Mohs Micrographic Surgery: Introduction
|
Background
Mohs micrographic surgery (MMS) is a surgical technique developed to excise skin cancer under complete microscopic control. The fresh frozen tissue technique is used, which permits immediate examination of the specimen, and the tissue is oriented in a way to permit evaluation of all surgical margins. This is distinct from the traditional bread loafing technique used to process tissue specimens. A special orientation is combined with a precise mapping technique, which leads to maximal conservation of normal tissue. The technique was developed by Dr. Frederick Mohs approximately 80 years ago using a fixed tissue technique that relied on zinc chloride paste. The original term, chemosurgery refers to the use of the tissue fixative which is no longer used. As a result, the term chemosurgery is considered archaic.1 MMS has been described by various names such as chemosurgery, microscopically controlled excision, and microscopically oriented histographic surgery. The latter is an attempt at creating an acronym to replace the eponymous term Mohs.
In the past several decades, the mapping component has been retained but the procedure has been refined using frozen tissue rather than fixed tissue, which has permitted more efficient patient care. The advantages of MMS over conventional excisional surgery include maximum cure rate and optimal preservation of healthy tissue. The latter serves to enhance cosmetic outcome and preserve function where applicable. MMS is now recognized as the standard of care for the treatment of various skin cancers in indicated circumstances. The most common cancers treated by this method are basal cell carcinoma (BCC, 73%) and squamous cell carcinoma (SCC, 23%).2 A defining characteristic of MMS is that the surgeon acts to interpret the histopathologic specimens. Specifically, the MMS procedure requires a single physician to act in two integrated but separate distinct capacities as surgeon and pathologist. MMS is a highly technical procedure that requires meticulous attention to detail and considerable training and experience to achieve the expected high cure rates.
The Procedure
Mohs surgery is performed under local anesthesia in the office setting or in an ambulatory center. In unusual cases, where multiple cancers or complex malignancies are to be removed, sedation may be used.3 Prior to surgery, it is essential to have the patient affirmatively identify the biopsy site as very often the biopsy site may fade due to postbiopsy healing. It has been shown that in 25% of patients, who had prior biopsy, no remnants of tumor were found during MMS. 4 This is consistent with the fact that the inflammatory process may contribute to elimination of residual cancer cells after biopsy. The fundamental elements of MMS are listed in Table 244-1. A complete medical history and list of medications should be documented before surgery is performed. Anticoagulants are not contraindicated and data have shown that they should not be discontinued prior to MMS. 5 Once the patient is properly positioned, it is important to mark the clinical tumor border with a surgical pen. Local anesthesia is then obtained by injection (Fig. 244-1). Marking the clinical borders of the tumor is necessary since the local anesthetic may cause blanching that can obscure the tumor borders. The most commonly used local anesthetic is 1% or 2% lidocaine with 1:100,000–200,000 epinephrine (Fig. 244-2). After the surgical site is gently curetted to determine the clinical extent of the cancer, a specimen is taken using the Mohs technique. (Fig. 244-3). This is considered the first Mohs stage. A thin layer of tissue is excised using a scalpel and incising the skin at a 45° angle. Nicks are made in the surrounding tissue to denote tissue orientation and mapping (Fig. 244-4). In some cases, double nicks can help in the orientation of the tissue.6 Mapping of the tissue is a crucial step in MMS. The topographic map allows the Mohs surgeon to relate the microscopic findings to the excised tissue and the anatomic reference points at the surgical site (Fig. 244-5) The Mohs map is typically created by drawing freehand, using a template or digitally using computerized software (Fig. 244-6). The tissue is brought to the adjacent laboratory (another key element of the Mohs technique is the presence of a contiguous lab under the supervision of the Mohs surgeon). Color coding of specimens is critical. The Mohs technician or the surgeon marks the borders of the tissue with different colors to allow orientation relative to the Mohs map. Usually two dyes are used such as red and black or black and yellow (Fig. 244-7). One of the dyes is represented on the map as a solid line and the other as a dotted line. The tissue is then processed by a technician who is specifically trained in the en face method of sectioning. The tissue is frozen and is cut horizontally on a microtome. In contrast to traditional paraffin sections, which are cut vertically (bread-loaf sections) the Mohs sections theoretically allows 100% of the tumor margins (depth and periphery) to be examined. Most Mohs surgeons use hematoxylin-eosin stain (83%) and a minority use toluidine blue as the preferred stain. The latter stain helps distinguish basal cell carcinoma from hair follicles by highlighting mucopolysaccharides in the stroma.7 In between the Mohs stages, the wound is dressed temporarily and the patient waits either in the procedure room or in a dedicated waiting room. Slide preparation takes 20–30 minutes on average. Examination of the slides by the surgeon is then performed in the laboratory. Residual cancer noted microscopically is marked on the Mohs map and the process of excision, mapping, and processing is repeated until all margins are free of tumor (Figs. 244-8, 244-9). High quality frozen sections are mandatory for the success of MMS8 Figs. 244-10 and 244-11 illustrate how the Mohs technique ensures complete tumor removal. Once MMS is complete, the wound is evaluated and reconstruction is either performed at that time by the Mohs surgeon or the wound is allowed to heal by second intention. In complex cases, collaboration with other reconstructive surgeons may be indicated. Reconstructive surgery has become an important and integral aspect of the care of the skin cancer patient. The original chemosurgery defects healed by second intention, but the current defects that result from the fresh tissue technique permit primary closures, adjacent tissue transfer, and grafts. As a result, parallel advances in reconstructive surgery have been significant in the evolution of MMS.
Injection of local anesthesia Curettage to determine gross clinical margins Excision of the first layer with the scalpel beveled at 45° (first MMS stage) Color coding and mapping of the tissue Horizontally cut frozen sections Tissue staining Microscopic examination of the tissue by the surgeon Repetition of the tumor excision cycle until cancer is removed Reconstruction |
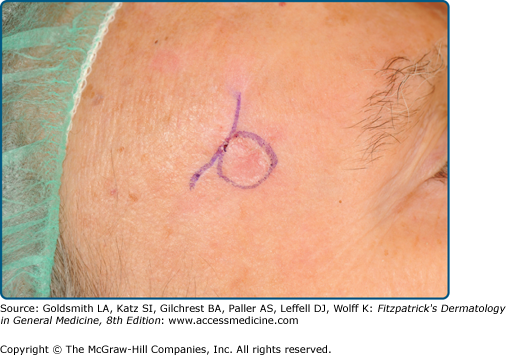
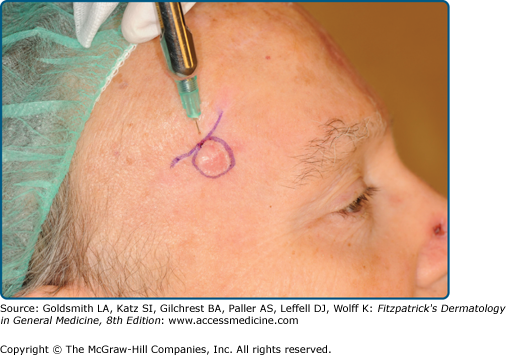
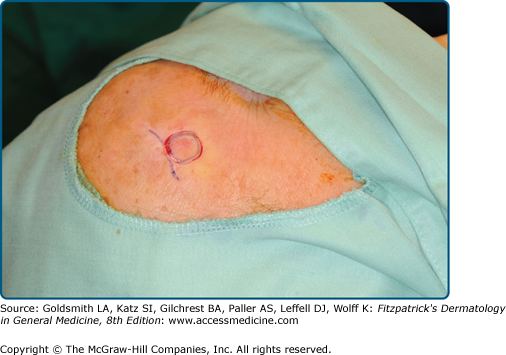


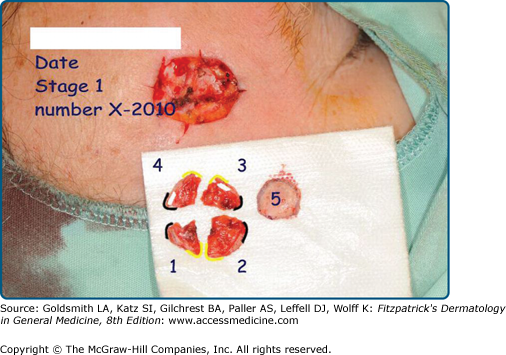
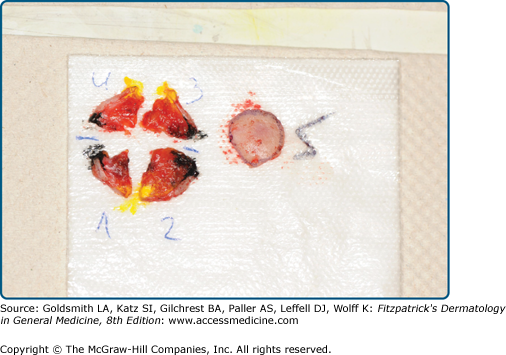
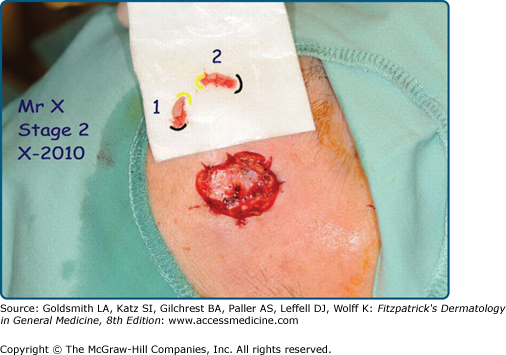

Figure 244-10
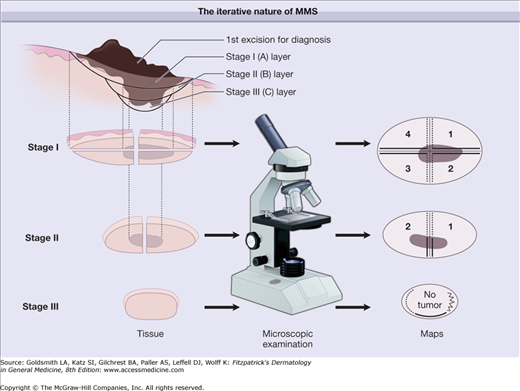
This schematic illustrates how the Mohs technique assures complete tumor removal. Obvious cancer (black) is obtained to determine subtype (upper left). Cancer discovered by microscopic examination is outlined by dots in each layer. In Stage I, a layer was removed and divided into four specimens (as viewed from the bottom); after microscopic examination, residual tumor was found only in the central area of all four specimens. In Stage II, a central layer was excised and bisected; after microscopic examination, residual tumor was found only in the center of specimens 1 and 2. In Stage III, another small block specimen was removed; after microscopic examination no residual tumor was found. In this case, the Mohs procedure consisted of three stages of excision and the microscopic examination of seven specimens. (From Mohs Micrographic Surgery, 2nd ed., edited by SN Snow and GR Mikhail 2004. The university of Wisconsin Press, with permission.)
Figure 244-11
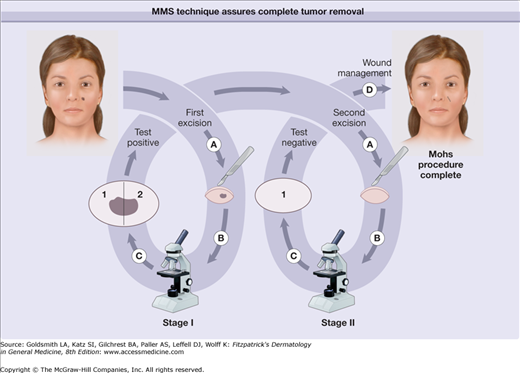
This schematic illustrates the cyclic nature of Mohs surgery. The four main components are the excision of a disc of tissue (a), microscopic examination (b), the appropriate marking of the map when residual cancer is found (c), and wound management (d). In Stage A, the tumor was removed, examined with the microscope. Residual tumor (black) was found throughout specimens 1 and 2. In Stage B, a deeper layer was removed and examined microscopically. In the second layer, no remaining cancer could be found. The defect was then allowed to heal by second intention. (From Mohs Micrographic Surgery, 2nd ed., edited by SN Snow and GR Mikhail 2004. The university of Wisconsin Press, with permission.)









