Fig. 11.1
The rat cremaster muscle after dissection prepared for intravital microscopy and recordings
Controlled Hemorrhagic Shock in Rats
Rodents are the most frequently used animals in experimental models for investigations. We summarize the results of the most important physiological recordings in rats, collected from several publications and veterinary sources in Table 11.1. It is important to notice that the rat utilized for the cremaster muscle microcirculation model represents a “young adult”, weighing below 200 g (150–180 g). In small rats, the cremaster muscle is thin enough to allow for transillumination and is transparent enough for adequate in vivo microscopic examination.
Physiology | Units | Approximate value |
|---|---|---|
Adult weight | Grams | 250–400 |
Blood volume | Milliliters per kg | 57.5–69.9 |
Heart rate | Beats per min | 400 |
Respiratory rate | Breaths per min | 66–114 |
Rectal temperature | Centigrade | 37.5 |
Systolic pressure | mmHg | 100–120 |
Diastolic pressure | mmHg | 70–80 |
Mean pressure | mmHg | 85–100 |
A rat weighing 180 g has an overall blood volume about 11 ml [6], so special care should be taken during all surgical dissections of the cremaster muscle as well as during placement of all catheters and probes to avoid blood loss.
Sometimes, the blood loss during the preparation and initial phase of the experiment can be significant even when caution is taken. The same level of caution applies to blood sample collection and it is important to realize that fluid replacement is not simply restoring the microcirculatory hemodynamic to baseline [7].
For an experimental design, the level of shock should be clearly defined according to the estimated volume of blood removed from the intravascular compartment. Applying the universally accepted definitions for humans, there are four classes of hemorrhagic shock: class I (<15 % blood loss); class II (15–30 % blood loss); class III (30–40 % blood loss) and class IV (>40 % blood loss) [8].
Generally, the precise calculation of each separate rat’s blood volume is not possible, nor is it necessary. In fact, the hemodynamic abnormalities within microcirculation are directly dependent on mean blood pressure (MBP) rather than the absolute volume of lost blood. This implies the necessity of precise blood pressure monitoring during the entire experiment (Fig. 11.2) [11]. For arterial blood pressure recordings, the catheter can be placed in the femoral or tail artery and then measurements can be taken through pressure transducers connected to continuous pressure monitoring computers [9, 10]. In previous studies, a MBP of about 50 mmHg in a rat usually results in severe hypovolemic shock, reflecting class III/IV shock in humans, and an MBP below 30 mmHg, especially for extended time, reflects irreversible shock leading to death.

Fig. 11.2
The whole experimental setup for invasive continuous monitoring of blood pressure, temperature, heart rate and ECG used during microcirculatory shock studies (From Parasuraman and Raveendran [11]
Even with minimally invasive procedures in the rat preparation, the hemorrhagic shock itself is a huge disturbance for the homeostasis of an animal, including inflammatory cytokines (TNFα, IL-1β) and inflammatory cell (WBC, PLT) release. The immunological changes accompany major local and general hemodynamic, enzyme (CPK, LDH), and hormone changes. These factors should also be considered when planning any experimental study in this field [21].
Transfusion of Blood and Microcirculation
The clinical treatment of hemorrhagic shock usually involves blood transfusion. The aim of red blood cell (RBC) transfusion is to increase blood oxygen content and oxygen delivery to the tissue. However, oxygen consumption and delivery frequently do not improve after banked blood transfusion and the function of microcirculation may actually worsen. This impairment is thought to relate to biochemical changes in the red blood cells, including a decrease in intracellular 2,3-diphosphoglycerate, which impairs the RBC’s ability to off-load oxygen at the tissue. Additionally, the RBC undergoes a decrease in intracellular adenosine triphosphate, sialic acid, and nitric oxide, which results in a change in the RBC’s shape and deformability. Some studies completed by Siemionow et al. confirmed the important changes in microcirculation after blood transfusion.
In their study published in 2005, Arslan, Sierko, Waters and Siemionow used the rat cremaster model to evaluate microcirculatory changes in vivo after withdrawal of 1 ml of blood and subsequent transfusion with fresh blood or banked blood [12]. Each group underwent a three-stage evaluation: baseline, after blood withdrawal, and after transfusion. Using intravital microscopy, RBC velocity, vessel diameter, functional capillary density (FCD), and leukocyte – endothelial interactions were noted.
The results of this study demonstrated that after blood loss and also after blood transfusion, there are distinct changes in the microcirculation. These changes significantly altered three different parameters of microcirculatory hemodynamics: FCD, leukocyte – endothelial interactions, and RBC conformational changes. In blood loss, the number of flowing capillaries significantly decreased. After transfusion with both banked and fresh blood, capillary perfusion increased. However, neither reached their initial level of capillary density. Fresh blood was significantly more effective at restoring functional capillaries than banked blood, particularly in the distal part of the microcirculation. Activation of leukocyte – endothelial interactions was confirmed by an increased number of rolling and sticking leukocytes after both fresh and stored blood transfusion. However, the degree of observed changes was much higher in the stored blood group (Fig. 11.3
 Lymphaticovenous Anastomosis Training Model in Rat
Lymphaticovenous Anastomosis Training Model in Rat
 Epineural Sleeve End-to-End Repair
Epineural Sleeve End-to-End Repair
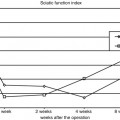
 Somatosensory Evoked Potential Model for Assessment of Nerve Regeneration
Somatosensory Evoked Potential Model for Assessment of Nerve Regeneration
 Peripheral Nerve Surgery Models Crush Injury and Epineural Patch
Peripheral Nerve Surgery Models Crush Injury and Epineural Patch
 Heterotopic Vascularized Ovarian Autotransplantation Model in the Sheep
Heterotopic Vascularized Ovarian Autotransplantation Model in the Sheep
 Defect Repairs After Resections of Laryngeal Cancer, Hypopharyngeal Cancer, and Cervical Esophageal Cancer
Defect Repairs After Resections of Laryngeal Cancer, Hypopharyngeal Cancer, and Cervical Esophageal Cancer




Related posts:
Lymphaticovenous Anastomosis Training Model in Rat
Epineural Sleeve End-to-End Repair
Somatosensory Evoked Potential Model for Assessment of Nerve Regeneration
Peripheral Nerve Surgery Models Crush Injury and Epineural Patch
Heterotopic Vascularized Ovarian Autotransplantation Model in the Sheep
Defect Repairs After Resections of Laryngeal Cancer, Hypopharyngeal Cancer, and Cervical Esophageal Cancer
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
