demarcated border ( Fig. 22.24 ). There are no melanocytes in the halo area. Halo nevi have the dermoscopic features of benign MNs, with globular and/or homogeneous patterns that are typically observed in children and young adults. Halo nevi structural patterns remain unchanged over time. Patients with Turner syndrome (short stature, gonadal dysgenesis, webbed neck, cubitus valgus, and lymphedema at birth) have a halo nevus prevalence of 18%.
Histologic Characteristics.
T lymphocytes at the site of depigmentation suggest that these cells participate in the halo phenomenon. Most halo nevi are located on the trunk; they never occur on palms and soles. They may occur as an isolated phenomenon, or several nevi may spontaneously develop halos. Halos may repigment with time, or the nevus may disappear. Repigmentation often takes place over months or years; however, it does not always occur. Repigmentation does not follow removal of the nevus. The incidence of vitiligo may be increased in patients with halo nevi. A halo may rarely develop around malignant melanoma, but in such instances it is usually not symmetric.
Removal of a halo nevus is unnecessary unless the nevus has atypical features. Parental concern over this impressive change is often the reason for a conservative excision. In such cases, the mole part of a halo nevus may be removed by shave, excision, or laser.
Spitz Nevus.
Spitz nevus (Spitz tumor, spindle and epithelioid cell nevus) is most common in children but does appear in adults. The most frequent sites include the head and neck regions (37%) and lower extremities (28%). They are hairless, red or reddish-brown, dome-shaped papules or nodules with a smooth ( Fig. 22.25 ) or warty surface; they vary in size from 0.3 to 1.5 cm. The color is caused by increased vascularity, and bleeding sometimes follows trauma. Spitz nevi are usually solitary but may be multiple. They appear suddenly and, contrary to slowly evolving common moles, patients can sometimes date their onset. Banal-appearing, stable Spitz nevi may be monitored clinically. Atypical Spitz nevi (growing, bleeding, change in color, unusual dermoscopic findings) should be completely removed for microscopic examination. Histologic differentiation from melanoma is sometimes difficult. Histopathologic features that suggest more aggressiveness relate to mitotic activity, mitoses near the base, and inflammation.


Dermoscopy of Spitz nevus shows: (1) a starburst pattern, characterized by a prominent, black to blue diffuse pigmentation and pseudopods regularly distributed at the periphery in a radiate pattern; and (2) a globular pattern, typified by a discrete, brown to gray-blue pigmentation and a peripheral rim of large brown globules, often extending throughout the entire lesion.
Blue Nevus.
The blue nevus is a slightly elevated, round, regular nevus, usually less than 0.5 cm, and contains large amounts of pigment located in the dermis ( Figs. 22.26 to 22.28 ![]() ). The brown pigment absorbs the longer wavelengths of light and scatters blue light (Tyndall effect). The blue nevus appears in childhood and is most common on the extremities and dorsum of the hands. A rare variant, the cellular blue nevus, is larger (usually greater than 1 cm) and nodular and is frequently located on the buttocks.
). The brown pigment absorbs the longer wavelengths of light and scatters blue light (Tyndall effect). The blue nevus appears in childhood and is most common on the extremities and dorsum of the hands. A rare variant, the cellular blue nevus, is larger (usually greater than 1 cm) and nodular and is frequently located on the buttocks.



Melanomas are reported as arising in association with a common or cellular blue nevus and arising de novo and resembling cellular blue nevi. Blue nevi may be removed for cosmetic purposes.
Dermal Melanocytosis.
Deep blue-black pigmentation due to melanocytes in the dermis may be seen in newborns with darker skin types. It is an isolated cutaneous finding and usually resolves by the toddler years ( Fig. 22.29 ). Dermal melanocytosis may be confused with child abuse and rarely is associated with inborn errors of metabolism.

Labial Melanotic Macule.
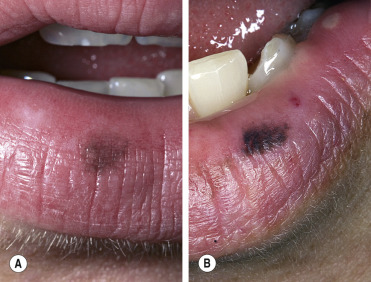
Brown macules on the lower lip are relatively common, especially in young adult women ( Fig. 22.30 ). Histologically, they resemble freckles and not lentigo, but unlike freckles, they do not darken with sun exposure. They are benign. Cryotherapy or laser surgery is used for patients who request treatment.
Atypical Nevi
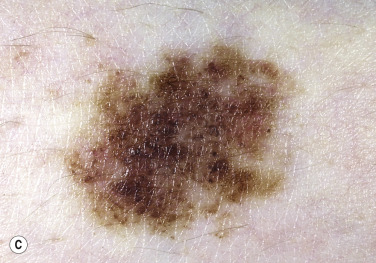
Atypical nevi, also referred to as dysplastic nevi or Clark nevi, may be inherited in a familial pattern or occur sporadically. They are usually larger than 5 mm in diameter and either are flat or are smooth with a raised center (“fried-egg lesion”) ( Table 22.2 ![]() ). They are darkly or irregularly pigmented with shades of brown and pink and usually have irregular or indistinct borders. Atypical nevi are common, with a prevalence rate of about 5%. Atypical nevi differ from commonly acquired nevi by (1) beginning to appear near puberty instead of in childhood and (2) continuing to develop past the fourth decade. Atypical nevi are benign and are a “marker” for patients at an increased risk for development of melanoma, especially in individuals with many nevi and/or a family history of melanoma. Atypical nevi, like banal-appearing nevi, may serve as a precursor to melanoma.
). They are darkly or irregularly pigmented with shades of brown and pink and usually have irregular or indistinct borders. Atypical nevi are common, with a prevalence rate of about 5%. Atypical nevi differ from commonly acquired nevi by (1) beginning to appear near puberty instead of in childhood and (2) continuing to develop past the fourth decade. Atypical nevi are benign and are a “marker” for patients at an increased risk for development of melanoma, especially in individuals with many nevi and/or a family history of melanoma. Atypical nevi, like banal-appearing nevi, may serve as a precursor to melanoma.
| Characteristics | Atypical Moles | Common Nevi |
|---|---|---|
| Distribution | Back most common, upper and lower limbs, sun-protected areas, female breasts, scalp, buttocks, groin | Usually sun-exposed areas; most above the waist |
| Number | Less than 10 to greater than 100 | 10 to 40 |
| Age at onset | Appear as normal nevi at age 2 to 6 years; increase in number and size at puberty; new nevi appear throughout life | Absent at birth; appear at age 2 to 6; grow vertically in uniform manner throughout life; several may appear at puberty |
| Size | Usually greater than 5 mm and commonly greater than 10 mm | Usually less than 6 mm |
| Shape and contour | Irregular border; flat (macular) areas; margin fades into surrounding skin; always has a macular component | Round, symmetric, uniformly macular or papular smooth border |
| Color | Variable within a single lesion; brown, black, red, pink | Uniform tan, brown, black; darken during pregnancy or at adolescence; become lighter with age |
| Histologic characteristics | Persistent lentiginous melanocytic hyperplasia; melanocytic nuclear atypia; * lamellar fibroplasias; concentric eosinophilic fibroplasias; sparse, patchy lymphocytic infiltration | Nevus cells at dermoepidermal junction and/or in dermis |
Familial Atypical Multiple Mole Melanoma Syndrome (FAMMM).
The FAMMM syndrome is an autosomal-dominantly inherited condition seen in patients with the following criteria:
- 1.
The occurrence of malignant melanoma in one or more first- or second-degree relatives
- 2.
The presence of a large number of MNs, often more than 50, some of which are atypical and often variable in size.
- 3.
The development of MNs that demonstrate certain histologic features.
Atypical Melanocytic Nevi Association With Melanoma.
Individuals with atypical nevi have up to a 20-fold increased risk of developing malignant melanoma, compared to those without atypical nevi. The risk for melanoma increases as the number of atypical nevi increases. Seventy percent of melanoma arises de novo and is not associated with a precursor melanocytic nevus. For this reason, prophylactic removal of atypical nevi is not recommended. Individuals with multiple atypical nevi and a family history of melanoma have a 15% risk of developing melanoma. Individuals who have multiple atypical nevi and a personal history of melanoma have a 10% risk of developing a second melanoma. The lifetime risk of melanoma approaches 100% for those individuals with multiple atypical nevi and two or more first-degree relatives with melanoma.
Classification of Atypical Melanocytic Nevi
Clinical Classification
The clinical diagnosis of atypical melanocytic nevi is established when at least three of the following characteristics are present:
- •
Diameter greater than 5 mm
- •
Ill-defined borders
- •
Irregular margin
- •
Varying shades in the lesion
- •
Presence of papular and macular components.
Clinical Features of Atypical Moles
Morphology.
These unusual nevi differ in a number of important ways from typical acquired pigmented nevi or moles (see Table 22.2 ![]() ). AMs are larger than common moles. They have a mixture of colors, including tan, brown, pink, and black. The border is irregular and indistinct and often fades into the surrounding skin. The surface is complex and variable, with both macular and papular components ( Fig. 22.31 ). A characteristic presentation is a pigmented papule surrounded by a macular collar of pigmentation (“fried-egg lesion”) ( Fig. 22.32 ). In one study, the total number of nevi and macular components were the only useful features to predict histologic melanocytic dysplasia. However, “fried-egg lesions” often do not display histologic melanocytic dysplasia. In contrast, the absence of a macular component in MNs in a person with fewer than 13 total body nevi accurately predicts the absence of melanocytic dysplasia on histologic examination.
). AMs are larger than common moles. They have a mixture of colors, including tan, brown, pink, and black. The border is irregular and indistinct and often fades into the surrounding skin. The surface is complex and variable, with both macular and papular components ( Fig. 22.31 ). A characteristic presentation is a pigmented papule surrounded by a macular collar of pigmentation (“fried-egg lesion”) ( Fig. 22.32 ). In one study, the total number of nevi and macular components were the only useful features to predict histologic melanocytic dysplasia. However, “fried-egg lesions” often do not display histologic melanocytic dysplasia. In contrast, the absence of a macular component in MNs in a person with fewer than 13 total body nevi accurately predicts the absence of melanocytic dysplasia on histologic examination.





Surface Characteristics.
The surface characteristics of atypical nevi are distinctive and can be appreciated with a hand lens and dermoscope.
Development and Distribution.
Atypical moles are not present at birth, but begin to appear in the mid-childhood years as typical common moles. The appearance changes at puberty, and newer lesions continue to appear well after the age of 40. Common moles occur most often on sun-exposed areas. AMs occur in those locations and at unusual sites such as the scalp, buttocks, and breast. The predilection sites for melanoma in familial AM patients of both genders correspond with the distribution of nevi; in males, nevi and melanoma counts are higher on the back; in females, both the back and the lower extremities are affected. These findings strongly suggest an association between nevus distribution and melanoma occurrence and site in familial AMs.
Histologic Characteristics.
The National Institutes of Health (NIH) Consensus Conference listed the histologic criteria as follows: architectural disorder with asymmetry, subepidermal (concentric eosinophilic and/or lamellar) fibroplasia, and lentiginous melanocytic hyperplasia with spindle or epithelioid melanocytes aggregating in nests of variable size and forming bridges between adjacent rete ridges. Melanocytic atypia may be present to a variable degree. In addition, there may be dermal infiltration with lymphocytes, as well as the “shoulder” phenomenon (intraepidermal melanocytes extending singly or in nests beyond the main dermal component).
Management.
Management recommendations are given in Box 22.1 .
- •
Frequency of total body examinations:
- •
Without personal or family history of melanoma: up to a few AMN – yearly; many – every 6 months
- •
With personal or family history of melanoma: every 3 to 6 months
- •
FAMMM kindreds first full body skin examination at age 10
- •
- •
Use blow-dryer for scalp examination
- •
Consider total cutaneous photographs as baseline
- •
Excise lesions suspected to be melanoma
- •
Educate patient on self-examination of skin
- •
Recommend sun avoidance and/or protection
- •
Suggest screening of blood relatives for AM and MM
- •
Suggest regular ophthalmologic examinations for ocular nevi and ocular melanoma
AM, atypical mole; AMN, atypical melanocytic nevi; FAMMM, familial atypical multiple mole melanoma syndrome; MM, malignant melanoma.
Surgical Excision and Re-Excision.
Consensus guidelines were developed for surgical and reexcision of atypical nevi ( Box 22.2 ).
- •
Examine the total cutaneous surface utilizing dermoscopy.
- •
Biopsy should attempt to obtain clear margins (1 to 3 mm)
- •
The histology of a partial biopsy may not be representative of the entire lesion when there is residual clinical pigmentation.
- •
Banal-appearing nevi should be monitored with photography
- •
Degree of clinical concern and histologic dysplasia are equally important when deciding to re-excise a DN. A clinically worrisome DN, with minimal histologic dysplasia and a DN with severe dysplasia should be re-excised with 2–5 mm margins, if the margins of the biopsy are involved.
- •
In general, DN with mild and moderate histologic dysplasia and negative biopsy margins do not require re-excision.
- •
DN with mild histologic dysplasia and no residual pigmentation may be followed without re-excision, even when biopsy margins are positive.
- •
All biopsy sites exhibiting growth or re-pigmentation should be re-biopsied.
Malignant Melanoma
Malignant melanoma is a malignancy of melanocytes that occurs in the skin, eyes, ears, gastrointestinal tract, leptomeninges, and oral and genital mucous membranes. One of the most dangerous tumors, melanoma has the ability to metastasize to any organ, including the brain and heart.
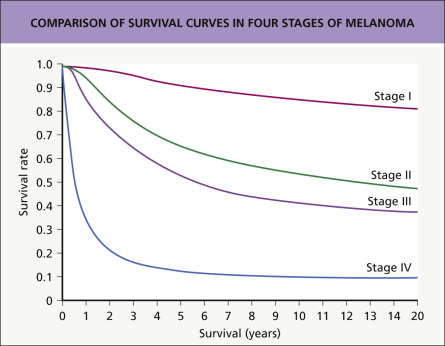
Epidemiology.
In the United States, melanoma is the fifth most common cancer after prostate, lung, colon, and bladder in men and breast, colon, uterine, and thyroid in women. In 2018, the National Cancer Institute estimated 91,270 new cases and 9320 deaths in the United States. The incidence of melanoma has continued to increase since 1992, but the number of deaths has not substantially decreased. Fig. 22.33 ![]() summarizes the current survival curves. The risk of developing melanoma is 20 times higher for whites (1 in 38) than Hispanics (1 in 172) and African Americans (1 in 1000). The risk for melanoma increases with age (average age at diagnosis 63), but melanoma is one of the most common cancers in young adults (age 20 to 39), especially women. The arms and legs are common sites in women and the back and shoulders in men. In nonwhites, the lower extremities and acral sites are most commonly affected.
summarizes the current survival curves. The risk of developing melanoma is 20 times higher for whites (1 in 38) than Hispanics (1 in 172) and African Americans (1 in 1000). The risk for melanoma increases with age (average age at diagnosis 63), but melanoma is one of the most common cancers in young adults (age 20 to 39), especially women. The arms and legs are common sites in women and the back and shoulders in men. In nonwhites, the lower extremities and acral sites are most commonly affected.
Risk for Melanoma.
The risk factors for melanoma are listed in Table 22.3 .
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


