Acknowledgment
All photographs, illustrations, descriptions, and text contained in this chapter are property of the Marten Clinic of Plastic Surgery, San Francisco, CA, and are used with permission.
 For video accompanying this chapter see ExpertConsult.com . See inside cover for access details.
For video accompanying this chapter see ExpertConsult.com . See inside cover for access details.
Introduction
Why Perform a Neck Lift?
Why perform a neck lift? Why not just lift the cheeks and jawline or perform other procedures that rejuvenate the eyes or upper face? The simple answer is that a well-contoured neck is an artistic imperative to an attractive and appealing appearance. A good neckline conveys a sense of youth, health, fitness, and vitality, and lends an appearance of decisiveness, sensuality, and beauty ( Fig. 67.1 ). Neck improvement is of high priority to almost every patient seeking facial rejuvenation, and the results of our “facelift” procedures are largely judged by the outcome we achieve in the neck. If the neck is not sufficiently improved our patients will feel we have failed them.
How Should a Neck Lift be Performed?
It is unlikely there will ever be a consensus on how a neck lift should be performed and it is a fact that no one procedure will be best for all patients. The technique used cannot be arbitrary, will depend on deformities present, and will necessarily vary from patient to patient. Success or failure in treating the neck, like the nose, breast, and body, lies in the diagnosis of problems and the application of a logical surgical plan, and any surgeon capable of identifying the anatomic basis of patient problems and forming a sound plan for their correction can achieve excellent outcomes.
So how should one perform a neck lift? Perhaps it is easiest to start by stating what not to do. Despite the fact that it is the traditional approach and remains a common practice, it is not enough to perform submental liposuction and tighten the skin in most patients. This approach ignores a number of anatomical problems present in many patients seeking neck improvement, including platysmal laxity, platysmal bands, excess subplatysmal fat, large submandibular glands, digastric muscle hypertrophy, and developmental factors such as the size and shape of the bony jaw and chin. Removing subcutaneous fat and tightening skin over these problems does not correct them, and the presence or absence of each must be looked for in order to create and apply an appropriate surgical plan ( Fig. 67.2 ).
Strategies for Neck Lift
Patients seeking neck improvement have a range of options available to them depending on the problems present, the degree of improvement they seek, and the time, trouble, and expense they are willing to undergo to obtain the improvement they desire. And while it is incumbent upon us to discuss these options and the advantages and disadvantages of each, patients are also seeking our guidance as to what is possible, what is practical, and what is really best. It is not enough to steer patients to procedures we are comfortable with. We are professionally bound and ethically obliged to refer patients for the care they need and desire if we are not able to provide it ourselves.
Submental Liposuction
Submental liposuction (and arguably “noninvasive” treatments including cryolipolysis, deoxycholic acid injections, and radiofrequency and ultrasound “skin shrinking” treatments) is the simplest and likely the most commonly performed procedure to improve neck contour in the range of options available to patients. It does not constitute a true neck lift, however, and only occasionally produces optimal outcomes. Patients and surgeons are predictably drawn into a sense of denial of this, however, by the fact that submental liposuction will occasionally produce worthwhile improvement in some cases, and it is these atypical outcomes that are predictably displayed in offices, placed in advertisements, shown on TV and websites, published in the beauty press, and even included in presentations at plastic surgery symposia. Adding to the deception is the fact that these photographs have usually been taken in the early postoperative period when swelling is still present that obscures irregularities and underlying but untreated deep layer problems.
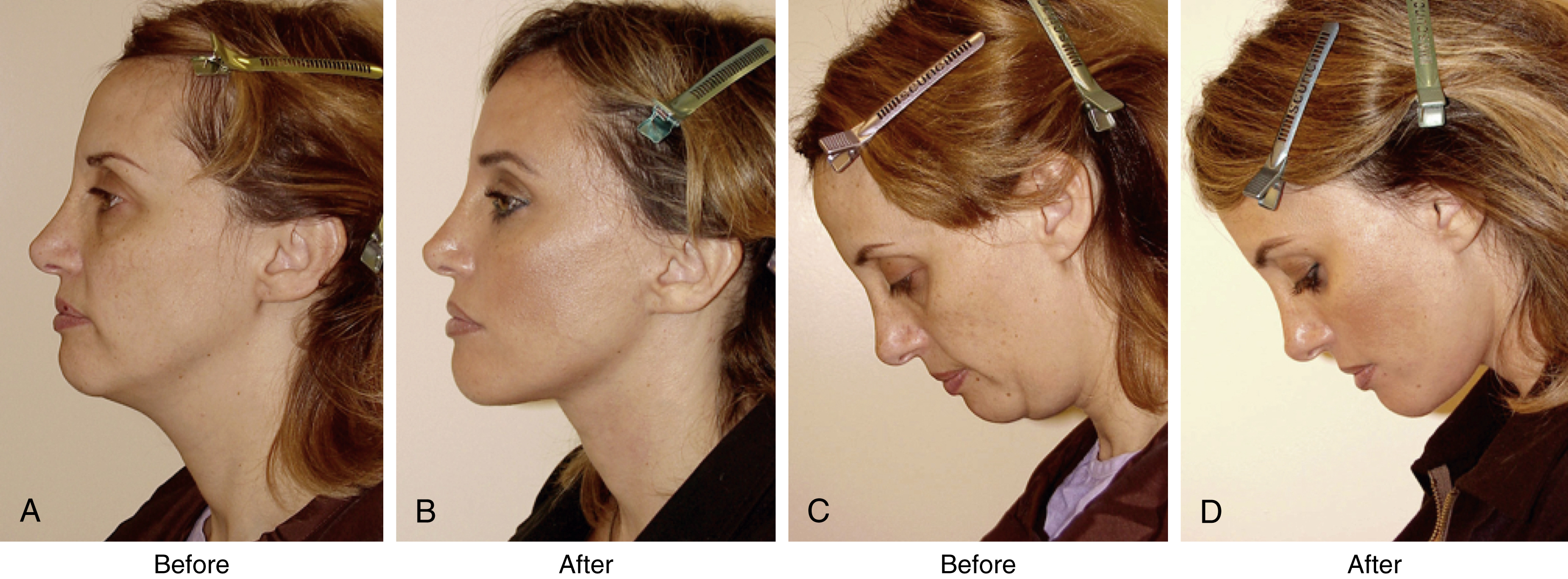
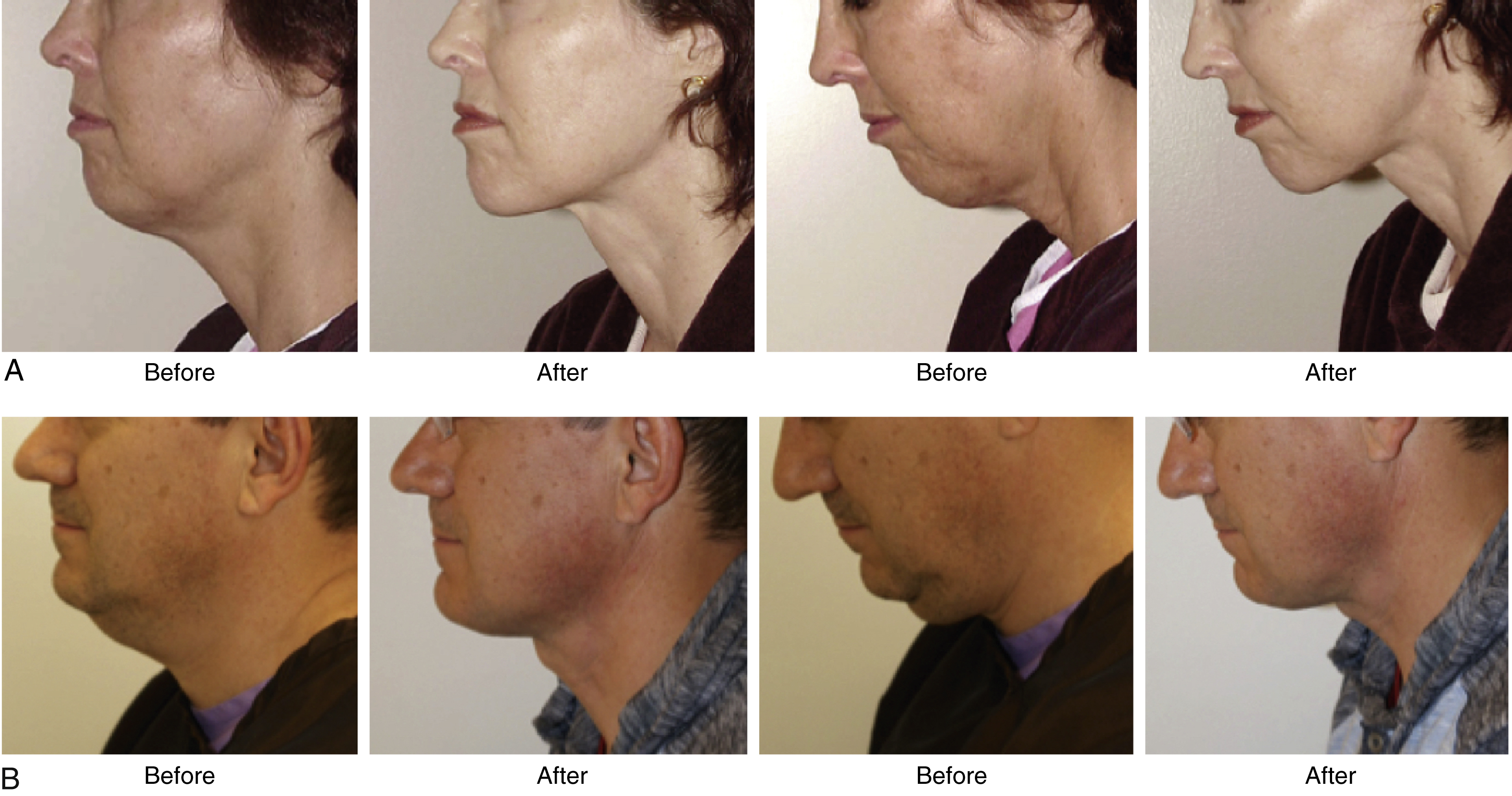
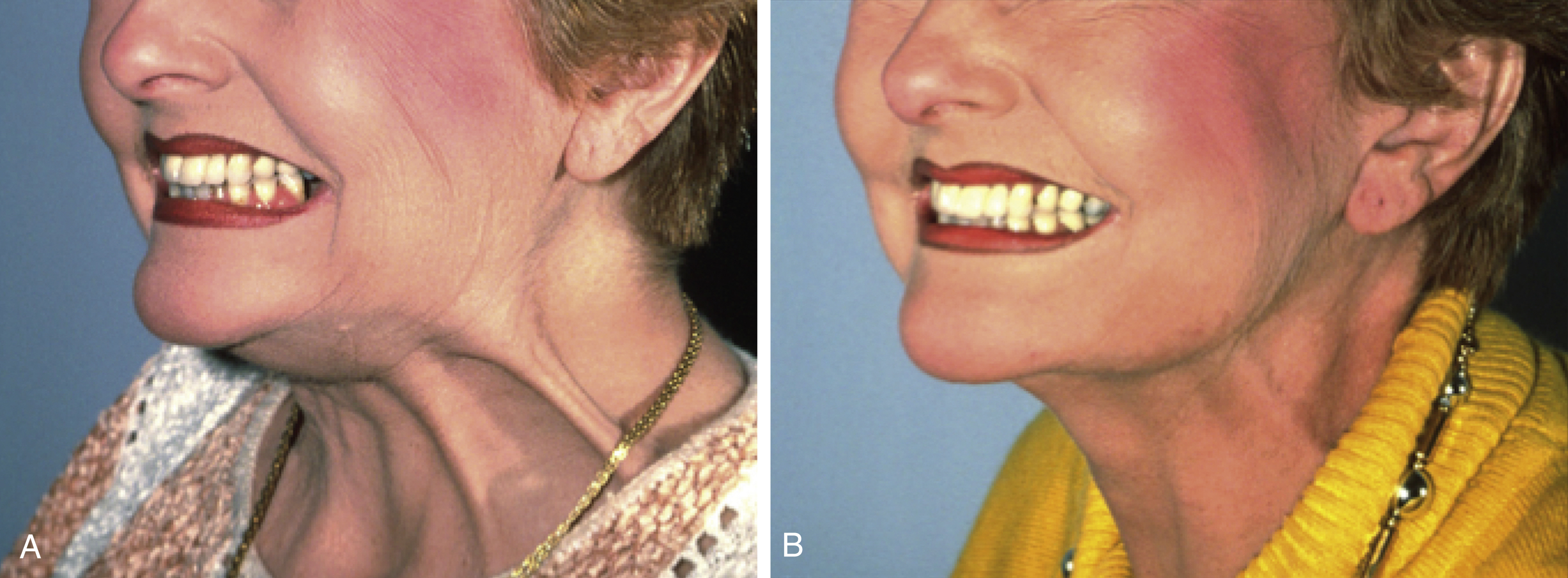
In reality, submental liposuction (and noninvasive procedures that target subcutaneous neck fat) is an incomplete solution to neck problems for most patients. As a standalone treatment it suffers the significant drawback that it falsely assumes poor neck contour to be solely the result of the accumulation of subcutaneous fat only, and it is conceptually flawed in that it does not address platysma laxity and other deep layer problems which together typically play a much larger and more important role in the aging neck and neck contour deformities. As a result, most patients undergoing this procedure arguably achieve marginal improvement, but not comprehensive correction of their neck problems, and ultimately relying on this technique as the only method to obtain improved neck contour will seldom be consistently successful ( Fig. 67.3 ).
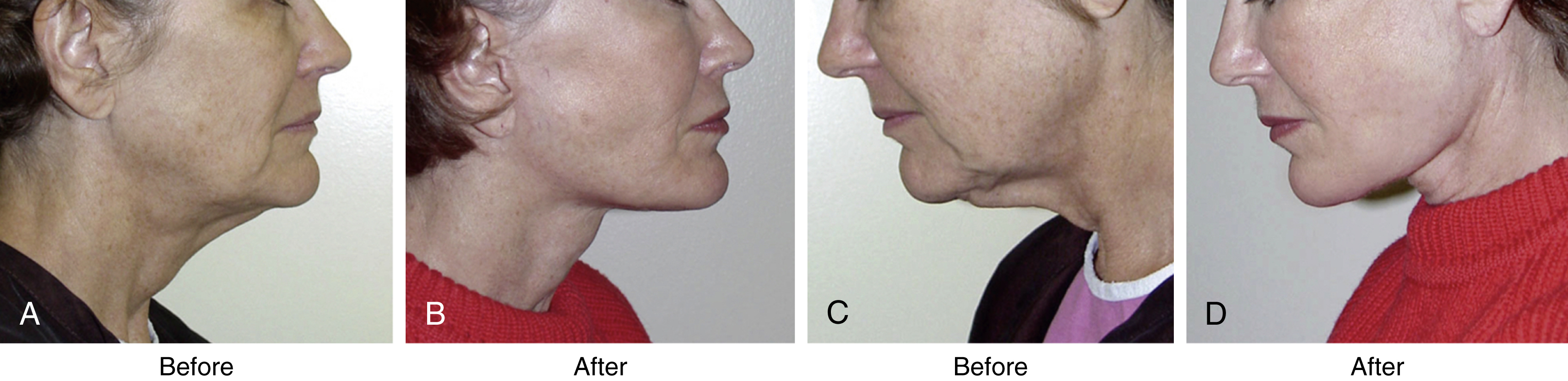
Submental liposuction is also a frequent cause of many vexing patient problems and complications as it often leads to unintended but inappropriate removal of subcutaneous fat essential to a natural and youthful appearance, and this can, in turn, expose underlying problems of deep layer origin. Misapplied and overused, or when aggressive “ultrasonic” and “laser” techniques and other “power tools” are over-zealously employed, submental liposuction can all too commonly result in extreme overresection of precious subcutaneous fat and very unnatural and objectionable appearances. These problems are typically not evident in the operating room or in the early postoperative period when cervicosubmental tissues are swollen, but appear later, and once present, are very difficult to correct ( Fig. 67.4 ).

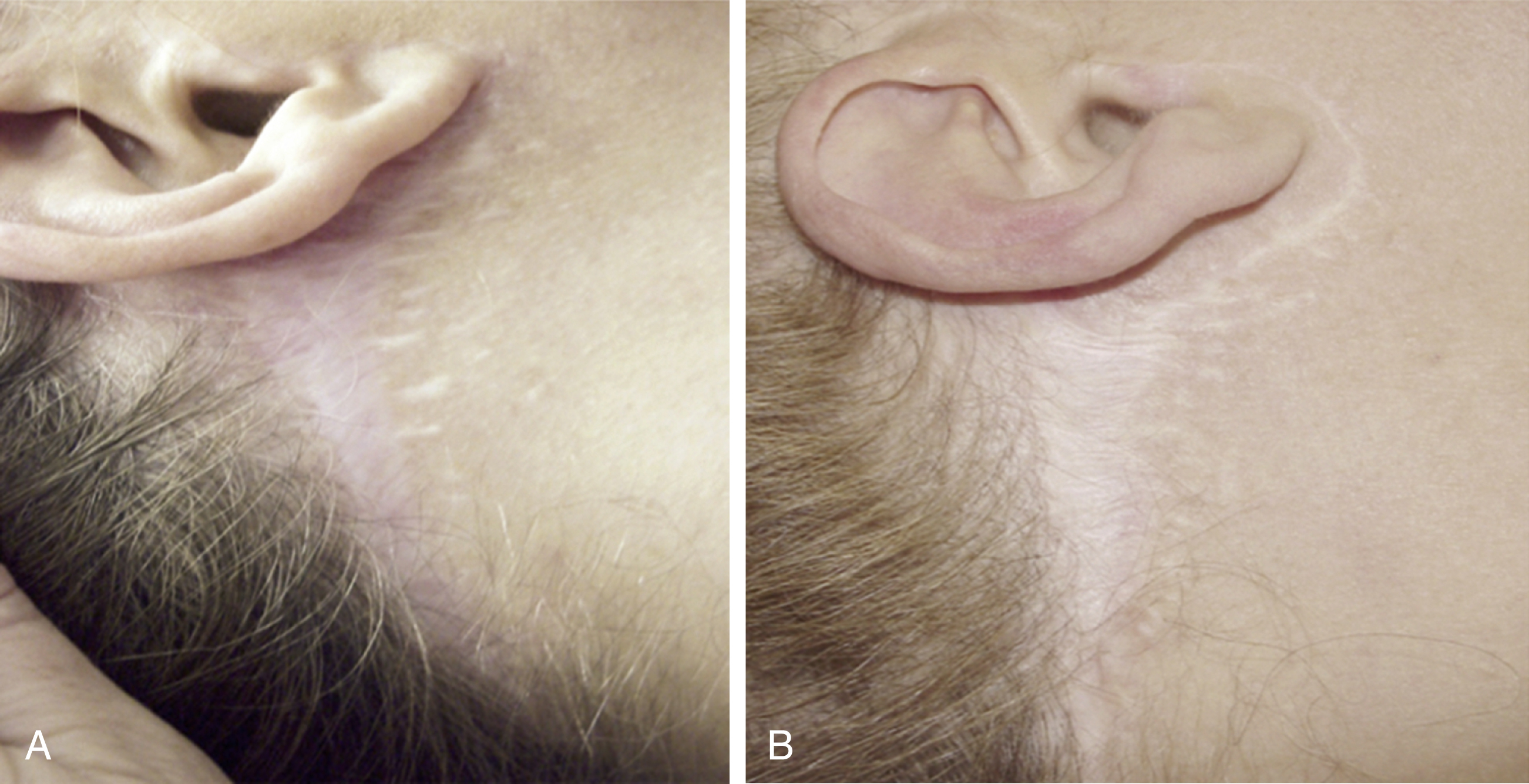
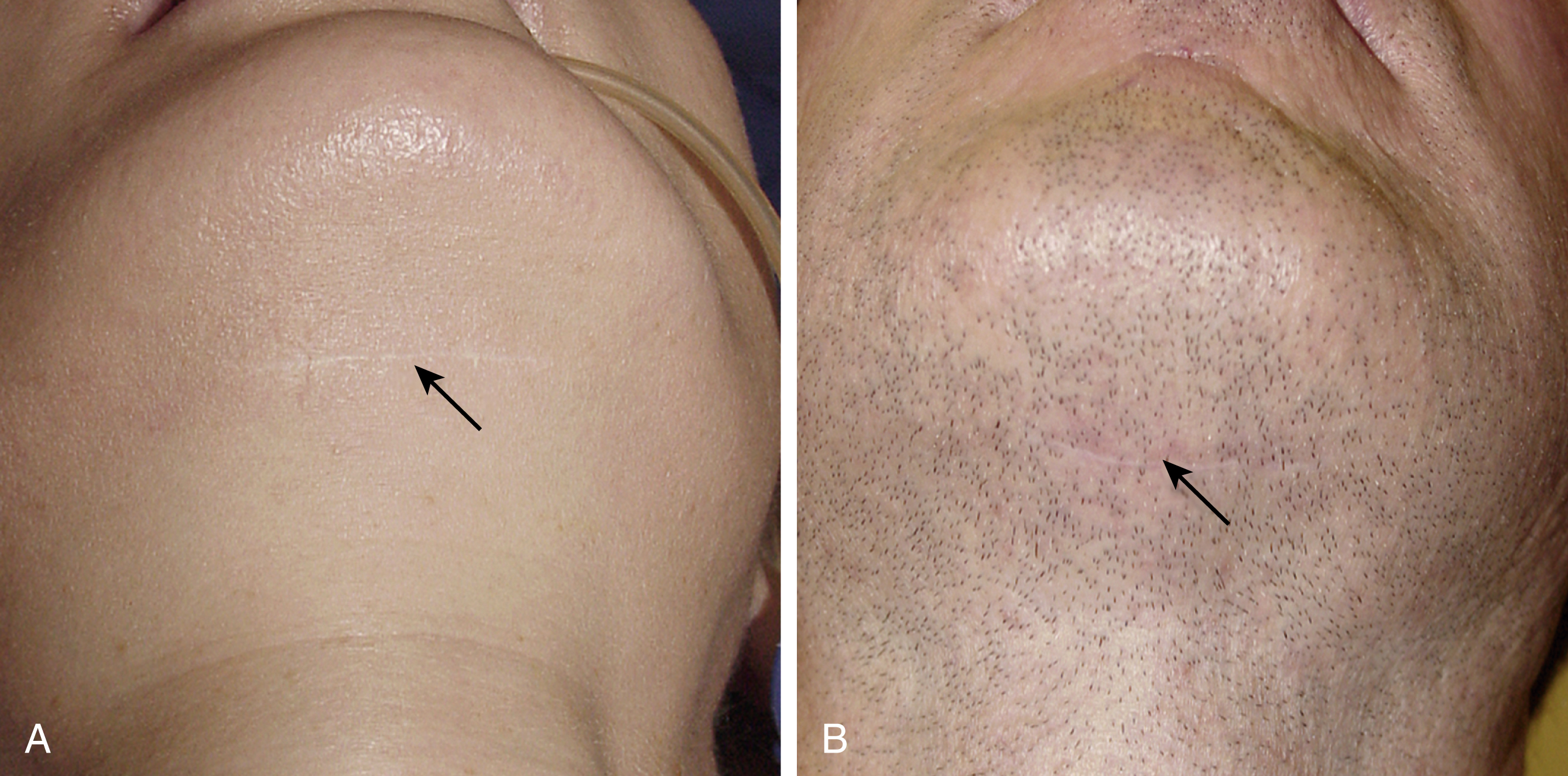
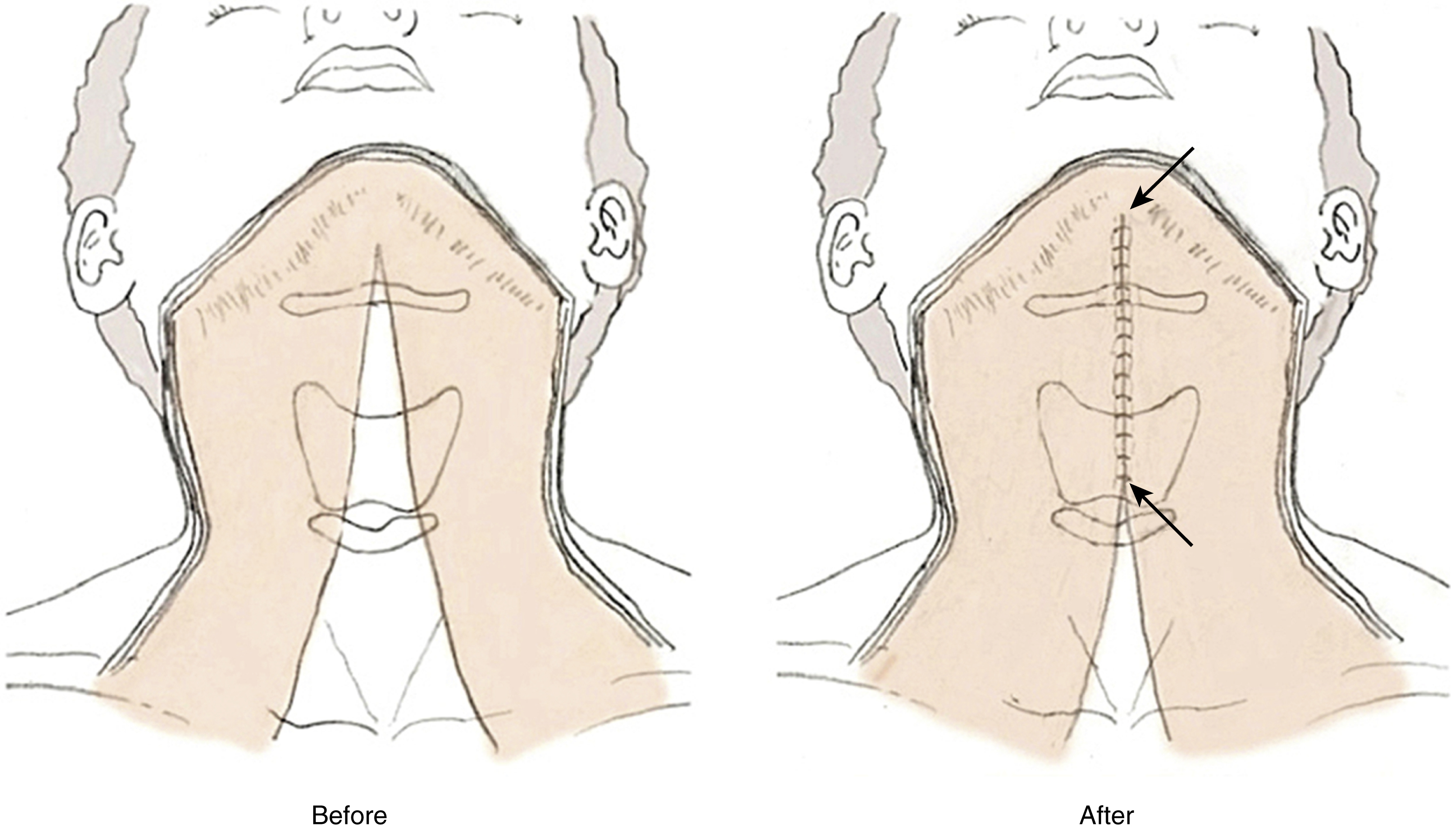
Liposuction, in combination with ill-conceived overtightening of neck skin, can add the additional objectionable problems of hairline displacement and wide postauricular scars, and compound the overall deformity ( Fig. 67.5 ).
Despite its many drawbacks and propensity to precipitate troublesome and difficult-to-treat problems, the conceptual and comparative technical simplicity of submental liposuction is particularly appealing to inexperienced surgeons and nonsurgeons performing esthetic surgery procedures. Indeed, these characteristics of the technique almost guarantee that, effective or not, it will continue to be overused and inappropriately recommended to patients who are not good candidates for the procedure for the foreseeable future.
“Short-Scar” Neck Lift (Neck Lift with Submental Incision Only)
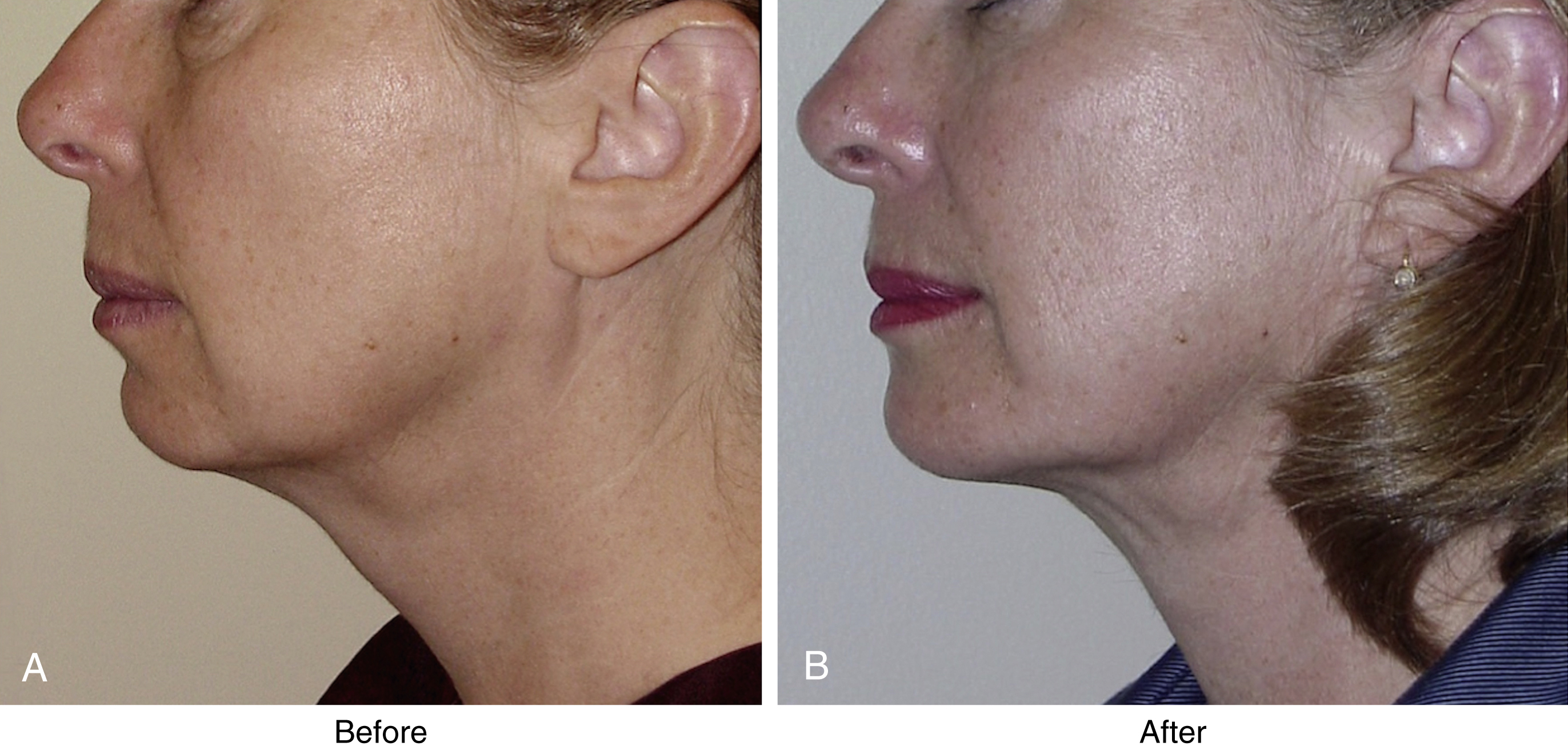
Although submental liposuction alone will rarely produce optimal neck improvement, a neck lift performed through a submental incision without any removal of skin can create attractive cervical contour in many patients ( Fig. 67.6 ).
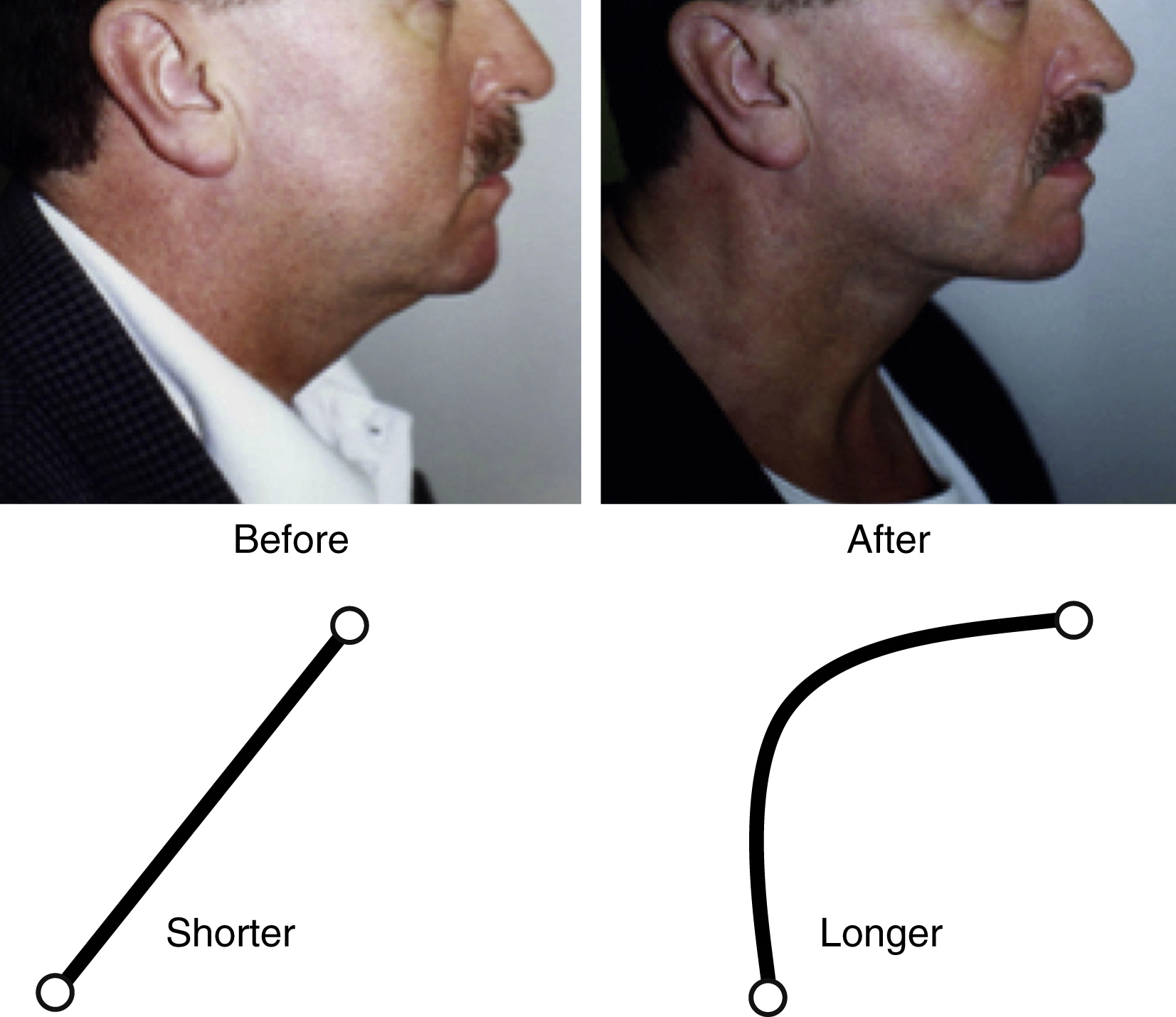
This is due to the fact that, unlike liposuction, a neck lift performed through a submental incision allows deep layer problems (subplatysmal fat excess and submandibular gland enlargement) and platysmal laxity typically present in the majority of patients seeking neck improvement to be addressed. This, however, begs the question, how can good neck contour be created without removing and tightening the skin, and what happens to the “excess” skin if only the deeper layer treatment is made and no skin is excised? The answer to this question is twofold. First, is the simple but often difficult to accept concept that in a properly performed neck lift contour is created by modification of deep layers of the neck and not by tightening of the skin, the covering layer. Skin stretches and relaxes, as we move and express ourselves; it is not intended to be a structural supporting layer, to hold up sagging muscle, fat and/or lift hypertrophied structures lying beneath it. The second part of the answer lies in the increase in neck surface area that occurs when deep neck contour is improved. Improving neck contour by excising redundant subplatysmal fat and performing other deep layer maneuvers as indicated, followed by the removal of lax platysma, will result in a deepened cervicomental angle, a longer curvilinear distance from the mentum to the sternal notch, a more concave, geometrically larger and longer neck surface ( Fig. 67.7 ). When neck skin is redraped and redistributed over the deeper, more concave surface, “excess” skin is absorbed and none need be removed.
These simple but not intuitive or immediately obvious facts underlie the reason that skin excision need not be performed in patients with good skin quality and mild to moderate skin excess to obtain a good result. In female patients good results can be obtained from short-scar neck lifts in patients up to their late thirties. In male patients satisfactory outcomes can be achieved in patients up to their late fifties.
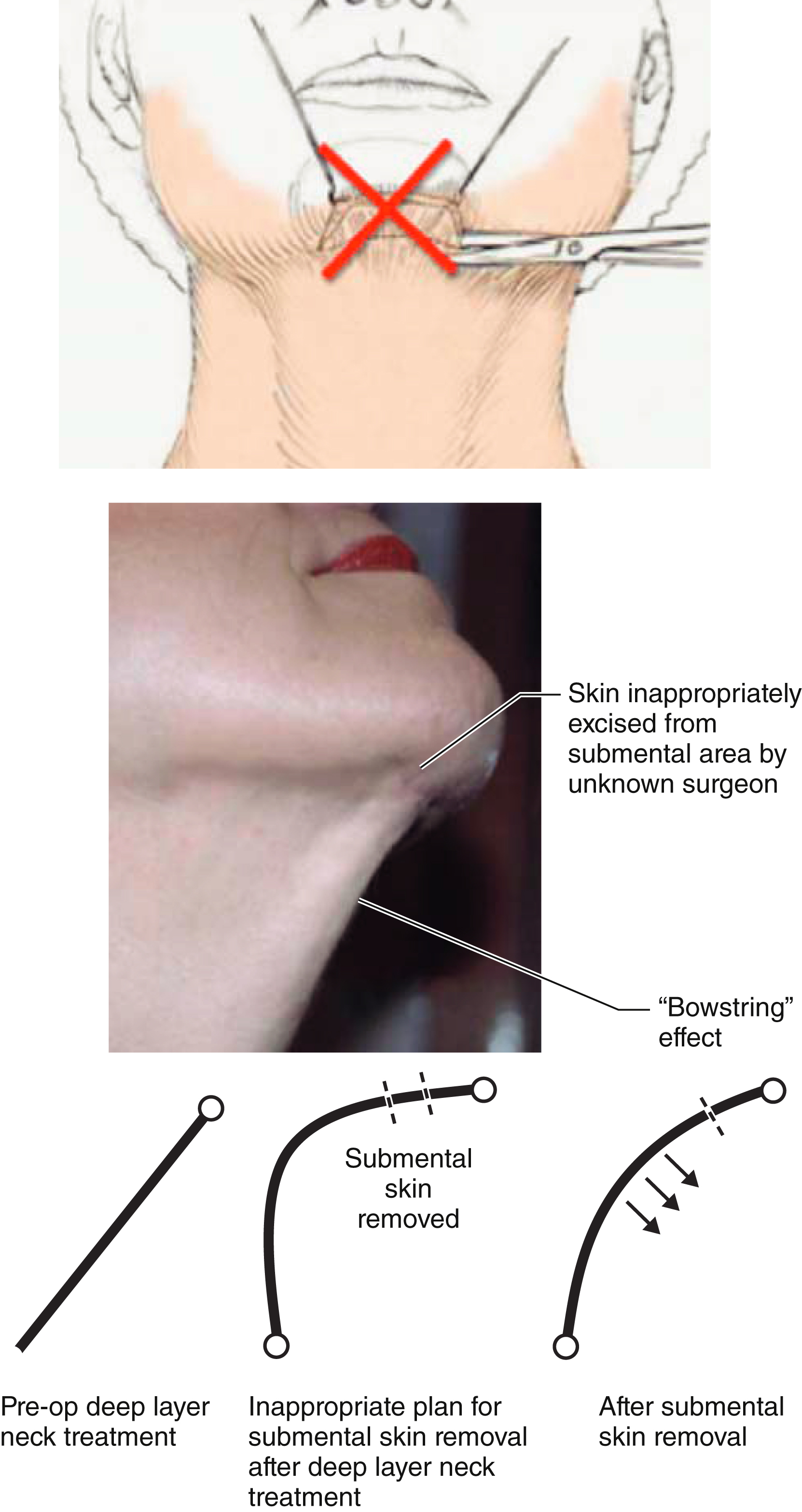
It is therefore clear why it is counterproductive to excise any skin from the submental incision, as this can create a “bow-string” effect and actually blunts the cervicomental angle. The submental skin incision is used for access to the neck only in a correctly performed neck lift, and if skin excision is necessary it is more practically, effectively, and logically removed from the postauricular area (extended neck lift or a facelift procedure) along a more appropriately directed lateral vector ( Fig. 67.8 ).
The results that can be obtained with a short-scar neck lift stand as compelling confirmation of the supremacy of the “deep layer” approach over more traditional procedures that mistakenly focused on skin excision, subcutaneous fat removal, and platysmal tightening.
There is a limit to the amount of neck skin that can be absorbed and managed by the short-scar neck lift technique, however, and an isolated neck lift performed through a submental incision only is typically best for male patients and younger women with mild to moderate skin excess, good skin elasticity, and minimal or modest aging in the midface, cheek, and jowl.
Neck Lift with a Chin Implant
The difference between the presence of poor neck contour and microgenia is commonly misunderstood, and it is a common misconception that placement of a chin implant improves neck contour. A chin implant is a treatment for microgenia – not a poor neckline – and the presence or absence of microgenia and the need for a chin implant is a cephalometric determination that is independent of the condition of the neck. Placement of a chin implant when microgenia is not present is a conceptual and artistic error that will create unnatural appearances.
When true microgenia is present however, placing a chin implant in combination with a neck lift will produce a more harmonious and balanced profile and a more esthetic and attractive cervicofacial profile ( Fig. 67.9 ).

“Extended” Neck Lift
If a significant amount of redundant skin is present, it must be excised to obtain the best result, and in such situations it is most logically and effectively excised in the postauricular areas using periauricular skin incisions. Skin excision can be combined with treatment of the neck through the submental incision as an “extended” or “long-scar” neck lift, or as part of a facelift procedure ( Figs. 67.10–67.12 ).



Neck Lift with Facelift
Practically speaking, most patients in need of a neck lift with skin excision also need a facelift. It is unusual to encounter patients with excess skin in the neck but not elsewhere on the face. This is particularly true in women and it is esthetically inappropriate to perform an isolated neck lift in most women who present for facial rejuvenation. Lifting only the neck but not the cheeks, jowls, and jawline can create an unnatural and unfeminine appearance.
Combining a facelift with a neck lift is almost always the best approach to obtain a balanced, natural, and harmonious rejuvenation of the female face, although not all patients will recognize or accept this (see Fig. 67.12 ). Performing a facelift in combination with a neck lift also allows for more complete and comprehensive removal of neck skin. And while many men will be put off by the idea of a “facelift,” they will readily agree to undergo the more palatable sounding “extended neck lift” procedure.
Surgical Planning in Neck Lift
Planning the Submental Incision
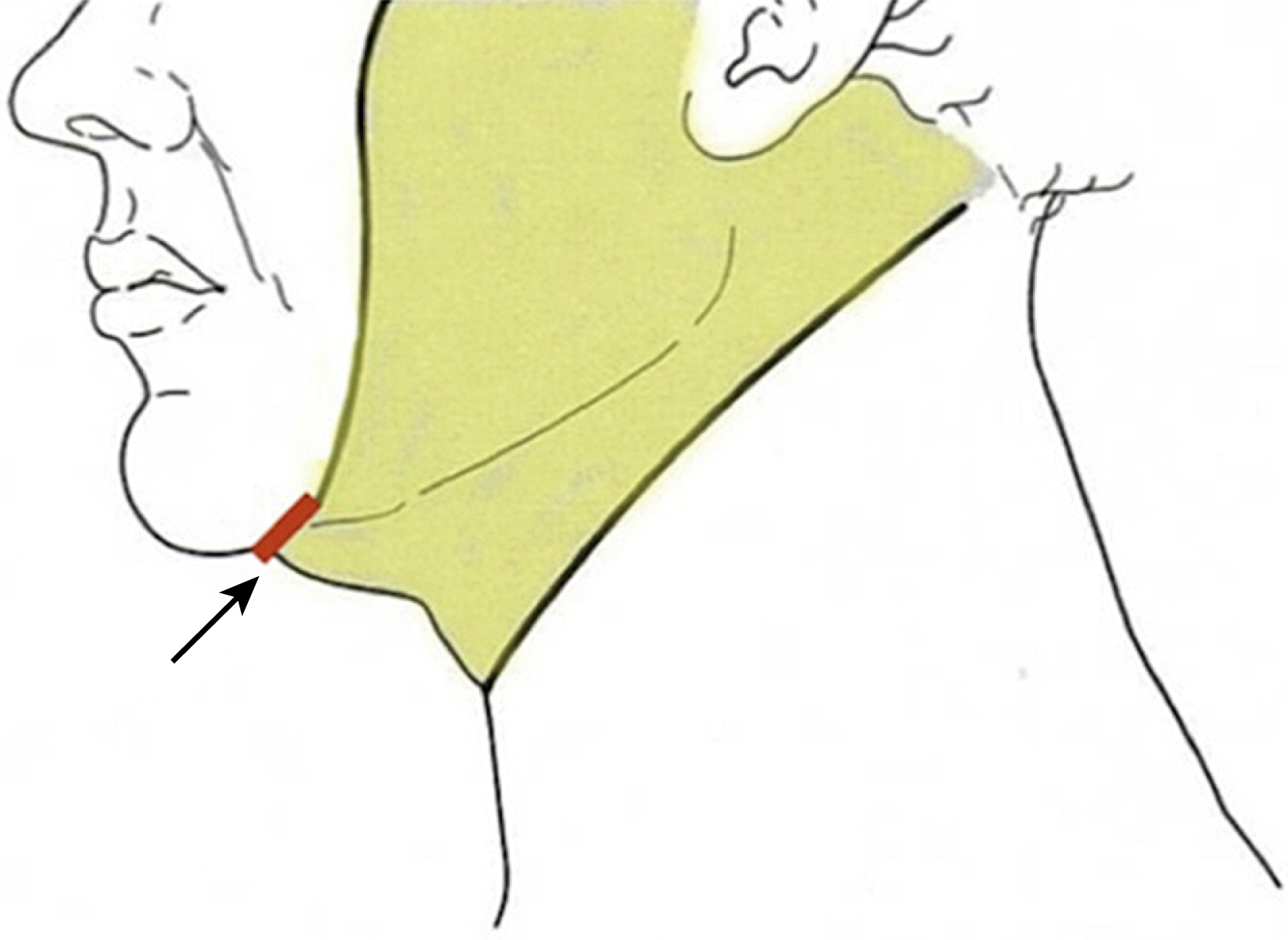
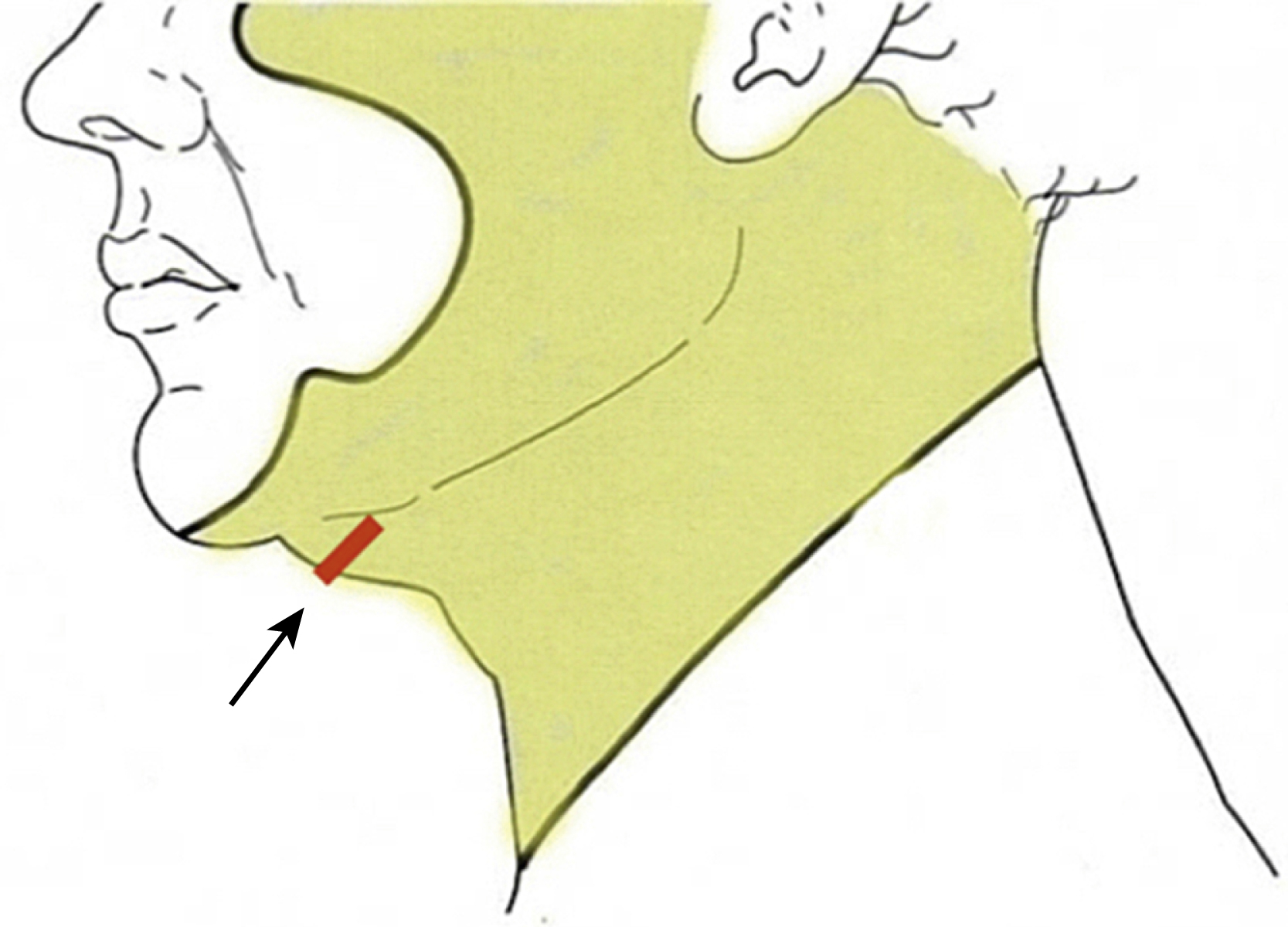
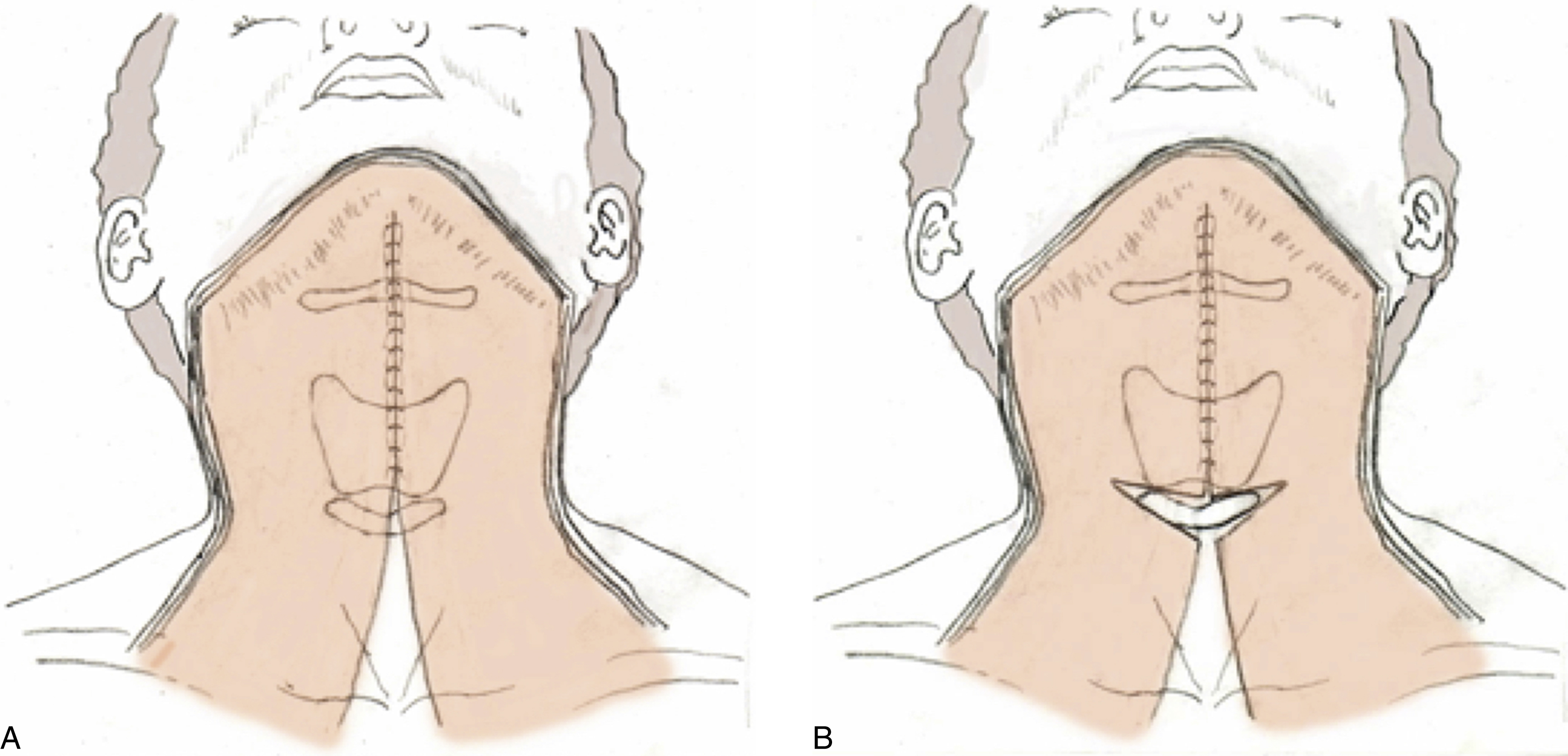
Whether performing a neck lift alone or in combination with a facelift, optimal improvement in the neck cannot generally be obtained in most patients without a submental incision. Traditionally, this incision is placed directly in and along the submental crease in a well-intended but counterproductive attempt to conceal the resulting scar ( Fig. 67.13 ).
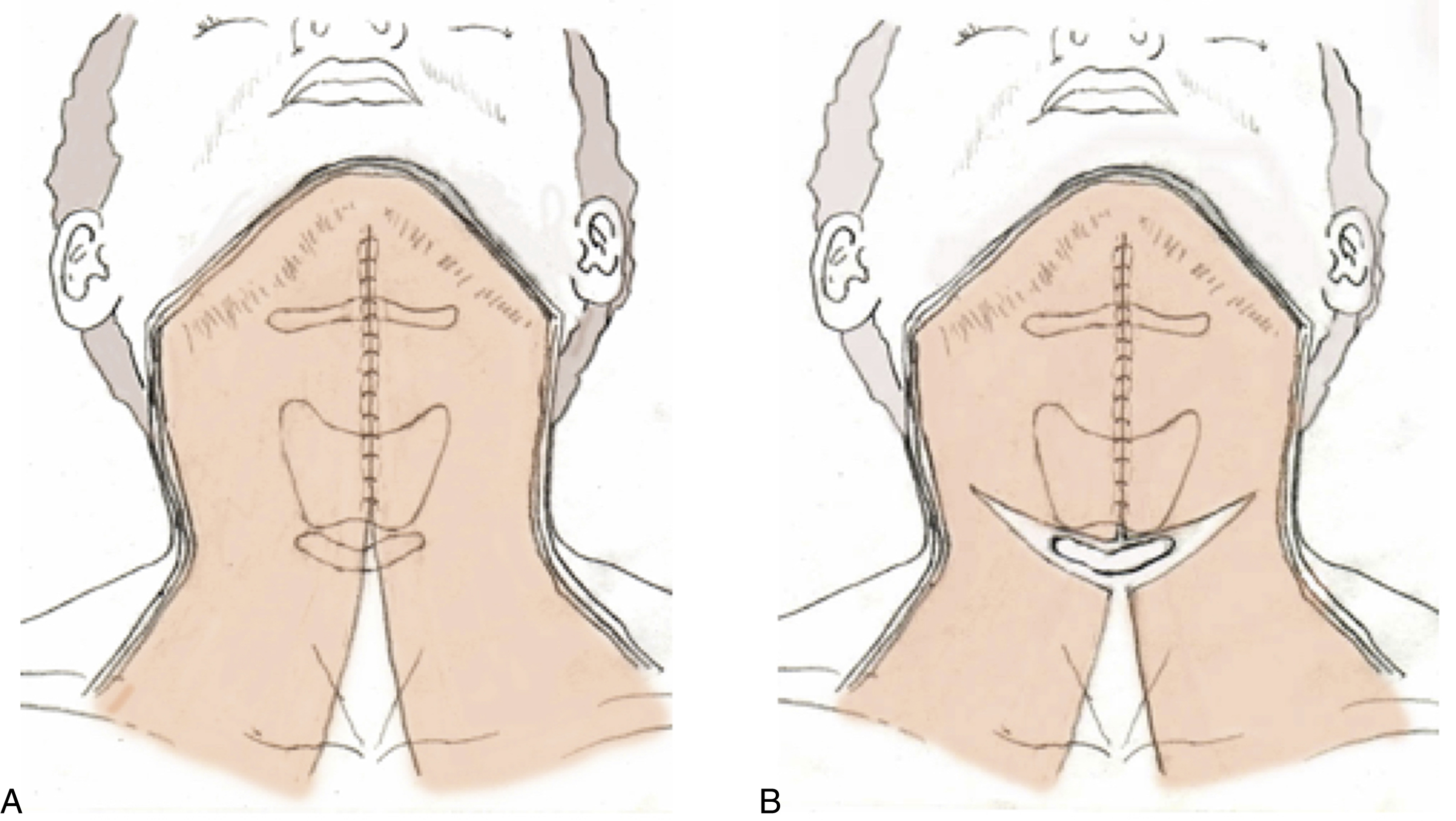
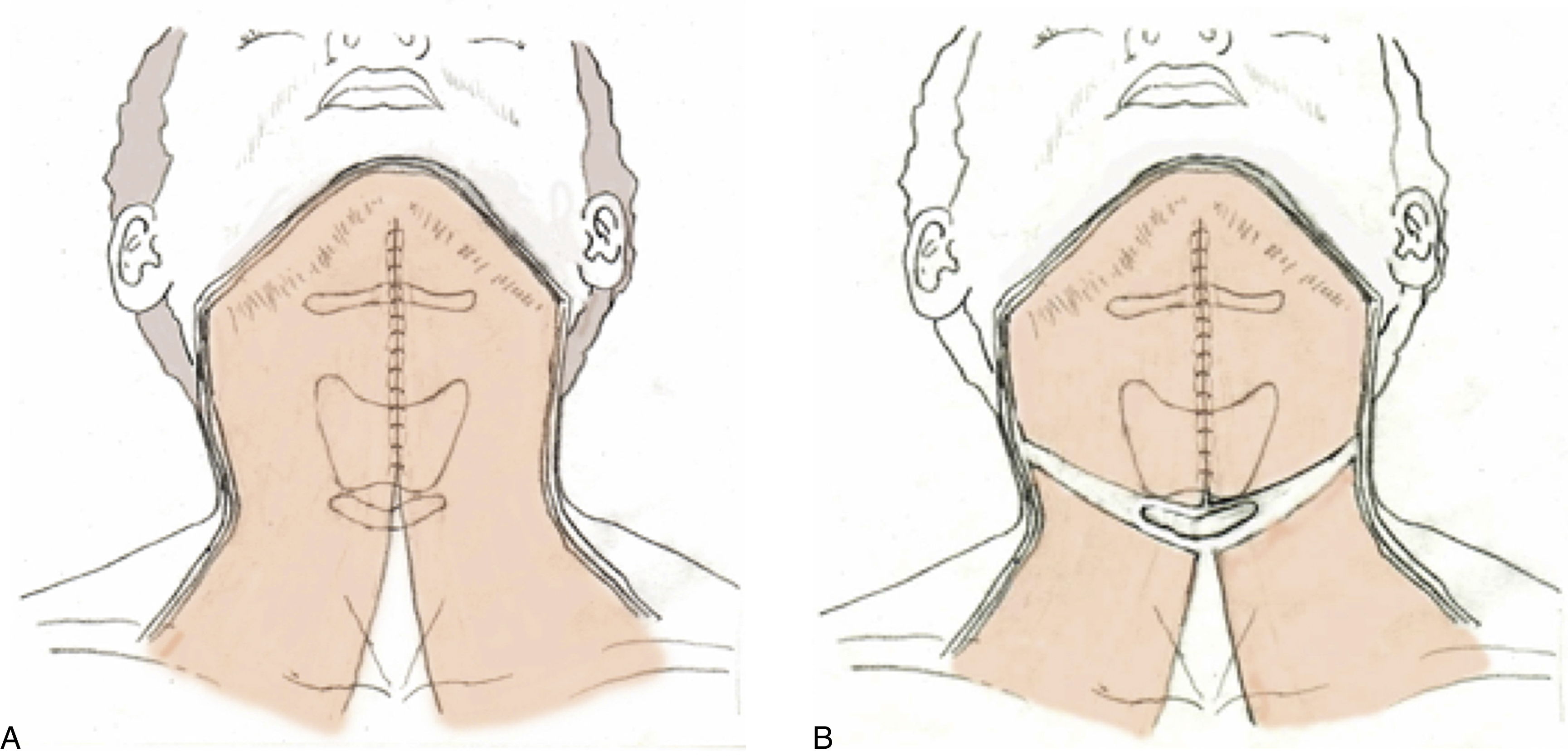
This, however, will surgically reinforce the crease and accentuate a “double chin” or “witch’s chin” deformity. Exposure of the submental region will also be compromised, and difficulty will be encountered when suturing or dissecting low in the neck. A more posterior placement of this incision will eliminate these problems, but still result in an inconspicuous and well-concealed scar ( Figs. 67.14–67.16 ).


The incision should be approximately 3–3.5 cm in length, but may be made longer, as long as neither end will be advanced up upon a visible portion of the face when skin flaps are shifted. Healing will be best, and the scar will be best concealed, if it is made as a straight, and not as a curved line ( Fig. 67.17 ).
Planning Treatment of the Platysma
As surgeons have pursued improved outcomes in treating the neck, our understanding of the origin of platysma muscle irregularities has improved and platysma muscle treatment techniques have evolved. Experience has shown that the traditional notion that platysma tightening will correct deep layer, neck problems, including accumulations of subplatysmal fat and the presence of large submandibular glands and protruding digastric muscles, was misguided, and that correct treatment of these problems will require “deep layer” procedures that address the actual anatomical problems present. Over time, thoughtful surgeons have come to understand and accept that a sustained improvement in neck contour is not created by platysma tightening, but by these deep layer maneuvers (subplatysmal fat excision, submandibular gland reduction, and partial digastric myectomy) that specifically target these problems.
Experience has also confirmed that traditional platysma tightening will not universally correct “platysma bands,” and that our traditional view that all platysma bands were a homogenous problem and simply a product of age-associated horizontal platysmal laxity was conceptually flawed and the underlying cause of many decades of failed treatments. In reality “platysma bands” comprise a heterogeneous group of distinct problems, and for many patients platysma bands can be seen to be the product of not only horizontal laxity but longitudinal platysmal hyperfunction , and as such, refractory to traditional horizontal lifting and pulling procedures. Correct treatment of these problems requires horizontal platysma transection to disrupt longitudinal hyperfunction, or treatment by other like means.
Assessing Platysma Deformity
The cervicosubmental region of each patient must be carefully examined both at rest and during platysmal activation if complete assessment of platysmal deformity is to be made. This is best accomplished by asking the patient to “push the jaw forward and tighten the neck.” It is often helpful if the surgeon demonstrates this maneuver first for the patient to be sure it is correctly performed. Frequently, an insignificant appearing deformity at rest will be obvious upon muscle activation ( Fig. 67.18 ). Failure to recognize and appropriately correct these “ dynamic deformities ” is the reason too many facelift patients appear improved in repose but unnatural or bizarre in conversation, animation, and during other activities that result in platysma muscle activation.

Examination of the cervicosubmental region with and without platysmal activation allows one to distinguish between “hard” dynamic and “soft” a dynamic cervical bands. Soft, adynamic bands change little during platysma activation and are predominantly a problem of loose skin or horizontal platysmal laxity. Hard dynamic bands become tight or exaggerated upon platysmal activation and indicate a problem of longitudinal platysmal hyperfunction.
If submental support is poor due to horizontal platysmal laxity or platysmal diastasis and optimal improvement in the anterior neck is desired, anterior platysmaplasty is planned ( Fig. 67.19 ). In this procedure, the medial borders of the platysma muscle are sutured together to help consolidate the neck, reduce horizontal platysmal laxity, and improve neck appearance when the patient flexes the neck and looks down (see Fig. 67.11 ). It is not , however, adequate or effective in the treatment of excess subplatysmal fat, prominent submandibular glands, hypertrophy of the anterior bellies of the digastric muscles, or the treatment of “hard” dynamic platysmal bands. Not recognizing and acknowledging this fact, and well-intended but misguided attempts to treat these problems by medial or lateral platysmal pulling and tightening, has led to frustration for many surgeons treating the aging neck. Treatment of these problems will require that other maneuvers discussed elsewhere in this chapter be performed.
It is important to distinguish between “soft” adynamic playsmal bands and “hard” dynamic bands as treatment will vary depending on the type present. Patients with soft bands are usually adequately treated with skin excision or skin excision and platysmaplasty alone. Patients with “hard” bands however require transverse platysma myotomy or some other procedure that disrupts longitudinal platysma muscle hyperfunction and prevents the muscle from contracting upon itself. Much like when a dancer ruptures their Achilles tendon they cannot point their toe, dividing the platysma transversely prevents it from pulling itself away from the anterior surface of the neck. The result of platysma myotomy when correctly performed is dramatic, long-lasting, and superior to any suture, suture suspension, lateral suspension of the platysmal border, or “corset” platysmal tightening technique ( Fig. 67.20 ). The length of transection required can be varied depending on the location and configuration of bands present, and may thus differ from patient to patient. The key to success in treating hard, dynamic bands is to recognize that they are the product of longitudinal platysma muscle hyperfunction and not one of horizontal platysma laxity, and employing a plan of treatment that recognizes this fact. Pulling medially or laterally on the platysma muscle borders as commonly advocated does not address the origin of dynamic platysma bands, and is not a logical or effective treatment of them. Likewise, attempts to vertically excise dynamic platysma bands along the length of the muscle fibers is not a logical or effective treatment, as the band is not fixed in location and any such a maneuver does not address overall longitudinal muscle hyperfunction.
Platysmal bands are generally seen to lie in medial and lateral locations and are often referred to as anterior and lateral platysma bands (see Fig. 67.18D ). Each band is situated near the medial and lateral platysma muscle borders, but does not usually correlate precisely with them and is not specifically fixed in location. Patients with anterior platysmal bands only can be treated with a partial transverse platysma myotomy by dividing the muscle medially and subtotally through and beyond the section of it in which the band is present low in the neck at the level of the cricoid cartilage ( Fig. 67.21 ). The platysma muscles need not be completely transected when an anterior band only is present, just the region where the platysmal band is located.
If lateral , as well as anterior bands are present, the myotomy is carried more laterally to include them as well ( Fig. 67.22 ). If poor definition is present over the lateral mandibular border, in addition to anterior and lateral neck bands, or if comprehensive improvement is desired, platysmal myotomy is planned to continue “full width” superior-laterally up to the anterior border of the sternocleidomastoid muscle ( Fig. 67.23 ). A similar full-width myotomy of this type is also indicated in a firm obtuse neck with a “short platysma” and poor definition over the mandibular angle, but no bands.
In theory and principle, in many necks a subtotal myotomy only is indicated and need be performed. As a practical matter, however, complete transection of the platysma is typically performed in most of our patients when any form of myotomy is indicated to limit the possibility of band reoccurrence in areas of muscle that were not divided, or that residual platysma bands will be present. Despite assertions to the contrary, full-width platysma myotomy will not result in an overly thin appearing neck (“lollipop neck”), or “reduced support” of the submandibular glands when correctly performed. These are merely false assertions put forth by surgeons who do not perform the procedure and do not want to take the time and trouble of learning and performing it.
Medial wedge resections of platysma at the hyoid and vertical excisions of platysma bands, while shown in many textbooks, are not typically effective in treating dynamic platysma bands in that a large segment of adjacent and more laterally situated muscle remains untreated. Vertical excision of platysma bands while still advocated by some has proven to be an ineffective treatment that has been abandoned by experienced surgeons. Trying to isolate and specifically excise the responsible muscle segment is difficult at best since the band is not specifically fixed in its location, and a partial excision along a vertical axis typically allows or incites new bands to form in an adjacent untreated area.
Medial wedge resections of platysma at the hyoid can result in unesthetic exposure of underlying cervical anatomy, a harsh transition from the submental region to the neck, as well as lower lip dysfunction and asymmetric smile. These procedures are not recommended in routine treatment of platysmal bands although they may be useful in certain secondary cases and in situations where there has been fibrosis and scarring of the platysma in that area. These problems can result from noninvasive treatment of the neck with radiofrequency, ultrasound, internal tissue heating, cryolipolysis, chemolipolysis, laser liposuction, and the use of inflammatory fillers in the neck area. When these problems are present a “high” myotomy (division at the level of the thyroid cartilage rather than the cricoid), or even a partial myectomy (excising damaged platysma muscle from the anterior neck at the level of the thyroid cartilage) may be indicated.
Similarly, attempts to place rigid support across the cervicomental angle in the form of a mastoid to mastoid “noose” of suture or commercially available straps to lift platysmal bands is conceptually flawed and practically problematic. Experience has shown that these maneuvers do not work and are the source of many patient problems.
Assessing the Anatomical Basis of Neck Problems
Planning the Modification of the Submental Region
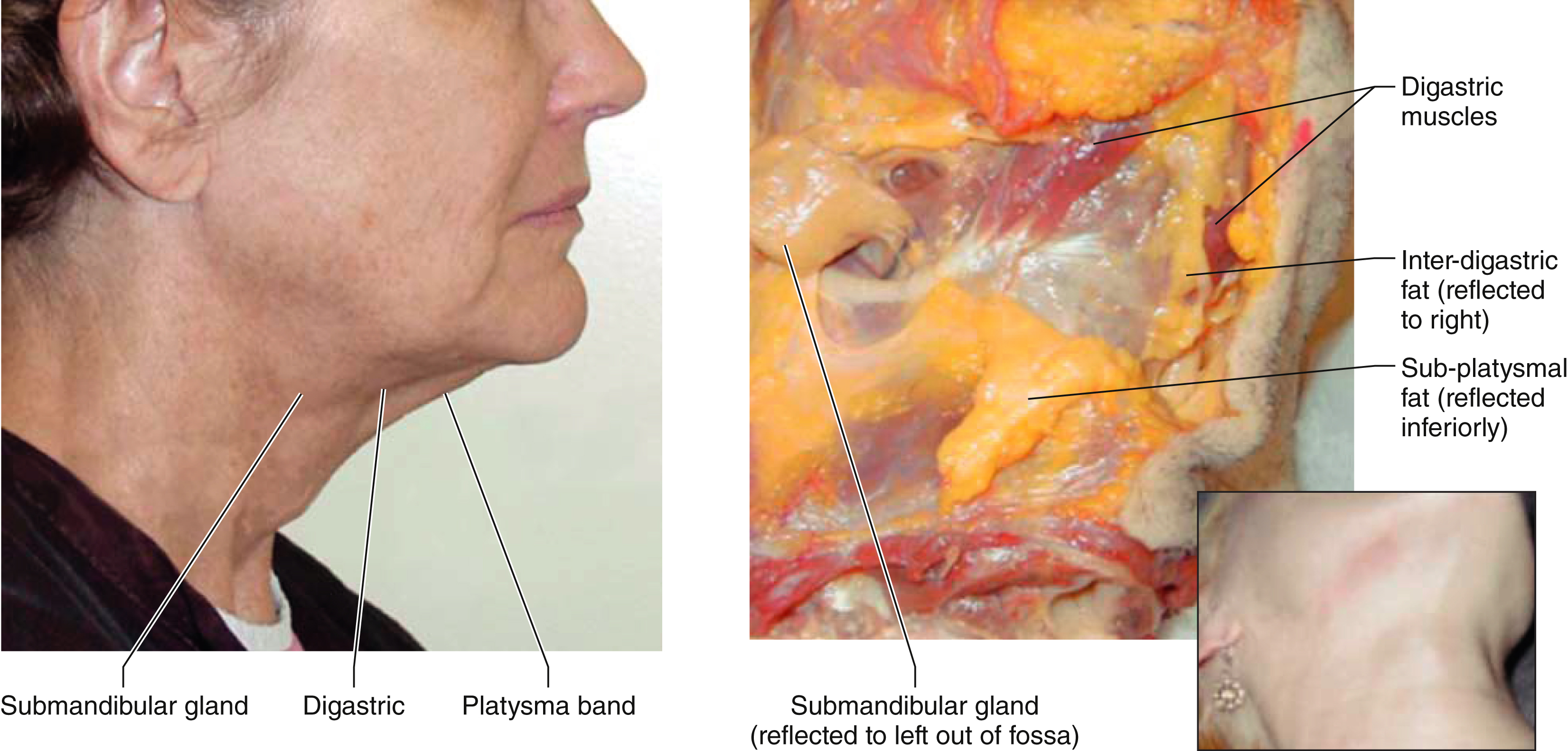
Traditional neck lift techniques do not adequately address many aspects of aging in the submental region and it is not enough in most situations to limit treatment of the neck to preplatysmal lipectomy alone or with postauricular skin excision. For many patients subplatysmal fat accumulation, submandibular salivary gland “ptosis” (enlargement), and digastric muscle hypertrophy will contribute significantly to the neck deformity present and necessitate additional treatment if optimal improvement is to be obtained ( Fig. 67.24 ). It must be acknowledged and accepted that simply tightening the platysma and creating a tight platysma “corset” over these problems will not correct them and will not produce a sustained improvement in neck contour if underlying deep layer problems are not addressed.
Identifying the Neck with Excess Subplatysmal Volume
The presence of abnormal fullness in the submental space can be demonstrated preoperatively by taking and examining a lateral-looking down view photograph (Connell’s view) of the patient’s neck ( Fig. 67.25 ). Often a neck that looks reasonably good in the straight lateral view will be revealed to be unexpectedly full when the patient looks down as they would when looking at work on their desk, a menu at a restaurant, or their phone screen. Failure to appreciate subplatysmal fullness preoperatively and treat it appropriately intraoperatively will result in compromised outcomes.

Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


