Maxillomandibular Fixation of Mandible Fractures
Joseph Baylan
Dana Johns
DEFINITION
Maxillomandibular fixation (MMF) can be used independently for closed reduction or in combination with open reduction and internal fixation (ORIF) for treatment of mandible fractures.
ANATOMY
An understanding of dental anatomy and normal occlusal relationship is important when planning treatment with MMF.
Incisor and canine teeth have a conical shape, whereas premolars and molars have a square shape.
Normal occlusion is defined when the mesiobuccal cusp of the maxillary first molar occludes in the buccal groove of the mandibular first molar (FIG 1).
The mandibular arch is lingual to maxillary arch.
PATHOGENESIS
Two most common causes of mandible fractures are assault and motor vehicle collisions.
Additional causes include gunshot wounds, falls, and sports injuries.
PATIENT HISTORY AND PHYSICAL FINDINGS
Focused history and physical examination
Mechanism of injury
Full intraoral and dental examination
Evaluate for anterior or posterior open bite in centric occlusion.
Evaluate for dental trauma and overall state of dental health.
Evaluate areas of wear on the teeth (“wear facets”) to determine which teeth and where teeth made daily contact prior to the injury. These wear patterns can give an idea of preinjury occlusion, as the occlusion may not have been normal.
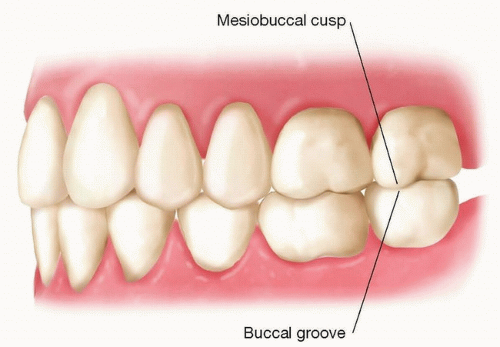
FIG 1 • Normal occlusion.
Tips
Use tongue blade intraorally for complete soft tissue and dental evaluation.
Previous dental imaging and molds can be used to determine preinjury occlusion.
IMAGING
Panorex plain films may be used to diagnose mandible fractures and can be used easily for postfracture follow-up.
CT imaging is superior to plain films for diagnosing and evaluating mandibular fractures.
SURGICAL MANAGEMENT
Indications for MMF3:
Temporary fragment stabilization as bridge to ORIF
Conservative treatment
Alveolar crest fractures
Tension band in conjunction with rigid internal fixation
Control of occlusion in the posttraumatic/postoperative period
Preoperative Planning
Nutrition optimization is important for postoperative healing.
For edentulous patients, consider intraoral prosthesis to maintain maxillary-mandibular relation.
Appropriate preoperative evaluation of cardiopulmonary status is always indicated prior to any surgical procedure.
Equipment
Erich arch bars and either 24- or 26-gauge dental wire (surgeon preference).
MMF set should include heavy needle drivers, wire cutting scissors, a pickle fork, and intraoral retractors (ie, Weider adult cheek tongue retractor, Minnesota, etc.).
Optional: MMF screws
Anesthesia
General anesthesia via nasotracheal intubation is preferred.
Orotracheal intubation with ETT posterior to the retromolar trigone and submental intubation are other alternatives if nasotracheal intubation is not possible.
Tracheostomy should be performed if there are contraindications to the above-mentioned methods of anesthesia.
Positioning
The patient is placed in the supine position with a shoulder roll and arms tucked.
TECHNIQUES
▪ Arch Bars
Check occlusion, paying attention to avulsed teeth and wear facets, to obtain preinjury occlusion.
If possible, obtain prior dental records; however, this is often not possible in the acute trauma setting.
Measure and cut appropriate length of arch bar required to span left second molar to right second molar.
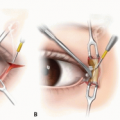
The arch bar should sit occlusal to the gingiva along the dental equator so as to avoid damage to the gingiva. Furthermore, the arch bar hooks should lie apical and symmetrical in the mandible and maxilla (TECH FIG 1A).Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree