(1)
Plastic Aesthetic and Laser Surgery, Hygeia hospital, Athens, Greece
Keywords
Blepharoplasty patient assessmentIntraoperative blepharoplasty complicationsPerioperative complicationsOvercorrectionUndercorrectionIncision qualityResidual fatSkin under resectionPostop instructionsPatient’s compliance6.1 Preoperative Assessment
Preoperative assessment is the cornerstone in preventing complications in blepharoplasty. It should be performed precisely and in all means to completely understand the patients’ desires, clinical history, and psychological status. The orbit and the eyelids are the prominent anatomical regions of the face, the first areas to look at when you communicate to people. Therefore, attention should be paid to avoid all these factors that can lead to an unlucky result, which will make the patient suffer for life.
In the initial assessment, patients are encouraged to express their desires and concerns regarding the aesthetic appearance and functional features of their eyelids. I use to ask my patients to stand in front of a mirror to help them explain what they are bothered from their appearance. If they have difficulty in demonstrating what they would like to be changed in their eyelids and periorbital area, I promote discussion or present alternatives, until clear agreement occurs; otherwise, I avoid surgery with them. It is very important to identify patients’ concerns and realistic expectations before taking a decision for surgery.
Unrealistic expectations of patients may vary a lot. I have consulted patients who in their initial assessment expressed desires for full emptiness of the upper eyelid or absence of eyelid fold, patients with normal lower eyelids who would like correction of skin pigment disorders with a blepharoplasty, operated patients with good postoperative outcome who wish further correction, patients who consider aesthetic surgery as a commodity or lifestyle trend and demand return to their everyday activities next day or the day after surgery, or others who have scheduled events or travels and want their blepharoplasty operation just prior to these activities. Heavy smokers also who deny to limit this habit for a certain period of time before and after operation are prone to prolonged healing process, edema, and bruising, and should be handled accordingly.
However, it is very important for the surgeon to identify which of those unrealistic patients can be educated and convinced for the operation under the specified instructions, and who cannot.
I have found that an approximate proportion of 70% of unrealistic patients are finally convinced to my instructions and postoperative course, proceeding to surgery in full confidence, compared to the 30%, who deny compliance, and I decide to avoid surgery with them.
Once patient’s concerns and realistic expectations are identified and agreed, a full clinical history and examination of the eyes and eyelids should follow.
The clinical history should investigate underlying hypertension, diabetes, coagulation disorders, keloid or hypertrophic formation, allergies, cardiac, or thyroid problems. Medication treatments are also an important issue to be clarified. Patients taking aspirin or other anticoagulants should discontinue use for 5–10 days. The use of carbon dioxide laser dramatically reduces the risk of intraoperative bleeding, and I have operated patients under such treatments who stopped the use for 3–5 days preoperatively with no increased incidence of bleeding. Patients who are in administration of vitamin E, hormones, contraceptives, or herbal medications should stop them, if possible, up to 2 weeks preoperatively, as in some of them who disclosed these treatments after surgery, I have noticed prolonged postop edema formation and increased bruising risk.
Clinical examination should exclude problems with strabismus, orbital, or eyelid asymmetry, difference of palpebral fissure aperture, exophthalmos, concomitant eyelid lesions, brow ptosis and asymmetry, true ptosis, lid retraction, inferior scleral show, lid laxity, dry eye syndrome, conjunctivitis, or allergic diseases of the eye and eyelids. Some of these manifestations such as eyelid asymmetry, different palpebral aperture, and exophthalmos, if existing, may be magnified after blepharoplasty, and patients should be informed (Figs. 6.1, 6.2, 6.3, 6.4, 6.5, and 6.6).





Fig. 6.1
Patient with asymmetric palpebral fissure aperture and lesion located on the ciliary line of the (L) upper eyelid. Blepharoplasty was combined with (L) eyelid lesion wedge excision and (R) lower eyelid traction with SSTT to achieve better symmetry
Fig. 6.2
Patient with prominent bilateral scleral show candidate for SSTT
Fig. 6.3
Patient with asymmetric eyelid fissure aperture due to true ptosis of (R) upper eyelid. This patient had undergone an ENT surgery for an acoustic neuroma, which resulted in a Horner’s syndrome-like complication
Fig. 6.4
Excessive (R) upper eyelid ptosis and mild (L) upper eyelid ptosis with concomitant bilateral sclera show. These cases should mainly aim for the functional upper eyelid height on both sides and the absence of the upper eyelids’ crease
Fig. 6.5
Patient with a postoperative (R) eyelid scleral show, asymmetry of the upper eyelid height, and ptosis due to damage of the (R) upper eyelid levator aponeurosis. Management of complications in such cases needs careful decisions for the timing of the correction pampering of the patients and avoiding early postop corrective surgery, due to their impatience
Fig. 6.6
Preoperative view of patient with upper eyelid asymmetry. Different amounts of skin excision and OOM contraction are required for the achievement of postop symmetry
In decision-making for the technique to be performed, determination of skin and muscle laxity, fat prolapses, wrinkling of lower eyelid, existence of festoons or malar pads, and of course ethnic facial features should be importantly considered. The open or transconjunctival laser technique should also be decided according to the clinical evaluation of the lower eyelid, since in the upper eyelid, the use of laser, as described in previous chapters, is considered as of great value.
Finally, the application of the SSTT for canthal support alone or in combination with improvement of the lower eyelid skin texture and correction of the canthal angle has to be decided.
Following detailed clinical history and preoperative anatomical issues assessment prior to surgery, photographic documentation is required. Photos are taken in face and profile views. I have found that most patients forget their preoperative appearance soon after the first days of surgery. Some of them are coming back in the clinic, with a range of complaints regarding the amount of correction achieved postoperatively. Photographic documentation has proved to be of utmost importance as an “antidote” to these kinds of complaints, together with the preoperative notes and informed consent.
6.2 Intraoperative and Perioperative Complications
It is within the responsibility of the surgeon to inform the patient for the unlikely potential risk of complications, the rate, and the postop management. Many patients are very well “educated” and informed by the wide use of Internet sites and other social media. They visit the office for consultation inquiring information for specific complications and their management. Reassurance and explanation of how these risks can be prevented are very important.
The gravity of a given complication might be different between the patient and the surgeon, and the postoperative management of them can range from reassurance to surgical correction if needed.
The prevention is therefore the very essential step of the procedure.
6.2.1 Minor and Intermediate Complications
Hemorrhage control during surgery
Intraoperative manipulations during surgery are closely related to the early postoperative complications. At this point, I would like to mention that some of these complications should rather been defined as expected side effects rather than real complications (i.e., bruising, edema).
In both upper and lower blepharoplasty, intraoperative care for reduced risk of bleeding with wise and precise use of diathermy for vessel coagulation, at every single surgical step of dissection, or the use of CO2 laser for dissection as described in previous chapters, prevents from postoperative early side effects like bruising. Moreover, gentle manipulation of tissues during surgery reduces excessive trauma and damage together with the risk of prolonged postoperative edema and healing process.
I have found that patients who undergo the procedure under local anesthesia, but with intraoperative i.v. sedation, are less prone to postop bruising and edema. Sedation reduces intraoperative patients’ stress and consequently stress hormones’ release from the adrenal glands. Adrenaline, cortisol, and norepinephrine, the three most important stress hormones, can affect the tissue response during surgery, and sedation significantly contributes in reducing this effect. Similarly, peros administration of bromazepam, diazepam, or lorazepam in patients who do not prefer i.v. sedation can offer analogous effect.
Right after surgery is completed, ice water compresses are applied on the eyelids, and I advise my patients to continue using it for 48 h postop. Ice packs and frozen masks have proved to be quite heavy and increase the risk of injuring the very delicate operated area, so I discourage their use. Small-sized balloons filled with cold water are also very effective and more versatile in postop prevention of bruising and edema onset.
Excessive bruising and ecchymosis can occur in patients who do not comply with the surgeon’s postop instructions. Exercise, raise of blood pressure with workout or other activities, restless sleep, or heavy food and alcohol intake in the first week postoperatively are also significant etiological reasons (Fig. 6.7)

Fig. 6.7
Patient with severe ecchymosis of the lower eyelids and periorbital skin. Chymosis of the conjunctiva is also observed. (L) Upper eyelid incision with dehiscence in the medial aspect. Patient presented in the clinic 8 days postoperatively and disclosed alcohol intake followed by severe vomiting on the fifth postoperative day, right after the suture removal
Overcorrection in upper blepharoplasty
As I have described in Chap. 4, Sect. 4.3.1, the correct marking of the skin prior to surgery is a very important step to prevent aesthetic and functional postoperative complications. The minimum distances of incision from the brow cilia border and the ciliary line (existing upper eyelid crease) have to be strictly followed. This will prevent postoperative lagophthalmos and consequent conjunctivitis or keratitis. Transient lagophthalmos can occur for 24–72 h postop due to a range of edema of the upper eyelid, induced intraoperatively and postoperatively. If observed, patient should be reassured and advised to use the prescribed lubricating and antibiotic eye preparations.
Orbicularis oculi muscle resection in upper blepharoplasty has been substituted by defocused CO2 laser beam contraction, and potential overcorrection is avoided. In cases that resection has been decided, particular attention should be focused to avoid injury of the levator muscle aponeurosis, which lies posteriorly to the inferior part of the preseptal portion of the OOM in the upper eyelid.
Excessive trauma to the levator, levator aponeurosis, or pre-aponeurotic fat pad can result in upper eyelid scleral show, eyelid retraction, and lagophthalmos. Although this complication is very rare, trauma can be induced by cautery overuse at the above areas or excessive laser heat conduction during fat removal. I always use a wet cotton bud behind the prolapsed fat, when removing it, to avoid heat and laser power affect of the underlying structures (Fig. 6.8).
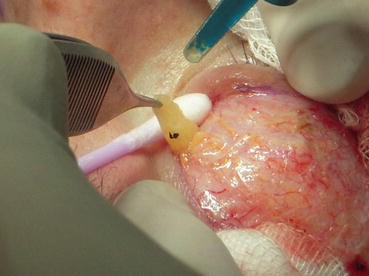
Fig. 6.8
Wet cotton bud used as a backstop right behind the fat before removal with laser
Over resection of fat from the upper eyelid retroseptal fat pads is a very annoying and difficult-to-correct complication for the patients.
I have discussed the concept of heaviness, fullness, and emptiness of the upper eyelid in Sects. 2.1.1, 2.2.1 and 4.3.3. The modern trend of maximum tissue conservation in blepharoplasty should always be considered seriously during surgery and in combined balance with necessary tissue removal. The hollow eye “syndrome” observed in aged patients who had undergone overresection of fat in the upper eyelids in the past should be strictly avoided in modern blepharoplasty, which must aim to fullness but not heaviness of the eyelids as a final outcome (Figs. 6.9 and 6.10)


Fig. 6.9
Heavy upper eyelids with extensive dermochalasis, lateral hooding, and fat prolapse (a) converted to upper eyelids with fullness, defined eyelid crease, and natural look. (b) Patient before and 4 years after surgery. Postoperative picture (b) shows the conservative skin and fat removal which resulted in a very pleasant and natural-looking postoperative outcome
Fig. 6.10
(a, b) Patient operated elsewhere in younger age, presented with upper eyelid hollowness due to excessive fat and skin removal. Lower eyelid scleral show is also present following bilateral retraction of the lower eyelids. Notice the upper eyelid crease unnaturally raised high due to the over-resection of fat, retraction, adhesion, and scarring, involving the eyelid structures and levator aponeurosis. In picture (b), fat transfer to the upper and lower eyelids has restored the fullness and crease formation of the upper eyelid and corrected the scleral show in lower eyelids. Fat transfer to the eyelids is a tricky but very promising procedure, providing surgeons with a very efficient tool for hollowed eyelids correction
My advice, in aiming to prevent and avoid complications as a result of fat over-resection from the upper eyelid fat pads, is to excise fat in small portions, continuously evaluating the residual amount by applying pressure on the eye globe with fingers, prior to each attempt of fat removal. In patients with minimal need of fat resection, controlled vaporization of fat with the CO2 laser-defocused beam prevents from excessive resection.
Finally, under-resection of fat should also be considered as a complication, especially in the medial fat pad of the upper eyelid. Residual amount of fat at this point results in annoying for the patient, postoperative bulging, many of them complaining and seeking surgical intervention for correction. For details, see Sects. 4.3.3 and 4.5 (Fig. 6.11)

Fig. 6.11
Patient with residual fat in the medial fat pad of the upper eyelid following upper blepharoplasty. This patient presented in our clinic complaining for the residual fat and excessive deepening of the upper eyelid crease following blepharoplasty elsewhere. Further minimal fat excision and fat transfer of the upper eyelid were performed to correct the complication
Over correction in lower blepharoplasty
The CO2 laser transconjunctival approach for lower eyelid blepharoplasty with the addition of the OOM posterior surface contraction with laser-defocused beam together with the application of the SSTT, as extensively described in Sect. 4.4.2 and Chap. 5, has dramatically reduced the risk and complication rate of over-resection in the lower eyelid. Moreover, the extended indications of this technique to patients with more excessive skin laxity and wrinkling, which in the past required transcutaneous skin excision, have minimized complications like webbing or rounding of the lateral canthal angle, lower eyelid retraction, scleral show, and ectropion.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


