Naso-Orbital-Ethmoid (NOE) Fractures
Craig Birgfeld
Joseph Gruss
DEFINITION
Naso-orbital-ethmoid (NOE) fractures are fractures of the bones of the central face between the orbits involving the nose, the orbits, and the ethmoid sinuses.
ANATOMY
The NOE region is comprised of the confluence of the nasal bones, the frontal process of the maxilla, the internal angular process of the frontal bone, the lamina papyracea of the ethmoid bone, and the lacrimal bone (FIG 1A).
The NOE framework defines the nasal dorsum, the volume of the orbits, the shape of the medial orbits, and the support of the central face.
Fractures tend to extend across the nasofrontal junction, down the medial orbital wall, across the inferior orbital rim, and across the medial buttress into the pyriform aperture (FIG 1B).
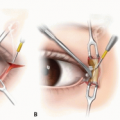
NOE fractures include the complex anatomy of the medial canthal tendon attachments and nasolacrimal apparatus (FIG 1C).
PATHOGENESIS
NOE fractures generally occur from blunt force trauma to the central face between the eyes, such as hitting the steering wheel or dashboard during an MVC.
They frequently occur from self-inflicted gunshot wounds across the temple and orbits.
NOE fractures are often components of more complex fracture patterns such as frontal sinus fractures and panfacial fractures.
NATURAL HISTORY
Without treatment, patients can suffer upper airway obstruction from impaction of the pyriform aperture and/or loss of nasal support resulting in a saddle nose deformity (FIG 2).
Impacted and comminuted NOE fractures can change orbital volume leading to enophthalmos, dystopia, and diplopia.
Damage to the nasolacrimal apparatus can lead to epiphora.
Disruption of the nasofrontal outflow tract with an impacted NOE fracture can lead to frontal sinus congestion and mucocele formation.
Untreated NOE fractures can significantly alter physical appearance.
PATIENT HISTORY AND PHYSICAL FINDINGS
Patients generally present with a history of blunt force trauma to the central upper face between the orbits.
They may report airway obstruction, epiphora, diplopia, and alteration of physical appearance.
Physical exam should focus first on vision, extraocular muscle involvement, and globe position.
Patients may display telecanthus (an increased distance between the medial canthal tendons that is greater than 35 mm in adults) and hence a shortened palpebral fissure.
The loss of dorsal nasal support leads to a saddle nose deformity with loss of nasal bridge, upturned nasal tip, and an increased nasolabial angle (normal = 90-100 degrees; FIG 3).
A speculum exam should be performed to assess impaction of the lateral nasal sidewall and rule out septal fracture and/or hematoma.
IMAGING
Fine cut (0.3-0.5 mm) maxillofacial CT scans with, at a minimum, axial and coronal views are necessary for accurate diagnosis (FIG 4A,B).
Three-dimensional reconstructions are helpful to delineate anatomy and plan reduction maneuvers (FIG 4C).
Sagittal views can be helpful if orbital floor fractures are also present.
DIFFERENTIAL DIAGNOSIS
Isolated nasal bone fracture
Isolated medial orbital wall fractures
NONOPERATIVE MANAGEMENT
Nondisplaced NOE fractures can be managed conservatively with activity precautions and protection of the nasal dorsum with a splint.
SURGICAL MANAGEMENT
Surgical intervention is reserved for displaced NOE fractures.
The complexity of the intervention is determined by the amount of displacement and comminution of the segments.
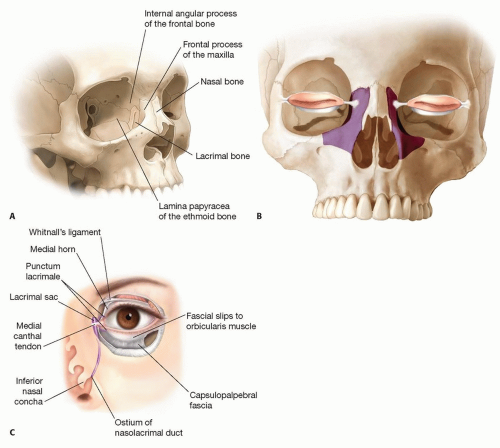
FIG 1 • A. The Naso-orbital-ethmoid complex is formed by the confluence of the nasal bones, the frontal process of the maxilla, the internal angular process of the frontal bone, the lamina papyracea of the ethmoid bone, and the lacrimal bone. B. Typical fracture locations of a noncomminuted bilateral NOE fracture. C. NOE fractures involve the complex attachments of the medial canthal tendon and the nasolacrimal apparatus.
The goal of surgical management is to restore facial harmony by focusing on the following features:
Establish dorsal nasal support
Ensure airway patency
Restore normal orbital volume
Return the intercanthal distance to within normal range
 FIG 2 • Loss of dorsal nasal support frequently occurs with NOE fractures. |
Preoperative Planning
Review of CT scans will allow planning of surgical approaches necessary to restore normal anatomy, the maneuvers necessary for reduction, and the amount and placement of rigid fixation needed for a stable framework.
Two classification systems aid in preoperative planning:
Manson (focus on central segment and canthal attachment):1
Type 1: single segment (FIG 5A)
Type 2: comminuted (FIG 5B)
Type 3: comminuted into the canthal insertion (FIG 5C)
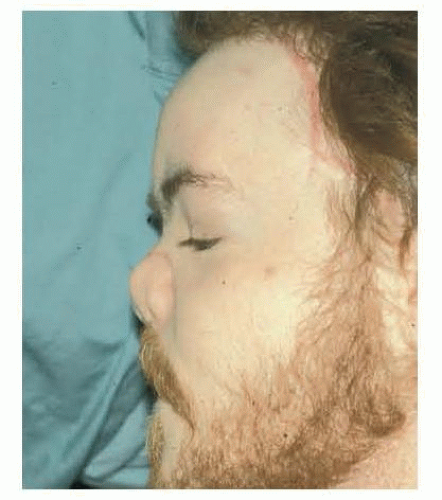
FIG 3 • Untreated NOE fractures can lead to a “saddle nose” deformity.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access