Key Words
nail diseases, nail psoriasis, nail lichen planus, fungal nail infection, onychomycosis, leukonychia, nail ridging, nail splitting, nail dystrophy, spoon nails, acute paronychia, nail tinea, subungual hematoma, Beau lines
See pages 963–964 for photos of the most common nail disorders.
Anatomy and Physiology
Anatomy.
The nail unit consists of several components ( Fig. 25.1 ). The nail plate is hard, translucent, dead keratin. The nail fold includes the skin surrounding the lateral and proximal aspects of the nail plate. The proximal nail fold overlies the matrix. Its keratin layer extends onto the proximal nail plate to form the cuticle. Capillary loops at the tip of the proximal nail fold are normally small and nonapparent, but they become distinct in diseases such as systemic lupus erythematosus and scleroderma. The proximal nail fold epithelium covers the proximal nail plate for a few millimeters and then makes a 180-degree turn and curves back into direct contact with the nail plate. It makes another 180-degree turn and becomes continuous with the nail matrix.
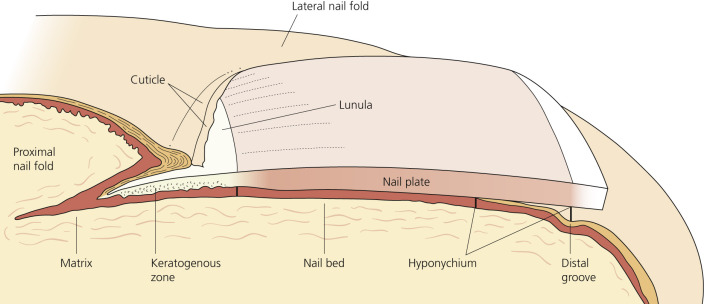
The matrix epithelium synthesizes 90% of the nail plate. The lunula (white half-moon), which is visible through the nail plate, is the distal aspect of the nail matrix. It is continuous with the nail bed. The nail bed extends from the distal nail matrix to the hyponychium. As the nail streams distally, material is added to the undersurface of the nail, thickening it and making it densely adherent to the nail bed. The nail bed consists of parallel longitudinal ridges with small blood vessels at their base ( Fig. 25.2 ). Bleeding induced by trauma or vessel disease, such as lupus, occurs in the depths of these grooves, producing the splinter hemorrhage pattern viewed through the nail plate. The hyponychium is a short segment of skin lacking nail cover; it begins at the distal nail bed and terminates at the distal groove. Damage to specific regions of the nail unit will result in unique nail findings ( Table 25.1 ).
| Affected Site | Clinical Manifestation |
|---|---|
| Proximal matrix | Beau lines Pitting Longitudinal ridging Longitudinal fissuring Trachyonychia |
| Distal matrix | True leukonychia |
| Proximal + distal matrix | Onychomadesis Koilonychia Nail plate thinning Onychauxis (nail plate hypertrophy or thickening) |
| Nail bed | Onycholysis Subungual hyperkeratosis Apparent leukonychia Splinter hemorrhages |
Nail Biopsy.
Ungual biopsies are used to diagnose tumors, inflammatory disease, and infections. A punch or excisional biopsy technique is chosen, which provides a sufficient amount of tissue and produces a minimal amount of scarring. In practice these procedures are performed by some dermatologists and orthopedic hand surgeons. All of these techniques have been described.
Growth Rates.
Nails grow continuously, but their growth rate decreases both with age and with poor circulation. Fingernails, which grow faster than toenails, grow at a rate of 0.5 to 2 mm per week. It takes approximately 5.5 months for a fingernail to grow from the matrix to the free edge and approximately 12 to 18 months for a toenail to be replaced. A reduction in the rate of matrix–cell division occurs in the presence of systemic diseases such as scarlet fever, causing thinning of the nail plate (Beau lines).
Normal Variations
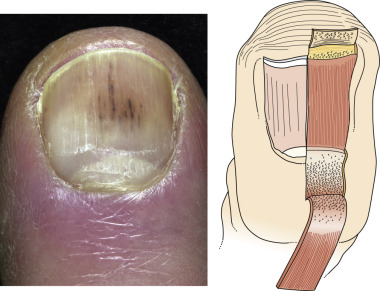
The shape and opacity of the nail vary considerably among individuals. Aging may increase or decrease nail thickness. Longitudinal ridging ( Fig. 25.3 ) is common in aging patients, but this variant is occasionally observed among the young. Beading occurs at all ages but is more common in the elderly ( Fig. 25.4 ). The beads cover part or most of the plate surface and are arranged longitudinally. A pigmented band or bands occur in more than 90% of black people ( Fig. 25.5 ). The sudden appearance of such a band in white people necessitates further investigation.



























Nail structure can be altered by primary skin diseases, infections, trauma, internal diseases, congenital syndromes, and tumors. A more detailed discussion with illustrations of the most commonly encountered entities is presented in the following sections.
Nail Disorders Associated With Skin Disease
Psoriasis.
Nail changes are characteristic of psoriasis (see p. 282 ), and the nails of psoriasis patients should be examined. These changes offer supporting evidence for the diagnosis of psoriasis when skin changes are equivocal or absent.
The incidence of nail involvement in psoriasis varies from 10% to 50%. Nail involvement usually occurs simultaneously with skin disease but may occur as an isolated finding. More than 50% of patients suffer from pain, and many are restricted in their daily activities.
Onycholysis.
Psoriasis of the hyponychium results in the accumulation of yellow, scaly debris that elevates the nail plate. The debris is commonly mistaken for nail fungus infection. Psoriasis of the nail bed causes separation of the nail from the nail bed. Unlike the uniform separation caused by pressure on the tips of long nails, the nail detaches in an irregular manner ( Fig. 25.6 ). The nail plate turns yellow, simulating a fungal infection. Separation begins at the distal groove or under the nail plate and may involve several nails.

Nail Deformity.
Extensive involvement of the nail matrix results in a nail losing its structural integrity, resulting in fragmentation and crumbling. Gross alteration of the nail plate surface and nail bed splinter hemorrhages are common ( Fig. 25.7 ).

Pitting.
Pitting, or sharply defined ice pick–like depressions in the nail plate, is the most common finding ( Fig. 25.8A–B ). The number, distribution, patterns, and depth vary. Nail plate cells are shed in much the same way as psoriatic scale is shed, leaving a variable number of tiny, punched-out depressions on the nail plate surface. They emerge from under the cuticle and grow out with the nail. Many other cutaneous diseases may cause pitting (e.g., eczema, fungal infections, and alopecia areata), or it may occur as an isolated finding in a normal variation.



Oil Spot Lesion.
Psoriasis of the nail bed may cause localized separation of the nail plate. Cellular debris and serum accumulate in this space. The brownish-yellow color ( Fig. 25.8C ) observed through the nail plate looks like a spot of oil.
Treatment
Nail psoriasis is difficult to treat, but may respond to different approaches used alone or together. A Cochrane Library review in 2013 showed the following results. There was significant improvement of nail psoriasis compared to placebo: with infliximab, golimumab, superficial radiotherapy, electron beam, and grenz rays. Radiotherapy for psoriasis is not used in common practice. The evidence for the use of topical treatments is inconclusive and of poor quality; however, this does not imply that they do not work. There is little merit in treating psoriatic nails with photochemotherapy (PUVA) or topical 5-fluorouracil (5-FU). Indigo naturalis extract in oil (Lindioil) has been reported to be successful with twice daily application after 12 weeks. No side effects have been reported with this regimen.
Triamcinolone Acetonide.
Intralesional injection at monthly intervals into the matrix with triamcinolone acetonide (2.5 to 10 mg/mL) delivered with a 30-gauge needle is the standard treatment for psoriatic nail disease used by most dermatologists. A simplified protocol has been proposed. Triamcinolone acetonide (0.4 mL, 10 mg/mL) is injected, following ring block, at each of four periungual sites: two at the nail matrix and one in each lateral nail fold, directed medially towards the nail bed. This method is utilized to achieve delivery of the agent to both the nail matrix and the nail bed. If needed, a second set of injections is administered after 2 months. Subungual hyperkeratosis, ridging, and thickening respond well. Benefits are sustained for at least 9 months. Onycholysis and pitting are less responsive.
Calcipotriene (Calcipotriol).
Application of calcipotriene cream or ointment once daily every weeknight and clobetasol once daily every weekend for 6 months followed by clobetasol twice weekly for the second 6 months reduces subungual hyperkeratosis. Use of calcipotriene ointment twice daily for up to 5 months is less effective. Calcipotriene 0.005% and betamethasone dipropionate 0.064% solution is a combination that may be effective with once-daily application to nails and nail folds.
Tazarotene.
Tazarotene 0.1% gel is applied each evening for up to 24 weeks to fingernails. Medication can be used under occlusion or nonoccluded. Tazarotene gel reduced onycholysis (in occluded and nonoccluded nails) and pitting (in occluded nails).
Biologic Drugs.
TNF-α inhibitors (adalimumab, etanercept, infliximab, certolizumab and golimumab), ustekinumab, apremilast and tofacitinib have been utilized to treat refractory nail psoriasis.
Traditional systemic medications such as methotrexate, acitretin, and cyclosporine may be administered for nail psoriasis.
Pustular Psoriasis of the Nail Apparatus
Pustular psoriasis of the nail bed, matrix, or surrounding skin is common and may be painful. It has a chronic course and poor response to treatment. Severe cases are treated with systemic retinoids. Topical calcipotriene is effective in about 50% of patients with localized disorder and is also useful as maintenance therapy after retinoid treatment. Calcipotriene 0.005% and betamethasone dipropionate 0.064% ointment is a combination that may be more effective than calcipotriene alone.
Lichen Planus
Approximately 25% of patients with nail lichen planus (LP) have LP in other sites before or after the onset of nail lesions. Nail LP usually appears during the fifth or sixth decade of life.
Metal allergies have been implicated. Metal patch tests were positive in 30% of patients. Improvement of the skin lesions was seen following removal of dental materials containing causative metals or systemic disodium cromoglycate therapy.
The matrix, nail bed, and nail folds may be involved in producing a variety of changes, few of which are characteristic. Minimal inflammation of the matrix induces longitudinal grooving and ridging, which are the most common findings of LP of the nail. The development of severe and early destruction of the nail matrix with scarring characterizes a small subset of patients with nail LP. A pterygium, caused by adhesion of a depressed proximal nail fold to the scarred matrix, may occur after intense matrix inflammation ( Fig. 25.9 ). The nail plate distal to this focus is either absent or thinner. In most cases, nail LP is self-limiting or promptly regresses with treatment. Permanent damage to the nail is uncommon, even in patients with diffuse involvement of the matrix. Matrix lesions may respond to intralesional triamcinolone acetonide (2.5 to 5 mg/mL) delivered with a 30-gauge needle every 3 or 4 weeks. Severe cases respond to prednisone (20 to 40 mg/day). This may require a long course of treatment in which the possible risks may outnumber the advantages. Onychomycosis may be confused clinically with LP.

Acquired Disorders
Bacterial and Viral Infections
Acute Paronychia.
The rapid onset of painful, bright red swelling of the proximal and lateral nail folds may occur spontaneously or may follow trauma or manipulation ( Figs. 25.10 and 25.11 ). Superficial infections present with an accumulation of purulent material behind the cuticle (see Fig. 25.11 ). The small abscess is drained by inserting a 23- or 21-gauge needle tip or similar instrument between the proximal nail fold and the nail plate and lifting the nail fold with the tip of the needle ( Fig. 25.12 ). Pain is abruptly relieved as the purulent material drains. There is no need for anesthesia or daily dressing. A diffuse, painful swelling suggests deeper infection, and cases that do not respond to antistaphylococcal antibiotics may require deep incision. Acute paronychia rarely evolves into chronic paronychia.



Treatment.
In patients with a red and painful nail fold with no abscess, treat with warm saline soaks three to four times a day and antistaphylococcal antibiotics (cephalexin, clindamycin, amoxicillin plus clavulanate, trimethoprim–sulfamethoxazole). A group II or III corticosteroid such as betamethasone dipropionate cream may suppress inflammation and pain.
Pus under the nail plate is drained. Lift the nail fold off the nail with a needle or remove part or all of the nail plate. Remove the portion of the nail plate overlying the abscess. When there is no pus under the nail plate but an abscess in the nail fold, drainage via skin edge elevation from the nail plate is first attempted under a digital block. This can be done effectively with a 21- or 23-gauge needle, a small scissor, or a Freer elevator. If some pus still seems to remain undrained, a portion of the nail plate is removed. Avoid incision of the eponychial skin when possible, but use incision if the abscess is most superficial. Some surgeons pack the space of the evacuated abscess with plain gauze, remove it after approximately 48 hours, and begin warm saline soaks three to four times a day.
Chronic Paronychia.
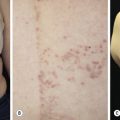
Chronic paronychia is not a yeast infection, but rather an inflammation of the proximal and lateral nail folds that may be colonized by Candida . Chronic paronychia evolves slowly and presents initially with tenderness and mild swelling around the proximal and lateral nail folds ( Fig. 25.13 ). Significant contact irritant exposure is a major cause. Individuals whose hands are repeatedly exposed to moisture (e.g., bakers, dishwashers, and dentists) are at greatest risk. Manipulation of the cuticle accelerates the process. Typically, many or all fingers are involved simultaneously. The cuticle separates from the nail plate, leaving the space between the proximal nail fold and the nail plate exposed to infection. Many organisms, both pathogens and contaminants, thrive in this warm, moist intertriginous space. The skin surrounding the nail becomes pale red, tender or painful, and swollen. Occasionally a small quantity of pus can be expressed from under the proximal nail fold. A culture of this material may grow Candida or Gram-positive and Gram-negative organisms. Candida is probably just a colonizer of the proximal nail fold rather than a direct cause of the disease. It disappears when the physiologic barrier is restored. The nail plate is not infected and maintains its integrity, although its surface becomes brown and rippled. There is no subungual thickening such as that present in some fungal infections. Proximal separation of the nail plate from the matrix area may occur as a consequence of nail matrix damage. The nail plate may sometimes present a green discoloration of its lateral margins as a result of Pseudomonas aeruginosa colonization. The process is chronic and responds very slowly to treatment. Psoriasis of the fingers may present in a similar form ( Fig. 25.14 ).


Treatment.
Resolution of chronic paronychia depends on avoidance of exposure to contact irritants and on treatment of underlying inflammation and infection. Every attempt must be made to keep the proximal nail fold dry. Patients should refrain from washing dishes and from washing their own hair. Wearing rubber or plastic gloves is of some value, but moisture accumulates in them with prolonged use. The hands stay dry if a cotton glove is worn under the rubber glove. Controlling inflammation is the primary goal. Topical steroid creams (group V) or tacrolimus ointment 0.1% applied twice daily for up to 3 weeks is more effective than systemic antifungals. Oral antibiotics do not penetrate this distal site in sufficient concentration, and the variety of organisms is too numerous to respond to a single oral agent. Treatments to keep the space between the nail plate and proximal nail fold dry may help. Place fungoid tincture (miconazole), ciclopirox (olamine) topical suspension, or one or two drops of 3% thymol in 70% ethanol (compounded by a pharmacist) at the proximal nail fold and wait for this liquid to flow by capillary action into the space created by the absent cuticle. Slight elevation of the proximal nail fold with a flat toothpick facilitates penetration. This should be repeated two or three times a day for weeks, until the cuticle is re-formed. The cuticle may never re-form in patients with long-standing inflammation. Fluconazole (200 mg/day) for 1 to 4 weeks may sometimes control chronic inflammation. Short courses of fluconazole may have to be repeated as the infection recurs.
Drug-Induced Paronychia.
The protease inhibitors lamivudine and indinavir, used to treat human immunodeficiency virus (HIV), have been reported to cause paronychia and ingrown toenails in about 4% of patients receiving these drugs. Pyogenic granuloma–like lesions, staphylococcal superinfection, onycholysis, and severe skin dryness may also be present. The nails of the great toes are usually affected. The lesions appear 2 to 12 months after starting treatment. Complete regression of skin manifestations occurs within 9 to 12 weeks after the drugs are withdrawn. Inhibition of endogenous proteases may explain the initial hypertrophy of the nail fold and the subsequent development of pyogenic granuloma–like lesions. Other drugs causing paronychia include: epidermal growth factor inhibitors, cytotoxic chemotherapy agents, and systemic retinoids.
Pseudomonas Infection.
Repeated exposure to soap and water causes maceration of the hyponychium and softening of the nail plate. Separation of the nail plate (onycholysis) exposes a damp, macerated space between the nail plate and the nail bed, which is a fertile site for the growth of Pseudomonas . The nail plate assumes a green-black color ( Figs. 25.15 and 25.16 ). There is little discomfort or inflammation. This presentation may be confused with subungual hematoma (see Fig. 25.32 ), but the absence of pain with Pseudomonas infection establishes the diagnosis. Apply a few drops of a mixture of one part chlorine bleach/four parts water under the nail three times a day. Vinegar (acetic acid) and thymol 4% in alcohol may also be used.


Herpetic Whitlow.
In the past, dentists and nurses were at risk of acquiring herpes simplex virus (HSV) infection of the fingertip. The risk has greatly diminished with the use of gloves. Young adults are typically affected by HSV-2. HSV-1 infection of the hand occurs in children as a result of autoinoculation following herpetic gingivostomatitis. The appearance and course of the disease resemble those at other body sites with grouped vesicles or ulcers on an erythematous base, except that there is extreme pain from the swollen fingertips ( Fig. 25.17 ). Lymphangitis and lymphadenitis, secondary to HSV infection of the hand, are possible complications, particularly with HSV-2 infection. Herpes simplex virus infection in acquired immunodeficiency syndrome (AIDS) patients is characterized by atypical presentations and unusual locations. Herpetic finger infections in these patients may rapidly progress to the complete destruction of nail structures. Viral culture or polymerase chain reaction confirms the diagnosis.

Fungal Nail Infections
Tinea of the nails is also called tinea unguium . The dermatophytes Trichophyton rubrum and Trichophyton mentagrophytes are responsible for most fingernail and toenail infections. Certain nondermatophyte nail pathogens (e.g., Scytalidium dimidiatum and Scytalidium hyalinum ) may also cause infection. Other nondermatophyte nail pathogens (certain species of Acremonium, Alternaria, Aspergillus, Fusarium, Onychocola, and Scopulariopsis ) may cause infection. Candida albicans can occasionally be a pathogen in fingernail disease. Multiple pathogens may be present in a single nail. Nail infection may occur simultaneously with hand or foot tinea or may occur as an isolated phenomenon. Onychomycosis is estimated to affect approximately 2% to 13% of the population of North America and Europe. In older individuals the prevalence is high and likely approaches 60% or more in those older than 70 years.
The disease may also occur in children. Trauma predisposes to infection. There is a tendency to label any process involving the nail plate as a fungal infection, but many other cutaneous diseases can change the structure of the nail. Fifty percent of thick nails are not infected with fungus. Many patients with nail disease have psoriasis and are not infected with fungus. Differential diagnosis is discussed at the end of this section.
Tinea Versus Psoriasis.
Differentiation of fungal infection from dystrophic changes resulting from psoriasis or other causes is difficult. Potassium hydroxide (KOH) preparations, culture, and, occasionally, nail-unit biopsy specimens are used. These tests are time-consuming and may yield false-negative results. Histologic examination of distal nail clipping specimens by routine histology and periodic acid – Schiff (PAS) staining is an accurate and simple method for differentiating onychomycosis from nail psoriasis ( Fig. 25.18 ). It is equal to culture and superior to KOH preparation in leading to the correct diagnosis of dermatophyte infection.

Laboratory Diagnosis.
The diagnosis of fungal nail infection may be established with both a KOH examination and a culture, and occasionally with a nail biopsy. Confirm the species of fungus before starting oral antifungal treatment. When performing cultures, obtain crumbling debris from under several nails and at different parts (proximal and distal areas of infection) of the infected nail ( Fig. 25.19 ). Collect subungual debris from under the distal edge of the nail with a curette. Sample the nail surface with a curette or scrape it with a no. 15 scalpel blade ( Fig. 25.20 ). Fungi are found in the nail plate and in the cornified cells of the nail bed. Hyphae that are present in the nail plate may not be viable; therefore, sample the cornified cells of the nail bed if possible.


Nail Biopsy.
Many clinicians initiate therapy after confirming the presence of hyphae in a nail biopsy specimen. The KOH test is the most cost-effective diagnostic method but a nail biopsy using nail clipping for histologic examination is more sensitive. Submit the nail clipping in the same formalin solution used for skin biopsies. The laboratory will stain sections of the nail with periodic acid–Schiff, which stains fungal hyphae. The fungal species cannot be identified with this method.
Nail Collection Techniques for Culture.
First swab the nail plate with alcohol to remove bacteria. Fragments of nail plate and nail bed scrapings are inoculated onto Sabouraud’s medium with and without antibiotics to identify the fungal species. Use fresh Sabouraud’s with antibiotics. Antibiotics degrade in old media and do not effectively suppress bacterial contaminants. The dermatophyte test medium contains the antibiotic cycloheximide and phenol red as a pH indicator. Dermatophytes release alkaline metabolites that turn the medium from yellow to red in 7 to 14 days. Some nondermatophytes, such as Scopulariopsis, Aspergillus, Penicillium, black molds, and yeast, may cause a color change and give a false-positive reaction. The nail plate and hard debris can be adequately softened for direct examination by leaving the fragments, along with several drops of KOH, in a watch glass covered with a petri dish for 24 hours. (See Chapter 13 on fungal infections for details of the KOH examination.)
Patterns of Infection.
There are four distinct patterns of nail infection. Several patterns of infection may occur simultaneously in the nail plate. T. rubrum and T. mentagrophytes invade the nail plate more frequently than T. violaceum or T. tonsurans. Aspergillus, Cephalosporium, Fusarium, and Scopulariopsis, generally considered contaminants or nonpathogens, have been isolated from infected nails. They may be found in any pattern of nail infection, especially distal subungual onychomycosis and white superficial onychomycosis (WSO). The contaminants do not respond to griseofulvin or the newer oral antifungal agents. The four patterns of nail infection are illustrated in Fig. 25.21 .
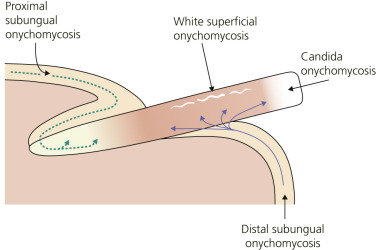
Distal Subungual Onychomycosis.
Distal subungual onychomycosis ( Figs. 25.22 and 25.23 ) is the most common pattern of nail invasion. Fungi invade the hyponychium, the distal area of the nail bed. The distal nail plate turns yellow or white as an accumulation of hyperkeratotic debris causes the nail to rise and separate from the underlying bed. Fungus grows in the substance of the plate, causing it to crumble and fragment. A large mass composed of thick nail plate and underlying debris may cause discomfort with footwear.