CHAPTER 50 Medial pedicle vertical mammaplasty
History
The inverted T inferior pedicle approach to breast reduction solved many problems.1 It was reliable and reproducible. It became the standard method in teaching programs and all residents finished their training being comfortable with its design and execution. Some surgeons in South America2,3 and Europe4–6 began describing procedures for breast reduction without an inframammary scar. The “vertical” approach to breast reduction became more popular but there were problems. Many surgeons felt that the inverted T procedure did not need “fixing”.
The superomedial vertical breast reduction7 solved some of the problems but it still seemed only applicable to moderate sized breast reductions. But the principles of separating the design of the pedicle, the parenchymal resection and the skin resection pattern however are applicable to all breast reductions. The controversy still persists as to which pedicle is best, what is the best approach to the tissue resection and which is the best skin resection design. The best procedure in the final analysis is that which each surgeon finds they can achieve the best result.
The vertical design involves a vertical wedge resection of breast tissue (and skin) whereas most inverted T patterns remove tissue (and skin) in a horizontal pattern. This vertical wedge excision allows the base to be narrowed and improves projection. The method described below uses the Wise pattern8 (not just the keyhole) as a good pattern of breast tissue that should remain behind after resection. All other breast tissue and fat should be removed either with direct excision or liposuction. Both the parenchyma and the skin should be closed without tension. This method also relies on excising the heavy inferior breast tissue so that bottoming out is less likely to occur.
Physical evaluation
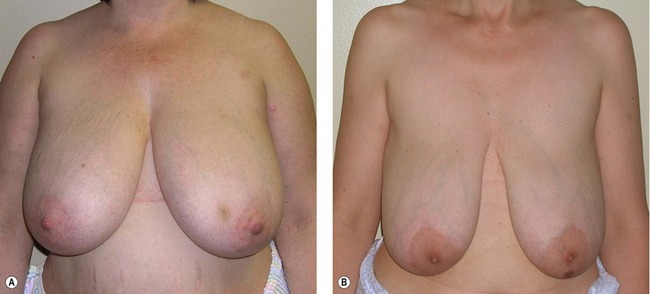
1. Assess the upper breast border. (Fig. 50.1A,B). This border will not change with the surgery. The distance from the clavicle to the upper breast border will determine whether the patient is “high-breasted” or “low-breasted”.
2. Assess the level of the inframammary fold. The fold level is quite variable from patient to patient. The fold can be raised to some degree with this procedure but an aggressive attempt to raise the fold will also increase the revision rate.
3. Assess the lateral breast border. If the breast is quite wide the parenchyma laterally will need to be excised and the breast coned in order to narrow the breast base.
4. Assess the amount of upper pole fullness. Some patients have unrealistic expectations about what surgeons can achieve – and sometimes the surgeons do as well. The amount of upper pole fullness can be rarely increased without the use of exogenous tissue such as an implant or fat injections.
5. Design the new nipple position relative to the upper breast border. The ideal nipple position should be determined preoperatively with the patient standing. For a “C” cup brassiere the new nipple should be about 10 cm below the upper breast border.
6. Use the Wise pattern for determination of final breast shape. The Wise pattern comes from a brassiere pattern and is not just about the keyhole design. The whole pattern is ideal for determining what should be left behind to get a good final shape. All tissue beyond the Wise pattern should be removed.
7. Close the breast pillars without undue tension. The tissue beyond the Wise pattern should be excised. The breast tissue should be excised directly and any fat beyond the breast tissue can be either directly excised or removed by liposuction. The pillars should be closed without tension. Neither the breast tissue nor the skin should be closed under tension or complications will increase and the shape will relapse.
Anatomy
The deep vessels come from the internal mammary system and perforate the pectoralis muscle usually just above the fifth rib (about 4–6 cm above the inframammary fold) and just medial to breast meridian. There are branches from this system which extend laterally in the septum described by Elisabeth Wuringer.9 The arteries are accompanied by venae comitantes. The deep system supplies an inferior and central pedicle.
The superficial system has been documented by Ian Taylor10 and the arteries and veins have been pushed into the superficial fatty layer as the breast enlarges. The arteries and veins travel separately and the veins are quite superficial and can be easily seen through the skin. They drain superiorly and medially which means that superior and medial pedicles are well supplied.
There are several nerves that supply sensation to the nipple and areola. The lateral branch of the fourth intercostal nerve is the main nerve but there are also medial nerves and some from the superior thoracoacromial system. The lateral branch of the fourth intercostal nerve has one branch that runs above the breast tissue toward the areola and a deep branch which runs along the pectoralis muscle and then runs vertically toward the areola at the breast meridian. This deep and superficial system is similar to the vascular supply. Maintaining a full thickness superomedial pedicle will preserve the deep branch of the nerve although the superficial lateral branch will be sacrificed.11 Superior and medial nerve branches will also be preserved. About 85% of patients with the superomedial pedicle will recover normal to near-normal sensation.
Technical steps
Marking
1. New nipple position (Fig. 50.2A,B). The key to marking is the upper breast border and evaluating the breast footprint on the chest wall. The upper breast border is the junction between the breast and the upper chest wall. It lies just below the pre-axillary fullness and the indentation below the pre-axillary fullness can be marked and carried medially. The breast meridian is then marked. It is not drawn through the existing nipple but drawn where the ideal nipple position should be. The new nipple position should then be placed on the new breast meridian about 8–10 cm below the upper breast border. This often corresponds with the level of the inframammary fold.
2. Areolar opening (Fig. 50.3). The top of the areola is then marked 2 cm above the new nipple position. The new areolar opening is drawn so that it will be a circle when it is closed. A good pattern is to use a large paper clip as a template. A large paper clip is 16 cm in length. This matches a 5 cm diameter areola. There is no need to make the opening in a “mosque” shape.
3. Skin resection pattern (Fig. 50.4A–C
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


