Abstract
The neck is an important structure for dermatologic surgery. Surgeons should be familiar with the anatomy of the neck including direction of the relaxed skin tension lines, location of the anterior and posterior triangles, and Erb’s point. Reconstructive options include linear closure, transposition and advancement flaps, and granulation. The skin of the neck can be used as a reservoir of tissue for full-thickness skin grafts or flap repairs to adjacent areas of the face.
Keywords
neck, Erb’s point, anatomy, linear closure, transposition flap, advancement flap
Introduction and Perioperative Consideration
The neck is the portion of the body that links the trunk to the head. As the neck is prone to sun exposure, it is a common location for dermatologic surgeons to remove skin cancers. The neck contains many vital structures, and one should therefore be familiar with the neck anatomy and potential reconstructive options.
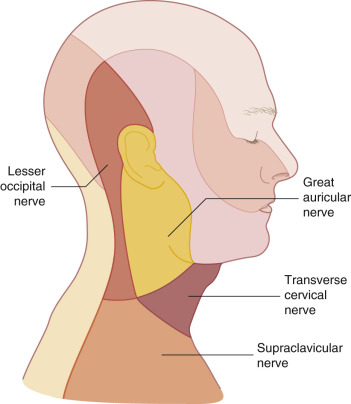
The mobility and thickness of neck skin are dependent on location as well as the age of the patient. The posterior neck skin is usually thicker and less mobile than the skin on the anterior or lateral portions of the neck. With increasing age, the skin of the neck also becomes more pliable, which allows the neck to serve as a reservoir for tissue recruitment. The relaxed skin tension lines on the central anterior and posterior neck lie horizontally and transition to an oblique orientation on the lateral portions of the neck ( Fig. 17.1 ). Placing scars within the relaxed skin tension lines whenever possible will lead to better cosmetic results.

Positioning a patient appropriately prior to surgery can have a great impact on the ease of performing the surgical procedure as well as overall cosmesis. When performing a surgery on the anterior or posterior neck, the patient should be positioned supine or prone respectively. When the surgical site is located on the lateral neck, the patient should be marked for closure while the patient is holding the neck in a neutral position. If the neck is turned far laterally for suturing, this may distort the relaxed skin tension lines and result in misplacement of scars and standing cones.
Introduction and Perioperative Consideration
The neck is the portion of the body that links the trunk to the head. As the neck is prone to sun exposure, it is a common location for dermatologic surgeons to remove skin cancers. The neck contains many vital structures, and one should therefore be familiar with the neck anatomy and potential reconstructive options.
The mobility and thickness of neck skin are dependent on location as well as the age of the patient. The posterior neck skin is usually thicker and less mobile than the skin on the anterior or lateral portions of the neck. With increasing age, the skin of the neck also becomes more pliable, which allows the neck to serve as a reservoir for tissue recruitment. The relaxed skin tension lines on the central anterior and posterior neck lie horizontally and transition to an oblique orientation on the lateral portions of the neck ( Fig. 17.1 ). Placing scars within the relaxed skin tension lines whenever possible will lead to better cosmetic results.

Positioning a patient appropriately prior to surgery can have a great impact on the ease of performing the surgical procedure as well as overall cosmesis. When performing a surgery on the anterior or posterior neck, the patient should be positioned supine or prone respectively. When the surgical site is located on the lateral neck, the patient should be marked for closure while the patient is holding the neck in a neutral position. If the neck is turned far laterally for suturing, this may distort the relaxed skin tension lines and result in misplacement of scars and standing cones.
Anatomy of the Neck
Cutaneous Anatomy
The anterior aspect of the neck is bound superiorly by the mandible of the jaw and inferiorly by the clavicle. The posterior aspect of the neck is bound superiorly by the hairline or base of the skull and inferiorly by the upper portion of the scapula.
Triangles
The sternocleidomastoid muscle divides the neck into the anterior and posterior triangles ( Fig. 17.2 ). The anterior triangle is defined by the anterior border of the sternocleidomastoid, the inferior margin of the mandible, and the midline of the neck. This triangle contains the platysma muscle, which constitutes a major component of the superficial musculoaponeurotic system (SMAS) layer, and is continuous with the SMAS of the face. This muscle overlays the investing cervical fascia and is approximately 0.6 mm thick, but becomes slightly thicker in the submental area. The platysma is considered a muscle of facial expression, as contraction of the platysma muscle pulls down the lower lip and results in grimacing.
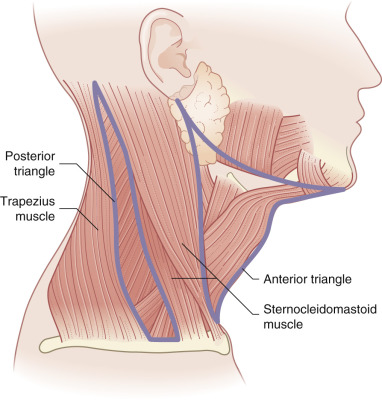
The posterior triangle is defined by the posterior border of the sternocleidomastoid muscle, the anterior border of the trapezius muscle, and the superior aspect of the clavicle. This triangle contains the spinal accessory nerve (cranial nerve XI) at its most superficial point, known as Erb’s point. Erb’s point describes the area where the spinal accessory nerve emerges from approximately one-third down the posterior border of the sternocleidomastoid muscle and courses through the posterior triangle inferiorly and diagonally along the levator scapulae muscle to penetrate a point two-thirds down the anterior edge of the trapezius muscle before it runs deep under the muscle.
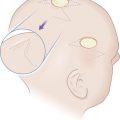
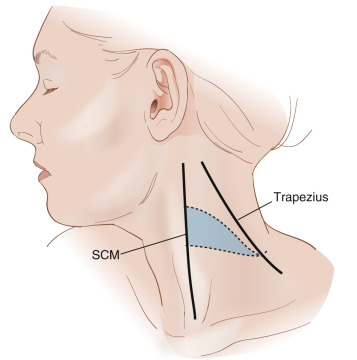
Erb’s point can be easily located by finding the half-way point between the mastoid process and the angle of the jaw and drawing a perpendicular line 6.0 cm vertically down the neck to the point where it intersects the posterior aspect of the sternocleidomastoid muscle ( Fig. 17.3 ). Another way to identify Erb’s point is by drawing a horizontal line from the thyroid notch to the posterior triangle on the neck. The area approximately 2 cm above and below where this line crosses the posterior border of the sternocleidomastoid is the where the nerve traverses the posterior triangle and is most prone to injury.
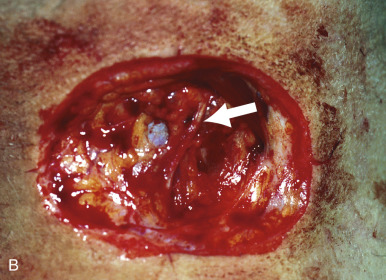
This point is particularly important for dermatologic surgeons given the superficial nature of the spinal accessory nerve lying just below the skin and subcutaneous tissue. Fig. 17.4A shows a basal cell carcinoma located over the posterior triangle of the neck, and the spinal accessory nerve is visible after removal of the tumor (see Fig. 17.4B ). Damage to the spinal accessory nerve can cause significant morbidity including shoulder drop and the inability to abduct the shoulder past 80 degrees. Paresthesias and pain may also accompany damage to this nerve. Given the superficial nature of this nerve, great care should be taken when operating in this area.

Blood Supply
Arteries
The common carotid artery courses through the anterior triangle, and divides within the triangle into the external and internal carotid arteries. After it leaves the neck, the external carotid artery branches extensively. Branches of note are the facial and superficial temporal arteries that provide blood supply to the face and anterior scalp.
Veins
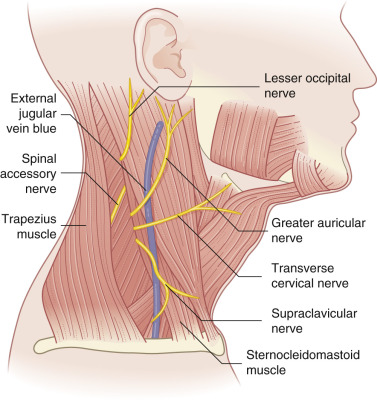
The external jugular vein ( Fig. 17.5 ) is a major drainage point for the scalp and face. It begins near or in the parotid gland, travels underneath the platysma, and crosses above the sternocleidomastoid muscle before it empties into the internal jugular or subclavian vein. Additionally, the external jugular vein has tributaries that connect with the internal jugular vein and the anterior jugular vein that is located anterior in the neck.
Nerves
Besides the major motor nerve, the spinal accessory nerve, which innervates the trapezius, a few important sensory nerves from the superficial cervical plexus also emerge near Erb’s point ( Fig. 17.5 ). The greater auricular nerve exits the posterior surface of the sternocleidomastoid and runs toward the earlobe and mastoid process. Damage to this nerve produces numbness to the earlobe. This nerve is one of the most frequently injured nerves during face and neck lift surgery, and the resulting sensory deficit can be distressing for patients. The transverse cervical nerve and supraclavicular nerve similarly can be damaged in this area and result in a loss of sensation to the anterior and lateral neck ( Fig. 17.6 ).