POSITIONING OF THE SURGICAL TEAM
■ Operation is performed by four surgeons: The first surgeon is on the right side of the table, the first assistant is on the left side of the table. The second assistant, who is holding the retractors, is at the head of the table. The third assistant, who is holding the endoscope, is on the left side of the table.The scrub nurse is behind the surgeon on the right side of the table (FIG 2).
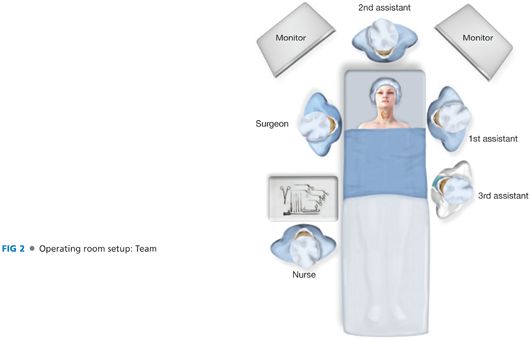
■ The surgeon is on the right side of the table.
■ The first assistant is on the left side of the table (opposite the surgeon).
■ The second assistant is at the head of the table.
■ The third assistant is on the left side of the table.
■ The scrub nurse is behind the surgeon on the right side of the table.
INSTRUMENTATION
■ Forward-oblique telescope 30 degrees, diameter 5 mm, length 30 cm; suction dissector with cutoff hole, with stylet, blunt, length 21 cm; ear forceps, very thin, serrated, working length 12.5 cm; conventional tissue retractor army navy type; small tissue retractor, double-ended, length 12 cm; clip applier for vascular clips; straight scissors, length 12.5 cm, Harmonic Scalpel CS14; electrocautery (monopolar) (FIG 3).

INCISION AND PREPARATION OF THE OPERATIVE SPACE
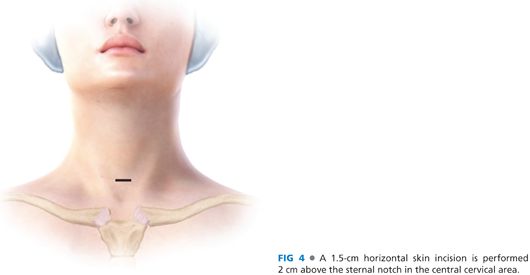
■ A 1.5-cm horizontal skin incision is performed 2 cm above the sternal notch in the central cervical area (FIG 4). Subcutaneous fat and platysma are carefully dissected so as to avoid any minimum bleeding.
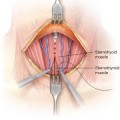
■ Two small retractors are used to expose the midline, which has to be incised for 2 to 3 cm in an absolutely bloodless plane (FIG 5).

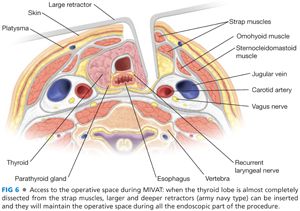
■ The blunt dissection of the thyroid lobe from the strap muscles is performed through the skin incision by gentle retraction and using tiny spatulas. When the thyroid lobe is almost completely dissected from the strap muscles, larger and deeper retractors (army navy type) can be inserted and they will maintain the operative space during all the endoscopic part of the procedure (FIG 6).
■ Then, a 30-degree, 5-mm or 7-mm endoscope is introduced through the skin incision: From this moment on, the procedure is entirely endoscopic until the extraction of the lobe of the gland. Preparation of the thyrotracheal groove is completed under endoscopic vision by using small (2 mm in diameter) instruments such as spatulas, forceps, spatula-sucker, and scissors.
SECTION OF THE MAIN THYROID VESSELS
■ The first vessel to be ligated is the middle vein, when present, or the small veins between jugular vein and thyroid capsule. This step allows a better preparation of the thyrotracheal groove where the recurrent nerve will be later searched.
■ During this step, the endoscope has to be held inside the camera with the 30-degree tip looking downward and in an orthogonal axis with the thyroid lobe and trachea.
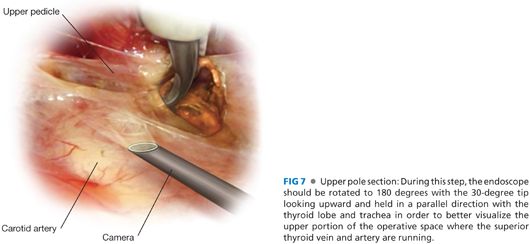
■ A further step is represented by the exposure of the upper pedicle, which must be carefully prepared, until an optimal visualization of the different branches is achieved. During this step, the endoscope should be rotated to 180 degrees with the 30-degree tip looking upward (FIG 7) and held in a parallel direction with the thyroid lobe and trachea in order to better visualize the upper portion of the operative space where the superior thyroid vein and artery are running.
■
Related posts:
 Thyroidectomy for Substernal Goiters
Thyroidectomy for Substernal Goiters
 Inguinal Lymph Node Dissection (Inguinofemoral and Ilioinguinal) for Metastatic Melanoma
Inguinal Lymph Node Dissection (Inguinofemoral and Ilioinguinal) for Metastatic Melanoma
 Thyroid Lobectomy
Thyroid Lobectomy
 Pedicled Transverse Rectus Abdominis Myocutaneous Flap Breast Reconstruction
Pedicled Transverse Rectus Abdominis Myocutaneous Flap Breast Reconstruction
 Open Neck Exploration for Primary Hyperparathyroidism
Open Neck Exploration for Primary Hyperparathyroidism
 Subtotal Parathyroidectomy or Total with Autologous Graft
Subtotal Parathyroidectomy or Total with Autologous Graft
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


