9 Midface reconstruction
Synopsis
Reconstructive goals of midface defects:










Introduction
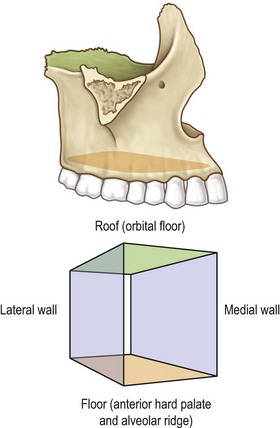
Reconstruction of the midface is best approached through a clear understanding of the complex three-dimensional anatomy of the maxilla.1 In the most basic terms, the maxilla may be thought of as a six-walled geometric box that includes the roof, which is made up by the orbital floor; the floor of the box, which is made up by each half of the anterior hard palate and alveolar ridge; and the medial wall of the box, which form the lateral walls of the nasal passage (Fig. 9.1). The maxillary antrum is contained within the central portion of the maxilla. The cranial base overlies the posterior pterygoid region of the maxilla. The two horizontal and three vertical buttresses produce facial width, height, and projection. The overlying soft tissues, including the muscles of facial expression and mastication, insert on the maxilla and are responsible for individual facial appearance and function.
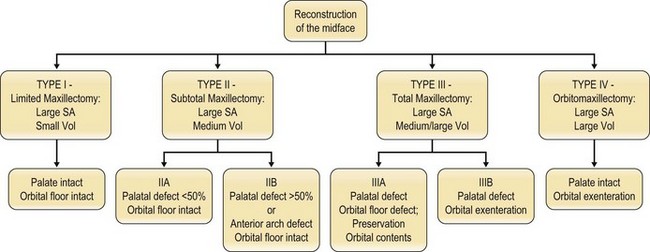
The goals of reconstruction are functional and aesthetic. Most extensive midface defects require free flaps for reconstruction, with the flap selection dependent on the amount of resected skin, soft tissue, and bone.2–7 Small volume defects can be reconstructed with radial forearm fasciocutaneous or osseocutaneous flaps.5,8 Large volume defects can be filled by a rectus abdominis myocutaneous flap.7,9 Currently, complex structures such as lips, eyelids, and the nose should be reconstructed separately, usually with local flaps, without incorporating free tissue transfer.10–14 By following an algorithm based on a clearly delineated classification system of midfacial defects, even patients with very large, complex defects can be restored to good function (Fig. 9.2).1,15
Diagnosis/patient presentation
Type I: limited maxillectomy defects
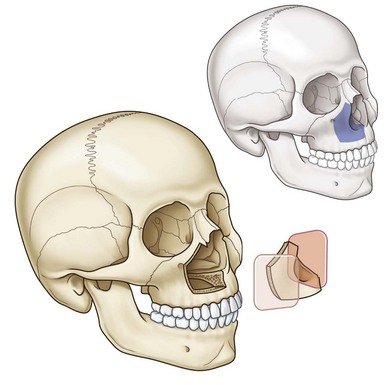
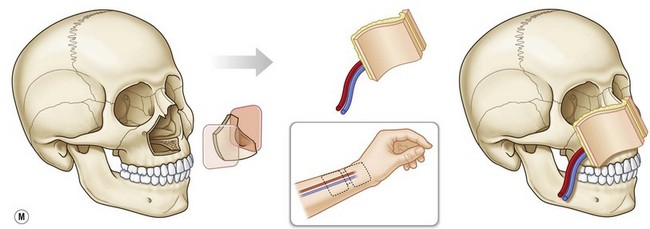
Type I, or partial, maxillectomy defects are those that involve one or two walls of the maxilla, most commonly the anterior and medial walls (Fig. 9.3). Both the palate and the orbital floor are intact. The resection will often include the soft tissue and skin of the cheek, and even the lips, nose, and eyelids. Occasionally, the orbital rim will be resected and non-vascularized bone grafts will be necessary for reconstruction. Type I maxillectomy defects are small-volume deficiencies with large surface area requirements, often needing one or two skin islands. Our flap of choice is the radial forearm free flap, as it provides good external skin coverage and minimal bulk while allowing multiple skin islands that can be de-epithelialized to improve contour, wrap around bone grafts, and supply lining for the nasal cavity (Fig. 9.4).