Key Words
microtia, aural atresia, auricular reconstruction, ear reconstruction, ear deformities, auricular deformities, rib cartilage framework, Medpor, auricular prostheses, Nagata, Firmin, Brent
Synopsis
Microtia literally means “small ear” but is used in reference to a spectrum of auricular deformities that almost always occur in association with aural atresia (absence of an external auditory canal). From a practical point of view, any congenital deformity of the auricle that requires insertion of a complete or near-complete framework is an example of microtia. Microtia has been classified in various ways, but the most useful is the classification of Nagata: lobular microtia, small concha microtia, and large concha microtia. Complete anotia is almost never seen. Because microtia usually occurs with aural atresia, the patients have a total conductive hearing loss on the affected side. 10% of microtia is bilateral, and those patients are functionally deaf and require a bone conduction aid to have sufficient hearing to develop normal speech. Auricular reconstruction in patients with microtia can be performed in one of three ways: rib cartilage framework with cutaneous coverage (all autogenous), an alloplastic framework with cutaneous and fascial/skin graft coverage (partially alloplastic and partially autogenous), or a prosthesis (totally artificial). This chapter will deal primarily with autogenous reconstruction but will make reference to the other methods. Auricular reconstruction using autogenous tissues can be applied to post-traumatic and post-ablative deformities as well. The procedure usually is performed in two stages: placement of a rib cartilage framework and, after a period of approximately 6 months, elevation of the framework and construction of a retroauricular sulcus. The most significant complications of auricular reconstruction for microtia are related to: 1. Errors in judgment regarding size, position, orientation, or incisions; 2. Poor framework design; and 3. Necrosis of cutaneous coverage with exposure of the underlying cartilage framework.
Clinical Problem
Presentations and Etiologies
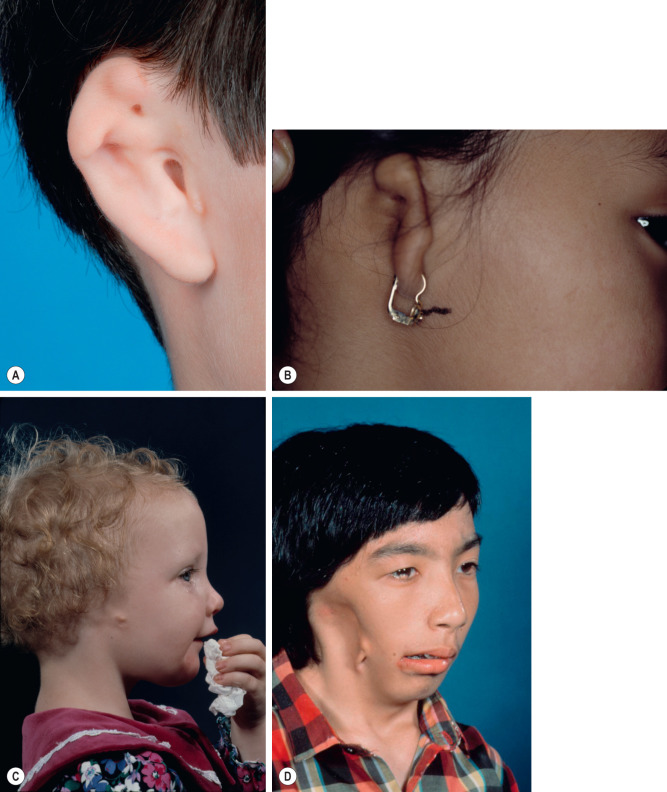
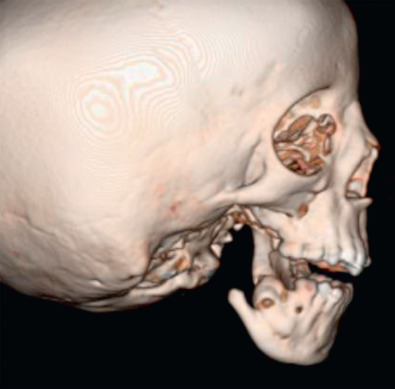
Microtia represents a wide spectrum ( Fig. 3.9.1 ). Microtia is more common on the right side and is unilateral in approximately 90% of cases. There is usually no external auditory canal ( Fig. 3.9.2 ) and also variable anomalies of the middle ear ossicles causing a total conductive hearing loss on the affected side. The inner ear is usually normal. Microtia is the second most common congenital deformity affecting the head and neck (after cleft lip and palate) and is more common in patients of Southeast Asian descent.
Associated Conditions
While the presentation of microtia is highly variable, microtia itself is a component of a larger clinical entity: hemifacial microsomia (HFM). HFM is a clinical entity involving underdevelopment on one side of the face. The auricle, facial nerve, soft tissue, and the skeleton can be involved. Most cases of microtia occur on faces that are near-symmetrical, but close examination and radiographic examination almost always show some asymmetry, indicating that even “isolated microtia” cases are part of the HFM spectrum. Approximately 10% of microtia cases, however, occur in patients with obvious facial asymmetry, which can sometimes be severe (see Fig. 3.9.1 ). A unilateral auricular deformity in a patient with a near-symmetrical face is totally different from a bilateral case (deafness requiring hearing aid) or severe HFM (where the missing auricle may be the least apparent aspect of the deformity).
Pre-operative Management
The ideal age to perform reconstruction of a missing auricle is age 10. At this age, the contralateral ear has reached adult size, and the rib cartilages are large enough to create an adult-size ear framework. In a patient who is small for his/her age, waiting beyond age 10 until the patient is approximately the size of an average 10 year old is recommended.
Before age 10, the focus of patient management is on the hearing. As mentioned, a patient with unilateral microtia has a total conductive hearing loss on the affected side but normal hearing in the unaffected ear. These patients can hear normally in quiet environments, but the lack of binaural input causes difficulty in localizing sound and in discriminating sounds in noisy environments. For example, a unilateral patient will have difficulty playing football when his/her name is yelled. The patient may have trouble determining immediately the direction of the sound and may look in the incorrect direction initially. In addition, in a room with multiple voices, it is more difficult for a microtia patient to screen out the background noise to focus on a conversation. These patients benefit from a bone-anchored hearing aid (BAHA) ( Fig. 3.9.3 ). Patients with bilateral microtia, on the other hand, absolutely require conduction aids because they are functionally deaf and will not develop normal speech without appropriate aids.

Hearing can be restored either surgically or by use of a BAHA. Reconstruction of the external auditory canal and ossicles can be surgically performed in approximately half the cases of aural atresia. In the other 50% of cases, the anatomy is too deranged for surgical repair. BAHAs are so effective, however, and so much less prone to complications compared with canalplasty, that BAHAs are more commonly employed than surgical reconstruction of the canal ( Fig. 3.9.4 ).










