Medical and Surgical Therapies for Keloids
A. Paul Kelly
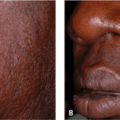
Keloids are medically benign but often psychologically malignant proliferative growths of dermal collagen that usually result from an excessive response to skin trauma in predisposed individuals.1,2 There are, however, spontaneous keloids that develop without a history of trauma. Keloids grow beyond the boundaries of the original wound by invading clinically normal skin. This is in contradiction to hypertrophic scars, which remain within those boundaries and usually regress spontaneously in 1 to 2 years. After several years of growth, keloids usually remain stable; however, some will gradually enlarge, with almost complete central clearing over the lifetime of the patient (Fig. 34-1).
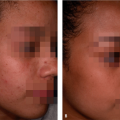
The etiopathogenesis of keloids is unknown (see Chapter 33). However, blacks form keloids more often than whites, and albinos do not develop keloids. Also, the author has treated two patients who developed vitiligo, and some of the vitiliginous lesions were overlying a keloid. The keloids in the vitiliginous areas resolved, whereas the keloids covered by the patient’s normal-colored skin did not improve. Enlargement can be predicted if any part of the keloid has an erythematous border (Fig 34-2). Unfortunately, there are no animal models to study these growths.
There is no single therapeutic modality that is best for all keloids. The recurrence rate for surgical excision is greater than 50% when used as a monotherapy. Thus, medical, physical, or radiologic adjuncts are needed. Location, size, depth, age of patient, past response to treatment, and a family history of keloids determine the type of therapy prescribed.
Intralesional Steroids
Intralesional steroids are usually the treatment of choice. Intralesional cortisone improves keloids by inhibiting alpha 2-macroglobulin, which inhibits collagenase in keloids. An increase in collagenase then increases collagen degradation.1,3,4 Triamcinolone (10–40 mg/mL) is injected every 2 to 3 weeks with a 27- to 30-gauge needle on a small bore Luer-Lock syringe. Larger needles, when injected into hard keloids, often become clogged with keloid tissue. The papillary dermis is the target because that is where collagenase is produced. If there is no regression of the keloid after four injections or if the keloid no longer responds to further injections, surgery is recommended.
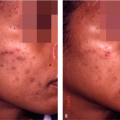
In addition, intralesional steroids are commonly used as an adjunct treatment in patients undergoing excision of lesions. Triamcinolone acetonide 40 mg/cc is injected into the postoperative sites every 2 to 3 weeks for a total of four injections, starting 1 week after the sutures are removed (Fig. 34-3A,B). If the site of keloid removal starts to enlarge later on, intralesional triamcinolone is restarted. Patients should be forewarned that the injection sites may become hypopigmented and stay that way for 3 to 6 months. A mixture of equal parts of 40 mg/cc of triamcinolone acetonide and 2% Xylocaine can be used to anesthetize the operative site. The steroid slows wound healing, so sutures should remain in for 10 to 20 days, especially on the earlobes.
Intralesional Interferon
Intralesional interferon has been reported to be effective in improving the appearance of keloids.5,6,7 Berman and Flores5 reported an 18.7% recurrence rate when injecting 1 million units of interferon alpha-2b per linear centimeter in the postoperative site immediately after surgery and 1 to 2 weeks later. The recurrence rate with excision alone was 51%. If the excision site is long, the patient should be premedicated with acetaminophen to help prevent the flulike symptoms caused by the interferon. Another limiting factor with interferon is its high cost. Interferon alpha and gamma inhibit type I and III collagen synthesis. Other potential mechanisms of action include reduced production of transforming growth factor beta and increased levels of collagenase activity.6
Imiquimod Therapy
Imiquimod is a topical therapeutic agent that acts as an immune-response modulator by inducing interferon-α, tumor necrosis factor-α, and interleukin-1, -6, and -8.
Berman and Kaufman8 evaluated the effects of postoperative imiquimod 5% on the recurrence of excised keloids. Imiquimod cream was applied to the postoperative site daily for 8 weeks, starting immediately after surgery. Those who experienced marked irritation had to discontinue the medication for 3 to 7 days and then resume therapy. Patients with large excisions, wounds under tension, or wounds closed with flaps or grafts are advised not to use imiquimod for 4 to 6 weeks after excision because the postoperative site may splay or dehisce. Approximately half of the patients treated with imiquimod developed hyperpigmentation. Berman and Kaufman8 also demonstrated that postoperative imiquimod cream reduced recurrence of keloids. The expression of genes associated with apoptosis is significantly altered in keloidal tissue treated with imiquimod.
Berman and Kaufman8 evaluated the effects of postoperative imiquimod 5% on the recurrence of excised keloids. Imiquimod cream was applied to the postoperative site daily for 8 weeks, starting immediately after surgery. Those who experienced marked irritation had to discontinue the medication for 3 to 7 days and then resume therapy. Patients with large excisions, wounds under tension, or wounds closed with flaps or grafts are advised not to use imiquimod for 4 to 6 weeks after excision because the postoperative site may splay or dehisce. Approximately half of the patients treated with imiquimod developed hyperpigmentation. Berman and Kaufman8 also demonstrated that postoperative imiquimod cream reduced recurrence of keloids. The expression of genes associated with apoptosis is significantly altered in keloidal tissue treated with imiquimod.
 Figure 34-1 Central clearing of Keloid. |
5-Fluorouracil Therapy
Intralesional 5-fluorouracil (5-FU) can also be used for treatment of hypertrophic scars and keloids. 5-FU is an antimetabolite that blocks DNA synthesis by blocking thymidylate synthetase. It decreases collagen synthesis in proliferating fibroblasts. It can be used alone or in conjunction with triamcinolone.9 Better results are achieved when used in combination with triamcinolone. The standard dosage is 5-FU 50 mg/mL, 0.9 mL, and 0.1 mL of triamcinolone acetonide 10 mg/mL. Lesions are injected 1 to 3 times a week for 10 to 12 weeks.
Other Therapies
The use of pentoxifylline (Trental) 400 mg three times a day has been suggested as a useful antifibrotic agent but had limited success in preventing recurrence of excised keloids.10




Related posts:


Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
