Fig. 2.1
The incision direction and the cleavage lines. (a) Langer’s lines in the facial skin. (b) The directions of the facial wrinkles
- 2.
If the incision must pass across the expression lines during the surgery, it is necessary to change direction to make the incision go along the zigzag direction or S direction, when the incisions in the limbs need to pass across the joints, and the incisions should be made as horizontal shaped or S shaped to prevent linear contracture.
- 3.
The facial incisions can be made along the dividing lines between the contour lines and regions, such as the hidden areas beside the nose, beside the nosewing, in front of the auricle, and in hairline margin and mandibular margin.
- 4.
The incisions should be made using a sharp knife, and all layers of the skin should be vertically cut through at a time, avoiding being repeatedly cut to result in an irregular incision line. The beveled incision should be prevented; otherwise an uplifted scar will appear on one side of the incision after suturing.
2.2 Dissection
The sharp dissection should be mainly performed during surgery, which is combined with blunt dissection. Close attention should be paid to the dissection plane to reduce tissue damage and bleeding.
2.3 Hemostasis
The thorough hemostasis is a basic requirement of the surgery, and the plastic surgery requires both thorough hemostasis and slight injury:
- 1.
The electric coagulation hemostasis can still be used during deep surgery and large flap transfer, but, in order to reduce tissue damage, we recommend using bipolar coagulation or mini electric coagulation to reduce the range of tissue charring.
- 2.
The compression hemostasis with warmly wet saline gauzes can be used for wounds with more extensive bleeding.
- 3.
The local application of epinephrine solution has a temporary hemostatic effect but leads to a higher incidence of secondary bleeding and the hematoma under the skin graft and the skin flap; therefore, the operators had better not use this method.
- 4.
The ligation hemostasis is a commonly used method with most definite efficacy. In order to ensure a smooth suture without tearing the line off, it is recommended to learn and master the method of two-hand tying to tie three knots.
- 5.
The hemostasis method such as suture ligation can be used in places where it is difficult to carry out hemostasis.
- 6.
The appropriate application of the inflatable and rubber sheet esmarch tourniquets can reduce blood loss during the lower extremity surgery.
2.4 Washing
The plastic surgeries often have a large wound and long operative time, and it is appropriate to wash the wound during surgery and before suturing to remove tissue debris and prevent infection, which is conducive to tissue repair. The clean wound is washed with normal saline, and the contaminated wound is washed repeatedly with 1:2000 benzalkonium bromide (bromogeramine), 1.5% hydrogen peroxide solution, and normal saline.
2.5 Drainage
The extensive dissected wounds often cause postoperative hematoma, effusion, or infection due to the oozing of the blood and the imperfect hemostasis; therefore, the drainage after such surgery is often a necessary measure. The drainage methods include rubber sheet drainage, half-flat catheter drainage, cigarette drainage, and negative pressure drainage, which are selectively used according to the different conditions. The drainage is removed usually at 48–72 h after surgery, and the negative pressure drainage can be prolonged up to 3–4 days after surgery and then will be removed.
2.6 Suture
The ideal suture in plastic surgery should be the layered suture, which requires the exact alignment, moderate degree of tightness, no dead space in deep layer, and no tension in skin layer. The wound should be carefully sutured on the basis of thorough hemostasis. It should be avoided to use the large needle and thick line; the layer dislocation should be prevented; and the wound should be sutured layer by layer from deep layer to shallow layer. The commonly used suture methods include skin and subcutaneous interrupted suture, intradermic suture, continuous blanket edge suture, vertical mattress suture, horizontal mattress suture, and the suture of the flap apex of triangular skin flap, and all kinds of suture methods have their own adaptive conditions and requirements (Figs. 2.2, 2.3, 2.4, 2.5, 2.6, and 2.7).
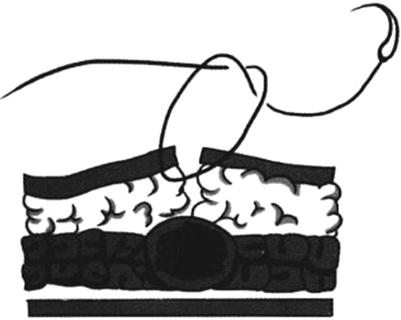

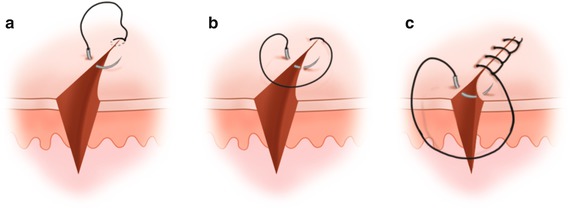
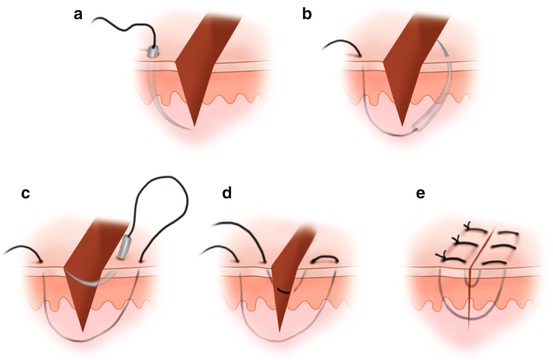
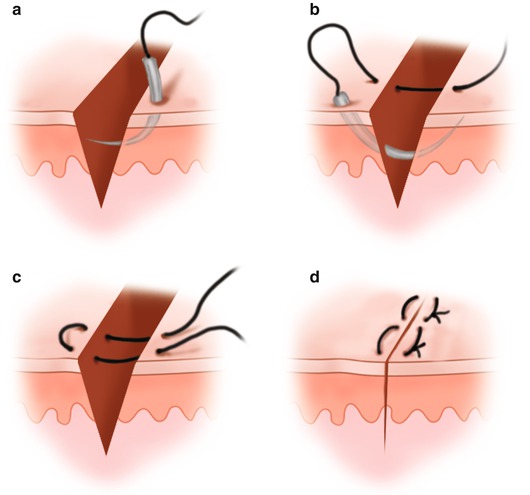
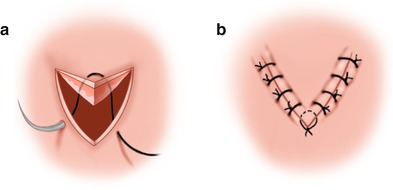
Fig. 2.2
Skin and subcutaneous interrupted suture
Fig. 2.3
Intradermic suture
Fig. 2.4
Continuous lock stitch (a) Location. (b) Locking with the thread. (c) Locked up
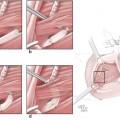
Fig. 2.5
Vertical mattress suture. (a) Needle pierces in on the same side and goes through the deep wound. (b) Needle pierces out on the other side. (c) Needle pierces in on the other side and goes through the shallow wound. (d) Needle pierces out on the same side. (e) completion
Fig. 2.6
Horizontal mattress suture. (a) Needle pierces in the back of the wound and pierce out. (b) Needle pierces in the front of the wound and pierce out. (c) Tie a knot. (d) Completion
Fig. 2.7
The suture of the flap apex of triangular skin flap. (a) Thread goes through the subcutaneous tissue of the triangle’s top. (b) Complete the suture
2.7 Bandaging and Fixation
The bandaging and fixation of postoperative wound should be considered as one of the important steps of the surgery, which may affect the success of surgery to some extent. For example, if the bandaging and fixation are inappropriate after transplantation of free skin graft, the skin graft failure may occur due to movement; after reconstruction of organs such as the ear and nose, the bandaging, shaping, and fixation are also very important.
3 The Basic Techniques of Microsurgery
The microsurgery refers to that under the surgical magnifying glass or the surgical microscope; the delicate surgery of small tissue is performed with microscopic equipment. The microsurgery is both a novel technology and a new interdisciplinary subject; it not only includes various technical problems in clinical surgical applications but also includes basic theory researches such as anatomy, physiology, biochemistry, pathology, and diagnostics which are associated with this technology. Therefore, the microsurgery has become an independent discipline and is called microscopic surgery or microscopic repair surgery. The microsurgery has been widely used in various surgical professional disciplines, along with the development of reparative and reconstructive surgery; microsurgical techniques will be more widely used in clinical practice [1–3].
Related posts:
 Microcirculation Model for Invasive Animal Monitoring
Microcirculation Model for Invasive Animal Monitoring
 Composite Osseomusculocutaneous Thymus Allotransplantation Model
Composite Osseomusculocutaneous Thymus Allotransplantation Model
 In Vivo Chimera Model: Creation of Primary and Secondary Chimera
In Vivo Chimera Model: Creation of Primary and Secondary Chimera
 Experimental Model for Monitoring of Composite Tissue Transplantation Induced Trauma
Experimental Model for Monitoring of Composite Tissue Transplantation Induced Trauma
 Neuroma Model
Neuroma Model
 Tissue Engineering and Oncological Surgery
Tissue Engineering and Oncological Surgery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


