Surgical Treatment of Skin Cancers in Darker Racial Ethnic Groups
P. Kim Phillips
Skin cancer is the most common type of cancer in the United States.1 Important risk factors associated with the development of nonmelanoma skin cancer (NMSC) and melanoma includes Fitzpatrick phototype I skin, Celtic ancestry, fair complexion, and light eyes. Hispanics, African Americans, and Asians, both having darker skin pigmentation than Caucasians, are at lower risk for developing skin cancer.2,3,4,5,6,7,8,9,10,11,12,13,14 Although the incidence of NMSC and melanoma is lower in Hispanics, African Americans, and Asians, tumors in these populations tend to present in more advanced stages and carry a poorer prognosis than those in Caucasians. Skin cancers can cause significant cosmetic disfigurement. Therefore, selection of appropriate excisional modalities is essential for optimizing aesthetic outcomes.
Squamous Cell Carcinoma
Squamous cell carcinoma (SCC) is the most common cutaneous malignancy in African Americans. SCC is an invasive epithelial malignancy exhibiting keratinocyte differentiation. When it occurs in African Americans, tumors tend to present in more advanced stages. SCC accounts for about three fourths of the mortality attributable to NMSC in African Americans.13,14
Numerous studies have reported that sun exposure does not appear to be an important etiologic factor in the development of SCC in African Americans, as lesions most frequently occur on non–sun-exposed skin. SCCs arising on non–sun-exposed skin tend to be more aggressive and have a greater potential to metastasize. When SCCs do arise on sun-exposed areas of pigmented skin, they are most commonly found on the “midfacial triangle,” which includes the forehead, nasal tip and lip. These tumors also occur to a greater degree on the legs, especially in elderly women.
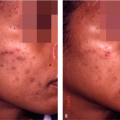
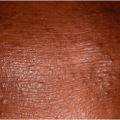
A significant predisposing factor for the development of SCC is the presence of scar tissue arising from a chronic inflammatory process such as discoid lupus erythematosus, cutaneous horns, chronic leg ulcers, or scrotal ulcers (Fig. 36-1). Further, Hubbell et al. reported that mortality was greater when the lesion arose from a chronic inflammatory process and was highest in perianal tumors.13
Basal Cell Carcinoma
Basal cell carcinoma (BCC) is the most common skin cancer in the United States, accounting for at least 75% of all NMSCs. However, more than 99% of these cases occur in whites. The rarity of this cancer in darkly pigmented skin is accounted for by the central role of ultraviolet radiation in the development of BCC13,14. However, other risk factors have also been reported for BCC, including prior exposure to radiation, trauma, arsenic ingestion, immunosuppression, and the basal cell nevus syndrome.
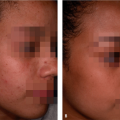
BCC typically exhibits characteristic nests or cords of small, dark-staining epithelial cells with palisading of the peripheral cells. Tumors may be pigmented or nonpigmented and arise most commonly on the face, head, and neck (Fig. 36-2). However, lesions may also occur on non–sun-exposed skin. BCCs are generally similar in histology and clinical course in both African Americans and Caucasians. Pigmented BCCs are found with increased frequency in blacks.
Malignant Melanoma
Risk factors for malignant melanoma in darker racial ethnic groups include exposure to ultraviolet light, a history of blistering sunburns, albinism, burn scars, exposure to ionizing radiations, pre-existing pigmented lesions, and history of trauma.6,7,8,9,10,11,12 Interestingly, family history does not appear to be a significant risk factor in the development of melanoma in persons of color.
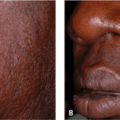
Individuals with pigmented skin are more likely to develop acral melanoma, both the acral lentiginous and subungual subtypes. Acral lentiginous melanoma is a very
aggressive tumor that commonly occurs on the plantar surface of the feet, palms, and digits and presents as a rapidly spreading, darkly pigmented patch (Fig. 36-3A,B). Subungual melanoma typically arises on the hand, and treatment often requires amputation. Occasionally, these tumors may be amelanotic, which often leads to a delay in the diagnosis. These lesions have a propensity to metastasize to the central nervous system, liver, lungs, bone, and lymph nodes. Prognosis in these cases is poor.
aggressive tumor that commonly occurs on the plantar surface of the feet, palms, and digits and presents as a rapidly spreading, darkly pigmented patch (Fig. 36-3A,B). Subungual melanoma typically arises on the hand, and treatment often requires amputation. Occasionally, these tumors may be amelanotic, which often leads to a delay in the diagnosis. These lesions have a propensity to metastasize to the central nervous system, liver, lungs, bone, and lymph nodes. Prognosis in these cases is poor.
 Figure 36-1 Squamous cell carcinoma of the scalp in an African American patient with discoid lupus. (Courtesy of Pearl E. Grimes, MD.) |
 Figure 36-2 A: Basal cell carcinoma of the face in an African American. (Courtesy of Carl Washington, MD.) B: Basal squamous cell carcinoma of the finger in a 90-year-old African American male with vitiligo. (Courtesy of Pearl E. Grimes, MD.) |
Overall, the outcome of melanoma is worse for deeply pigmented individuals when compared with white skin. According to the California Cancer Registry, melanoma was diagnosed only after metastasis to a remote site for 12% of black men, compared with only 6% of white men.
When faced with a skin cancer in darker racial ethnic groups, as in all other patient populations, the surgeon’s primary focus must be: (a) complete removal of the tumor, (b) preservation of function of key anatomic structures, and (c) restoration of cosmesis. These key principles must be considered in the order presented to achieve high cure rates and prevent tumor recurrence. This chapter will focus on a discussion of common surgical techniques required to manage most cutaneous malignancies as well as reconstruction of postoperative defects to achieve acceptable aesthetic outcomes.
Primary Excision
Chief among the surgical procedures performed on skin is the elliptical or fusiform excision. It is used for the therapeutic removal of benign and malignant lesions and is critical to properly diagnose pigmented lesions and inflammatory diseases of the skin. The elliptical excision encompasses all the fundamental elements of more advanced procedures, such as local flaps, skin grafts, and cosmetic procedures. Those elements that must be mastered include knowledge of local anatomy, cosmetic units,
incision technique, tissue handling, and wound management. All of these elements are the foundation upon which more advanced surgical procedures are based. The goal of the elliptical excision, as with any other surgical procedure, is a cosmetically acceptable result. The scar should be hairline in width and well concealed within natural skin tension lines.
incision technique, tissue handling, and wound management. All of these elements are the foundation upon which more advanced surgical procedures are based. The goal of the elliptical excision, as with any other surgical procedure, is a cosmetically acceptable result. The scar should be hairline in width and well concealed within natural skin tension lines.
 Figure 36-3 A: Nodular malignant melanoma of the heel. B: Acrolentiginous melanoma of the digit. (Courtesy of Carl Washington, MD.) |
Patient evaluation
After obtaining a thorough history of present illness as well as information regarding medications, allergies, review of systems, and past medical surgical history, physical examination should be performed with the aid of appropriate lighting with the patient in a seated position. The most important aspect of the physical examination is identifying anatomic landmarks, including cosmetic units and relaxed skin tension lines. These important landmarks are used to help camouflage the surgical scar.
The importance of understanding cosmetic units is critical. Cosmetic units are regional subunits or anatomic areas defined by gradations of light and shadow that are determined by the underlying framework of soft and hard tissue. Scars limited to one cosmetic unit or at the boundary between two cosmetic units will appear less noticeable than a scar that crosses the border between two units.
One of the basic principles for cosmetic closure of surgical wounds is placement of scar in the natural skin tension lines. Proper orientation of scars makes them imperceptible. Wounds heal so well that patients have the impression that there is no scar.
Langer’s lines should be familiar to all dermatologic surgeons. Tension lines may vary between patients, but they become more prominent with age. The severity of tension lines is influenced by sun exposure, cigarette smoking, and skin type. It is important, therefore, that each patient be examined closely when planning an excision. Visual inspection, palpation, and gentle manipulation are necessary to confirm the location of relaxed skin tension lines and to determine the impact of a particular repair on adjacent structures. There are many locations, such as the glabella, lateral margins of the chin, or shoulder, for which there is more than one set of relaxed skin tension lines. Patients should be encouraged to smile or make other specific facial expressions such as pursing the lips or raising the eyebrows to help clearly delineate skin tension lines.
Surgical technique
Elliptical excision
The classic elliptical or fusiform excision is based on a design that bears a length-to-width ratio of 3:1 or 4:1, with the apical angles ranging from 30 degrees to 75 degrees.15 This design is intended to eliminate tissue redundancies or dog-ear formation at the poles of a linear closure.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


