Mons Pubis Reduction
Michele A. Shermak
DEFINITION
The mons region is defined as a part of the vulvar anatomy, which also includes the labia majora and labia minora.
Monsplasty is performed as an isolated procedure or in conjunction with abdominoplasty and/or medial thighplasty. The goal of monsplasty is to create a smooth mons with attractive dimensions vertically and horizontally and appropriate fat composition, with harmonious continuity with the abdomen.
The mons is often affected by massive weight loss (MWL) and pregnancy, with descent of the pubic area, lengthening of the distance between umbilicus and the vulvar cleft, and residual adiposity.
Although shortening of vertical dimensions and thinning and resuspension of the mons may be performed with abdominal contouring procedures, narrowing horizontal dimension can occur in conjunction with medial thigh lift.
Monsplasty has been shown to improve hygiene, urinary continence, and confidence in sexuality.
ANATOMY
The vulva includes the mons pubis, labia majora, labia minora, vaginal vestibule, and bulb of the vestibule (FIG 1).
The mons pubis is superficial to the pubic bone.
The labia majora are paired cutaneous folds that extend posteriorly from the mons pubis and contain variable fatty tissue. The labia majora converge with the labia minora at the posterior commissure or fourchette.
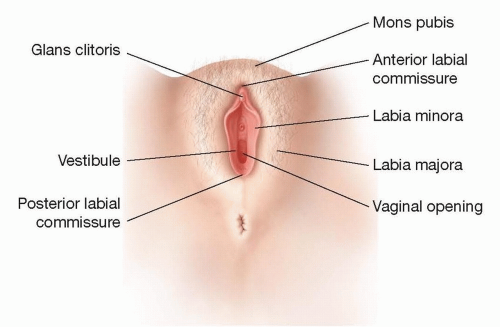
FIG 1 • The female genitalia, with anatomic areas indicated: 1, labia majora; 2, labia minora; 3, mons pubis; 4, clitoral hood; 5, glans clitoris; 6, urethra; 7, vaginal opening.
The labia minora are cutaneous folds located medial to the base of the labia majora. The visible rounded portion of the clitoris is located near the anterior junction of the labia minora, above the openings of the urethra and the vagina.
The vasculature of the female external genitalia includes the anterior labial arteries, branches of the external pudendal arteries, the posterior labial arteries, and branches of the internal pudendal artery. The labial veins drain to the pudendal and femoral veins.
The vulva is innervated anteriorly by the anterior labial nerves and branches of the ilioinguinal nerve and by the genital nerve, which extends from the genitofemoral nerve. The vulva is innervated posteriorly by posterior pudendal branches.
PATHOGENESIS
Mons pubis and labia majora morphology are impacted by aging, pregnancy, and weight changes that in turn impact fat composition, dimensions, and ptosis.
The youthful mons pubis is narrow, with good skin tone, and has a moderate amount of fat in the subcutaneous plane to provide padding against the bony symphysis.
With age, pregnancy, or weight fluctuations, the mons pubis can appear wide and protuberant with poor skin tone (FIG 2). The labia majora may be deflated, and there is ptosis of the external genitalia with increasing distance from the abdomen inferiorly.
With obesity, the mons becomes increasingly protuberant with a relatively high composition of fat, which often lends itself to surgical correction with liposuction alone. Difficulty with sexual intercourse and maintenance of hygiene as well as discomfort when wearing pants and swimsuits may result. This situation can also impact self-esteem.
Techniques to correct the protuberant mons and pubic descent with excess skin address these issues with pubic lifting, fat excision and liposuction, and/or elevation and suspension of the fatty layers to the rectus abdominis fascia.
PATIENT HISTORY AND PHYSICAL FINDINGS
The surgical consultation should begin with discussion of patient concerns and desired outcomes. Discomfort or dissatisfaction with sexual intercourse, bladder control, problems with exercise or wearing certain clothing, and hygienic concerns could result in a patient initiating a surgical consultation.
Medical history should be explored for any medical conditions and history of weight gain or loss and pregnancies, as well as surgical history.
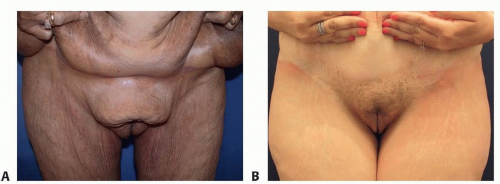
FIG 2 • A. Mons pubis in MWL demonstrates significant ptosis and excess fat. B. Abdominoplasty with removal of the upper part of the mons pubis will allow a rejuvenated appearance.
Physical examination is comprehensive and involves the abdomen as well as the external genitalia.
A surgical plan is then developed to address patient desires and goals, as well as physical findings, adjusting treatment to health and safety concerns.
IMAGING
This is not applicable to monsplasty management.
SURGICAL MANAGEMENT
Preoperative Planning
After history and physical examination, planning for monsplasty takes place. Considerations for the pubic region include fat composition and skin quality and excess, as well as height and width dimensions. In most abdominal contouring procedures, the mons pubis is treated with the abdomen with liposuction.
With varying degrees of mons distortion beyond excess fatty tissue, excisional procedures including horizontal and vertical wedge excision with or without abdominal or thigh contouring are necessary.
Horizontal excision shortens vertical distance and may be performed in continuity with abdominoplasty, allowing 6 to 7 cm of distance between the vulvar cleft and the lower abdominal skin incision.
Vertical excisions of the mons and labia majora as a central ellipse or as lateral wedges may be included in medial thighplasty to narrow the mons pubis, by restoring a more youthful triangular configuration.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree








