Mastopexy
David A. Hidalgo, M.D.
Jason A. Spector, M.D.
New York, N.Y.
From the Division of Plastic Surgery, Weill Cornell Medical College.
Received for publication January 24, 2013; accepted March 27, 2013.
Copyright © 2013 by the American Society of Plastic Surgeons
DOI: 10.1097/PRS.0b013e31829fe4b4
Disclosure: Neither author has a financial interest in any of the products or devices mentioned in this article.
Related Video content is available for this article. The videos can be found under the “Related Videos” section of the full-text article, or, for Ovid users, using the URL citations published in the article.
Learning Objectives: After reading this article, the participant should be able to: 1. Assess patient physical characteristics to determine candidacy for mastopexy and select the most appropriate technique. 2. Understand current methods, their relative effectiveness, and key technical elements. 3. Become conversant with methods to fixate, redistribute, and autoaugment the parenchyma. 4. Understand the benefits and pitfalls of combining augmentation and mastopexy, and how to best design and execute these procedures. 5. Become cognizant of mastopexy complications and how to both avoid and treat them.
Summary: Mastopexy includes multiple skin incision design and parenchymal manipulation options. Patient evaluation includes assessment of goals, degree of ptosis, tissue volume, skin quality, and breast position on the chest wall. There are critical technical details for each of the three incision options, the various methods of parenchymal manipulation, and implant placement. The potential for complications is greatest for combined augmentation and mastopexy. Although they are effective, mastopexy procedures have the greatest incidence of litigation among aesthetic breast procedures. (Plast. Reconstr. Surg. 132: 642e, 2013.)
Mastopexy is by nature problematic because it trades significant scars for limited lift capability on arguably the most aesthetically sensitive female body part. The incidence of untoward results, revisions, and litigation is high despite mastopexy being ranked well behind augmentation and reduction in the number of procedures performed annually.1,2 Nevertheless, it is effective when the right technique is matched to favorable indications.
There are three basic incision types, with several variants. There are multiple options for parenchymal fixation, redistribution, and autoaugmentation. Combining breast augmentation with mastopexy increases the risk for complications but may be necessary to achieve the best result (reference 5: Therapeutic, Level III Evidence).3–5
Mastopexy spans a spectrum of procedures from mastopexy with modest reduction; to mastopexy alone when tissue volume is adequate; to augmentation combined with mastopexy when there is a tissue deficiency, marked skin excess, or both. The scope of surgery, the recovery, and the potential for complications are least for skin-only procedures, minimal for mastopexy with modest reduction, and greatest with combined augmentation and mastopexy.
Essentials of Preoperative Assessment and Management
Patient Evaluation
Relevant patient history includes age; goals; pregnancies and breast feeding history; medications including psychotropic agents, birth control, and hormone replacement therapy; history of weight fluctuations, bleeding, or clotting problems; and previous surgery.6 Physical evaluation includes height and weight measurement, assessment of breast position on the chest wall, nipple distance from the clavicle, areolar diameter, tissue volume, skin quality and amount, and asymmetry.
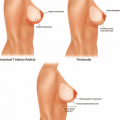
Nipple position relative to the inframammary crease determines the degree of ptosis (Table 1).7
Nipple position relative to the inframammary crease determines the degree of ptosis (Table 1).7
Table 1. Ptosis Classification* | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||
Patients primarily exhibiting low breast position but without significant ptosis do not benefit from mastopexy. Those with normal position and only minimal ptosis do not benefit enough to justify the scar burden entailed.
Patient Education
Patients often expect that mastopexy will provide upper pole fullness, raise the breast completely above the inframammary crease level, and leave either minimal or no scars. They do not realize that the breasts are not lifted from above, as they frequently simulate, but instead are pushed up from below, an inherently less powerful approach necessary for scar concealment. Descriptions of mastopexy scar patterns, particularly when a vertical component is necessary, often produce dismay. Photographs of representative results typically allay fears in those who are realistic, however.
Patients primarily seeking breast augmentation but have low nipple position, enlarged areolar diameters, or nipple position asymmetry may require mastopexy only as a limited adjunct. Although conservative circumareolar mastopexy usually suffices in these cases, a vertical component may be required on one side if significant nipple position asymmetry exists (Fig. 1).
Volume-deficient mastopexy candidates often require breast implants. The additional risks must be explained and include implant malposition, capsular contracture, and the need for periodic replacement. Combining augmentation with mastopexy has a much higher incidence of complications than either procedure alone.3,8
Advantages and Disadvantages of Treatment Options
Crescent Mastopexy
Crescent mastopexy was originally described as an eccentric circumareolar skin excision without areolar
mobilization and no purse-string suture.9 Problems with scar widening and oval areolar deformity were reported. A more recent description advocates excising a wedge of breast tissue down to the pectoralis muscle to prevent these problems.10 Crescent mastopexy is not widely used today.
mobilization and no purse-string suture.9 Problems with scar widening and oval areolar deformity were reported. A more recent description advocates excising a wedge of breast tissue down to the pectoralis muscle to prevent these problems.10 Crescent mastopexy is not widely used today.
 Fig. 1. Breast augmentation with right circumareolar mastopexy and left vertical mastopexy. (Left) Preoperative view showing postpartum atrophy, nipple position asymmetry, and volume asymmetry. (Right) Postoperative view with 225-g round silicone implant on the right and 250-g implant on the left. |
Table 2. Mastopexy Options and Indications | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||
Circumareolar Mastopexy
Circumareolar mastopexy was originally described as a “donut” mastopexy because of the shape of the skin excision design.11 The best indication was for protuberant areolas. Since then, variants with eccentric skin excision design and wide undermining have been described, with some including inferior suture invagination of the parenchyma.12,13 Circumareolar mastopexy by itself does not elevate nipple position enough or remove sufficient skin to be very effective.
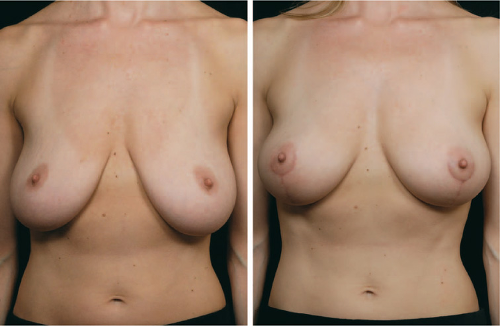
Circumareolar mastopexy is best used as an adjunct in breast augmentation. It can reduce areolar diameter and simultaneously raise nipple position modestly (<2 cm) by using an eccentric shaped excision pattern that includes intra-areolar skin (Table 2). It can also increase infra-areolar skin show in ptotic breasts and can correct nipple position asymmetry when used unilaterally (Fig. 2).
Although outside incision diameters up to 12 cm have been advocated, those not exceeding 7 cm will reliably avoid problems with pleating, central flattening, wide scars, areolar spreading, and the loss of skin texture inherent in this technique. An alternative recommendation is that the ratio of outside diameter to areolar diameter should not exceed 2:1.14,15
A purse-string suture of permanent material reduces scar tension in circumareolar mastopexy. Placement
only along the outside circumference is less effective than the “wagon-wheel” method that also incorporates the areola. The latter better distributes and reduces wound tension.16
only along the outside circumference is less effective than the “wagon-wheel” method that also incorporates the areola. The latter better distributes and reduces wound tension.16
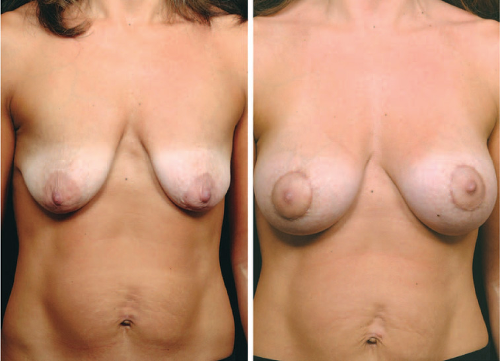 Fig. 2. Breast augmentation with circumareolar mastopexy. (Left) Preoperative view showing severe postpartum atrophy and grade II ptosis. (Right) Postoperative view; 300-g round silicone implants were placed in a subpectoral plane. |
The Benelli procedure is a true circumareolar mastopexy without augmentation. Extensive skin undermining exposes the parenchyma, which is then split to create flaps that are overlapped to provide coning and lift.17 This method is not recommended because the large central skin excision advocated causes the aesthetic problems described previously.
Vertical Mastopexy
Vertical mastopexy removes more skin than circumareolar techniques. It effectively raises nipple position and reduces circumareolar skin tension (Fig. 3). Both the splay angle between the vertical limbs and limb length will increase with increasing amounts of lower pole skin.
The greater these measurements, the higher the nipple position is elevated based on geometry (Fig. 4). Vertical mastopexy without simultaneous reduction does not significantly narrow the breast base.
The greater these measurements, the higher the nipple position is elevated based on geometry (Fig. 4). Vertical mastopexy without simultaneous reduction does not significantly narrow the breast base.
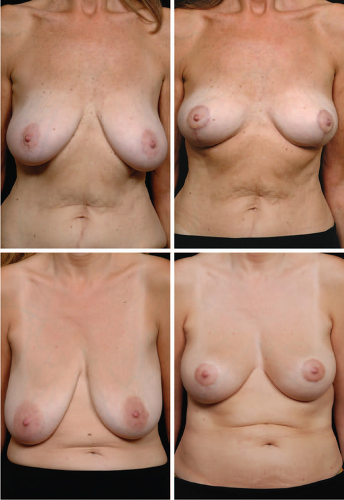 Fig. 3. Vertical mastopexy. (Above, left) Preoperative view showing low breast position and grade I ptosis. (Above, right) Postoperative view. Small amounts of tissue were resected from each side (left, 52 g; right, 94 g) but there was otherwise no parenchymal manipulation. (Below, left) Preoperative view showing grade II ptosis. (Below, right) Postoperative view following skin resection only. There was no parenchymal manipulation. |
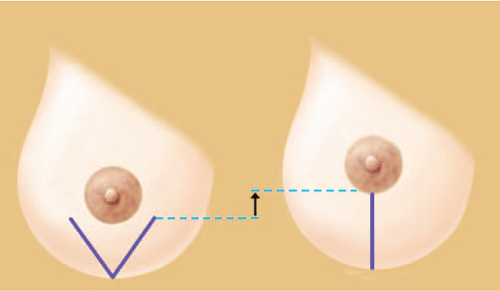 Fig. 4. (Left) The vertical limbs vary both in length and their angle of divergence depending on the amount of excess skin present. (Right) The nipple position is elevated based on simple geometry as the angle between the vertical limbs is closed. |
Vertical mastopexy can be used for grade I to III ptosis, but the scar burden may not be justified in mild cases. Adequate mobilization for nipple transposition can prove challenging when applied to patients with severe grade III ptosis.
Y-Scar Vertical Mastopexy
Y-scar vertical mastopexy deletes the superior portion of the circumareolar incision but is otherwise similar to vertical mastopexy.18 The requirements for its use are nearly normal areolar diameter and nipple position (Table 2). Sufficient nipple elevation accompanies vertical incision design geometry without the need for a superior periareolar incision component. The scar burden is perceptibly less with this technique (Fig. 5).
Circumvertical Mastopexy
Patients with significant ptosis, large areolas, and little skin between the areola and inframammary crease are poor candidates for standard vertical mastopexy. The paucity of lower pole skin dictates short vertical
limbs that diverge at a narrow angle. This minimizes the amount of nipple elevation possible. In addition, the vertical limbs may not diverge wide enough to skirt outside the areolar margin. Continuing the vertical limbs within the areolar skin results in patches of retained areolar skin along the vertical incision, something poorly tolerated by patients even when forewarned.
limbs that diverge at a narrow angle. This minimizes the amount of nipple elevation possible. In addition, the vertical limbs may not diverge wide enough to skirt outside the areolar margin. Continuing the vertical limbs within the areolar skin results in patches of retained areolar skin along the vertical incision, something poorly tolerated by patients even when forewarned.