Mastopexy with Chest Wall–Based Flap and Pectoralis Muscle Loop
Ruth Graf
Thomas Biggs
André Ricardo Dall’Oglio Tolazzi
Maria Cecília Closs Ono
Introduction
The evolution of all surgery, including breast surgery, is persistent and ongoing (1,2,3,4,5,6,7,8,9,10,11,12,13,14). The great advances by Wise (15), Pitanguy (16), Lassus (17,18,19), Lejour (20,21,22,23), Benelli (24), and others have not only simplified the operative plan, but have also contributed to a shorter scar and a more aesthetic breast. This chapter describes a maneuver designed to give a better shape. This maneuver involves the use of a chest wall–based flap of breast tissue that is moved into the upper pole of the breast and held in place by a loop of pectoral muscle under which it is passed. The technique can be used with different kind of incisions: standard inverted T, short T, L-shaped incisions, or periareolar-vertical incisions. Our choice, and the maneuver described in this chapter, is a vertical incision with whatever redundant skin remains after excising the vertical ellipse removed from around the nipple and closed with a round block suture. This is best described as a circumvertical excision. If reduction is necessary, it can easily be carried out in this maneuver by removing the desired amount from under the breast and in the most appropriate location for resection. There is no limit to the amount of breast tissue that can be removed.
Technique
Marking is done with the patient in the upright position. Lines are drawn first straight down the midline from the suprasternal notch to the xiphoid process and second from a point 5 cm from the suprasternal notch at the clavicle to the nipple-areola complex (NAC) and then straight down to the areola. A point at 17 to 20 cm on the suprasternal–NAC line is marked (point A), which will be the top of the areola. A point is made (point D) on the line through the middle of the breast and 2 to 4 cm above the inframammary fold. This distance varies between 2 and 4 cm depending on the size of the breast (Fig. 84.1). The breast is then gently displaced laterally (as in the technique described by Lejour), and a line is drawn parallel to the midline and connected to point D. A similar line is drawn with the breast displaced medially. A distance of 5 to 8 cm is measured from point D on the medial and lateral lines (points B and C). It should be pointed out that the tension resulting from this displacement should be firm enough to allow adequate skin resection but not so tense as to create difficulty with closure. This distance varies also in accordance with the size and laxity of the breast. Gently curved lines are drawn from point A to point B and C. Line A–B should never be closer than 9 cm to the midline and line A–C never less than 10 cm from the anterior axillary line.
The variation in distances of point D to the inframammary fold and of lines B–D and C–D allows the surgeon the latitude of adjustments, depending on the size of the breast. The larger the breast is to be, the greater are these distances; however, the distances should never exceed 4 and 8 cm, respectively.
One additional item in the markings is to move points B and C slightly closer together so that when they are closed there will be no significant tension.
Operative Procedure
The patient is placed supine on the operating table, and, after induction with general or epidural anesthesia (local is possible) and preparation and draping, the incision markings are infiltrated subdermally (except superior to the areola), with a dilute epinephrine-in-saline solution (1:100,000). The area of the skin demarcated by lines A–B, A–C, B–D, and C–D is deepithelialized (Fig. 84.2), leaving the NAC (4.5 to 5 cm in diameter) in place. An incision is made in the dermis transversely along lines B–D and C–D, passing 1 cm below NAC. This is the beginning of the creation of the chest wall–based flap (Fig. 84.3). Along the vertical lines this incision is beveled inward for 1 to 2 cm to preserve tissue on the medial and lateral pillars for closure later. After preserving this tissue, the incisions continue inward and away from the flap so the base is broad. This dissection is carried to the chest wall, with a minimal amount of subcutaneous tissue being left on the skin as dissection is carried to the inframammary fold.
After this dissection has been performed laterally and medially a large hook is placed in the NAC and the breast is lifted straight up. Then, an incision is made in the breast tissue from point B to point C, proceeding to the pectoral fascia. Great care must be taken at this point not to undercut the flap (chest wall pedicle). The flap is now freely mobile and is based on vessels from the fifth and sixth intercostal spaces, as a perforator flap (Figs. 84.4 and 84.5). The flap is free from all of the four sides: superior, lateral, inferior, and medial. It is very important that the flap not be restrained; if it is, continuous dissection should be extended to the pectoral fascia. This freely mobile, totally chest wall–based flap is made up of the tissue that in other procedures “bottoms out,” but in this procedure it is being transposed into the upper pole, where it will remain permanently.
The breast tissue is retracted upward and cephalad and dissected off the pectoral fascia up to the second intercostal space, creating a space in the upper pole of the breast into which the flap will be fixed. Before this, however, a strip of pectoral muscle approximately 8 to 10 cm long and 1.5 to 2 cm wide is marked with methylene blue. Its caudal or inferior line is at the cephalad end of the flap base (Fig. 84.6).
This muscle strip is elevated incorporating no more than one half of the muscle (the posterior fascia of the muscle is not
violated), and the donor site is close with 2-0 nylon. This loop will be used to help hold the flap in position in the upper pole. The flap is then passed under the pectoral loop into the space of the upper pole of the breast. It is very important that all dermal elements on the flap be completely passed under this loop. The dermis of the flap is then sutured to the pectoral fascia with a running 2-0 nylon suture, starting laterally and finishing medially. If, after passing the flap under the loop, there seems to be excessive tension on the loop causing pressure on the flap, the loop can be released by a small amount of dissection laterally (medial dissection could disrupt the origin of the pectoralis) (Fig. 84.6).
violated), and the donor site is close with 2-0 nylon. This loop will be used to help hold the flap in position in the upper pole. The flap is then passed under the pectoral loop into the space of the upper pole of the breast. It is very important that all dermal elements on the flap be completely passed under this loop. The dermis of the flap is then sutured to the pectoral fascia with a running 2-0 nylon suture, starting laterally and finishing medially. If, after passing the flap under the loop, there seems to be excessive tension on the loop causing pressure on the flap, the loop can be released by a small amount of dissection laterally (medial dissection could disrupt the origin of the pectoralis) (Fig. 84.6).
 Figure 84.1. Basic markings of the vertical technique. Lines are drawn straight down the midline from the suprasternal notch to the nipple-areola complex (NAC). Point A, 20 cm from the clavicle, will be the top of the areola (A), from a point 5 cm from the suprasternal notch at the clavicle to the NAC and then straight down parallel to the midline line, crossing the inframammary crease, not less than 11 cm (B). The breast is gently, with the Lejour maneuver, displaced laterally (C) and medially (D) to obtain the vertical lines. The suprasternal notch is noted to be at the cephalad edge of the bone, not down into the notch. |
 Figure 84.2. A: The vertical lines cross at the midbreast line, 2 to 4 cm above the inframammary fold, and point D is made. B: A distance of 5 to 8 cm is measured on the medial and lateral lines, and points B and C are placed, respectively. A gently curved line is drawn from point A to point B (C), and again from point A to point C (D). Line A–B should never be closer than 9 cm to the midline, and line A–C should never be less than 10 cm from the anterior axillary fold. |
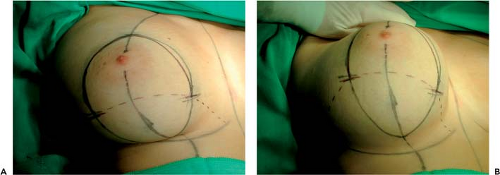 Figure 84.3. A, B: Patient on the operating table. Skin demarcated with vertical lines and the chest wall–based flap. |
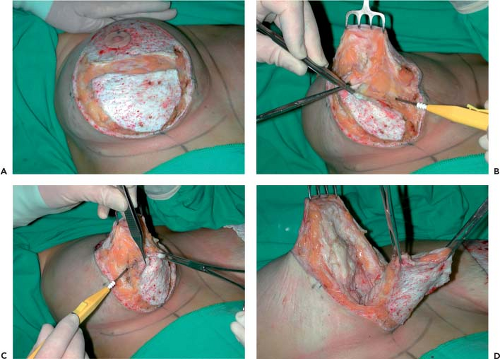 Figure 84.4. A: Deepithelization and dermis incision following demarcation, to 2 cm above points B and C. Along the vertical lines, this incision is beveled inward for 1 to 2 cm to preserve tissue on the medial (B) and lateral (C) pillars, preserving this tissue for closure later. D: A large hook is placed in the nipple-areola complex, the breast is lifted straight up, and dissection of the breast tissue from point B to point C is carried out 1 cm below the areola, proceeding to the pectoral fascia. |
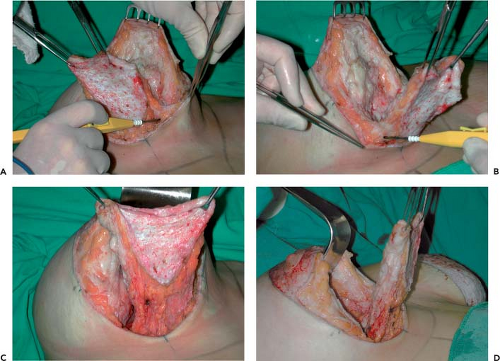 Figure 84.5. A, B: The incisions continue inward and away from the flap so the base is broad. This dissection is carried to the chest wall with a minimal amount of subcutaneous tissue being left on the skin as dissection is carried to the inframammary fold. C, D: Undermining of chest wall–based flap maintaining the large base. |
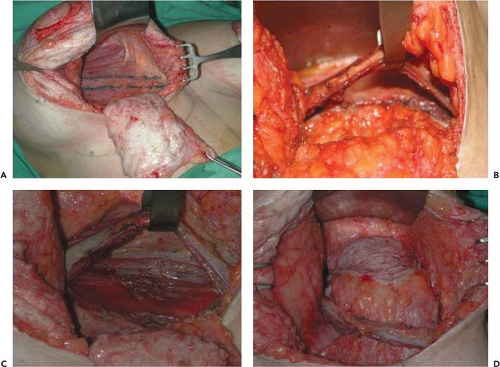 Figure 84.6. A strip of pectoral muscle approximately 8 to 10 cm long and 1.5 to 2 cm wide is marked with methylene blue just superior to the base of the chest wall–based flap (A) and elevated leaving the deep half of the muscle intact (B). Passage of chest wall–based flap under the bipedicled muscular flap, closure of the donor site (C), and suture of the flap to the second intercostal space (D). |
With the flap in the correct position and the breast suspended by the hook in the NAC, breast tissue excess is removed. At this step of the surgery the reduction is made in accordance with the breast’s size and the desire of the patient. The main block of tissue is removed as an inverted central kill, from the base of the breast laterally and a lesser amount centrally to reduce the base and the excessive projection of the breast. The highest reduction with this technique (vertical incision and circumvertical closure) is 800 to 1,000 g, including the suction in the lateral aspect of the breast, although the chest wall–based flap can be used in any breast size.
Related posts:
 Follow-Up After Surgery for Primary Breast Cancer: Breast-Conserving Therapy and Mastectomy
Follow-Up After Surgery for Primary Breast Cancer: Breast-Conserving Therapy and Mastectomy
 Breast Implants: Materials and Manufacturing Past, Present, and Future
Breast Implants: Materials and Manufacturing Past, Present, and Future
 Reconstruction of the Irradiated Breast
Reconstruction of the Irradiated Breast
 Perforator Flaps in Breast Reconstruction
Perforator Flaps in Breast Reconstruction
 Lipomodeling of the Reconstructed Breast
Lipomodeling of the Reconstructed Breast
 The Periareolar Approach to Augmentation Mammaplasty
The Periareolar Approach to Augmentation Mammaplasty
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


