21 Modern Concepts of Prosthetic Rehabilitation in Amputation of the Lower Extremity
Summary
Targeted muscle reinnervation offers a proven method for the treatment of amputation-related pain in lower limb amputees. It is recommended for any patient suffering from painful terminal neuromas and/or phantom limb pain and has also shown good effects in preventing these conditions, when performed during the amputation procedure. Targeted sensory reinnervation may provide a similar approach for purely sensory nerves with the additional benefit of improved sensory feedback at the stump.
Keywords: neuromas, phantom pain, amputation-related pain, targeted muscle reinnervation
21.1 Introduction to Targeted Muscle and Sensory Reinnervation
The majority of lower limb amputees suffer from some type of amputation-related pain.1,2 Generally, these painful sensations may include neuroma and/or phantom limb pain, which are both related to loss of continuity of the affected extremity nerves.3 After a peripheral nerve loses its physiological target through trauma or surgery, its axons regrow at the nerve stump. If they do not find a target to innervate, they sprout in an unguided manner, leading to the formation of a terminal neuroma.1,4 When sensory fibers are included, these neuromas are generally painful upon external stimuli such as increased pressure. Located at an area of weight bearing, stump neuromas frequently inflict pain upon loading and thereby prevent the use of a prosthetic device. Phantom limb pain, in contrast, is not directly associated with mechanical stimuli at the stump. It affects up to 80% of amputees and entails painful sensation of the missing parts of the limb. It usually appears as intermittent background pain, with intervals that range from 1 day to several weeks and some additional short exacerbations.5 The underlying pathomechanisms of phantom limb pain are not well understood. While there are different theories about its origin, there is an agreement that various peripheral and central factors along the neuraxis are at play.6 Furthermore, external factors such as emotional stress or psychiatric disorders might also contribute to an increase in pain.7,8,9
Both stump neuromas and phantom limb pain do not respond well to standard pain medication. While as first-line medication the use of paracetamol and nonsteroidal anti-inflammatory drugs (NSAIDs) is recommended before other pharmacologic agents, there is still limited evidence on the effect of these.10,11 Regarding stump neuromas, over 150 surgical treatment methods4 have been described and traditionally the best, although still limited, results have been achieved by shortening of the nerve and transposition into muscle tissue. Phantom limb pain treatment has generally been conducted in a multimodal manner, including pharmacological interventions, behavioral approaches, physical and occupational therapy, surgical approaches such as sympathectomy, aimed at lesioning certain neural pathways, and neurostimulation. Several studies have shown that most of these treatments are ineffective, often not exceeding the placebo effect.6,12 Other studies showing positive effects of treatment approaches lack the methodological rigor and robust reporting needed to confirm effectiveness.13
Targeted muscle reinnervation (TMR) was first introduced in 2004 by Kuiken et al as a technique for improved prosthesis control in upper limb amputees.14 The main concept is the transferal of blindly ending nerves onto the motor nerves of remaining muscles in the stump, thereby creating novel neuromuscular units. While the primary emphasis of this technique was to create an increased number of intuitive myosignals for upper limb amputees in order to facilitate improved prosthetic control, it has also shown to be effective in the treatment of amputation-related pain. It also prevents neuroma formation by offering the nerves new terminal receptors. While it may be argued that muscles only provide a target for motor fibers, experience has shown that sensory fibers also regrow into the skin overlying the reinnervated muscles after TMR.15 This “reafferentiation” of a peripheral target to the central nervous system, that is, the recreation of a complete and functional neuraxis, is believed to be a driving factor behind the positive effects of TMR on phantom limb pain.
In the first randomized clinical trial on surgical treatment of amputation-related pain, TMR has shown better outcomes for phantom limb pain and neuroma-related residual limb pain compared with conventional neurectomy, that is, shortening of the nerve.16 More recently, it has also been explored as a preventive treatment performed during amputation, showing similarly encouraging results.17,18
Targeted sensory reinnervation (TSR) applies the same concept to the reinnervation of sensory nerves. While theoretically providing the same benefits as TMR with regard to pain management, it offers the additional benefit of creating specialized sensation at the stump of lower limb amputees. For example, after transfer of the sensory tibial nerve onto the sural/saphenous nerve, a transtibial amputee will feel their planta pedis at the stump.19 This can be employed with the idea in mind to create more natural gait feedback for the amputee.20 It is hypothesized that such an approach to create meaningful and intuitive feedback can help improve postural stability and embodiment of the device, while reducing falls.19 However, not much work has been done on this topic and its feasibility is yet to be investigated.
21.1.1 Indications and Contraindications
TMR should be considered for any patient with lower extremity amputation, suffering from either phantom limb or neuroma pain. In light of recent research, it is recommended to perform TMR already during the amputation procedure, thereby effectively preventing neuroma formation and acting against phantom limb pain after successful muscle reinnervation.17,18 There are no specific contraindications for this procedure. In the cases where there is no viable musculature left at the stump or soft-tissue coverage at the weight-bearing area is insufficient, which may happen in certain avulsion traumas, a free muscle transfer may be used as target for nerve transfers.
21.1.2 Preoperative Management
In the case of terminal neuromas at the stump, these can in most cases be located in clinical examination by elicitation of a Tinel–Hoffmann sign. In addition, high-resolution ultrasound can be helpful to determine the exact location and type of neuroma, and ultrasound-guided nerve block may be used to secure the diagnosis. Phantom limb pain, on the other hand, is a purely clinical diagnosis, associated with painful sensations at missing parts of the limb. The availability of sufficient stump muscles for TMR may be assessed clinically. In the cases where there is doubt about the condition of stump musculature, high-resolution ultrasound and MRI may prove helpful and surface or needle electromyogram (EMG) is recommended to test muscular activity.21
21.1.3 Technique
The patient is placed in a prone or lateral position. In above-knee amputees, the main nerves of the thigh are exposed via a longitudinal dorsal incision. In below-knee amputees, the incision crosses the knee joint in a Z-fashion, continuing laterally along the course of the peroneal nerve.
As an example, we report the case of a 17-year-old adolescent boy who lost his lower limb at the below-knee level in a traumatic accident with a boats’ propeller. Prosthetic fitting was not successful, as the patient developed chronic ulcerations at the scarred distal stump end as well as painful neuromas. To save the below-knee level of amputation and improve the soft-tissue quality, a free musculocutaneous latissimus dorsi flap was performed. In this case, the deep peroneal nerve was coapted to the thoracodorsal nerve of the latissimus flap, and the distal tibial nerve was coapted to the nerve branches of the gastrocnemius heads. With this complex procedure, painless weight bearing at the distal stump end and therefore excellent prosthetic use could be achieved (▶ Fig. 21.1, ▶ Fig. 21.2, ▶ Fig. 21.3).
The nerve transfers used in the treatment of neuroma and phantom limb pain should be chosen based on clinical examination (location of neuromas) and available anatomy. The donor nerves have to be neurotomized at least to a level of palpable healthy fascicles. Nerve transfers can be performed under loupe magnification in an end-to-end fashion using 8–0 or 9–0 nylon sutures and fibrin glue.
21.1.4 Postoperative Management
Depending on the exact site of nerve coaptation, successful reinnervation of the target muscles may take 3 to 6 months. If there is neuropathic pain during this period, this can be managed with specific analgesics such as pregabalin. Neuropathic and phantom limb pain should subside once the nerves have reached the targets. After reinnervation, selective activation and training of the newly innervated stump muscles can be helpful if phantom limb pain persists. This is done with the aim to effectively strengthen the cortical representation of the lost limb and may be guided by surface EMG biofeedback or approaches for sensory training.21,22

Fig. 21.1 Chronic ulcerations at the scarred stump end.
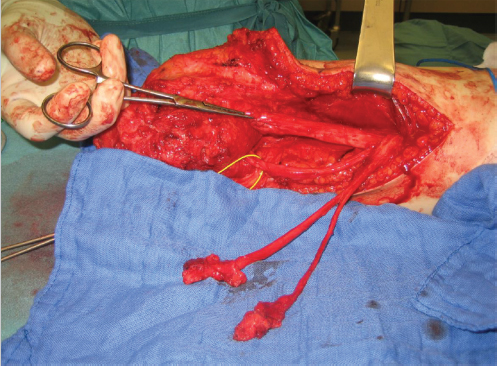
Fig. 21.2 Dissected neuromas.

Fig. 21.3 Stump 6 months after soft-tissue correction with free latissimus dorsi flap.
Related posts:
 General Wound Preparation and Timing
General Wound Preparation and Timing
 The Pertinence of the Reconstructive Ladder and the Reconstructive Elevator
The Pertinence of the Reconstructive Ladder and the Reconstructive Elevator
 Supermicrosurgery Approach to the Lower Limb
Supermicrosurgery Approach to the Lower Limb
 Lower Limb Vascularized Composite Allotransplantation
Lower Limb Vascularized Composite Allotransplantation
 Using the Flap and Angiosome Concepts to Optimize Functional Lower Leg and Foot Amputations
Using the Flap and Angiosome Concepts to Optimize Functional Lower Leg and Foot Amputations
 Procurement of Thin Flaps as Indicated in the Lower Extremity
Procurement of Thin Flaps as Indicated in the Lower Extremity
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


