CHAPTER 22 Managing submandibular glands
History
In search of the artistically pleasing neck through the addition of subplatysmal fat contouring and submandibular gland treatment
1968: Millard – Submandibular lipectomy.
1972: Millard – Submental and submandibular lipectomies in conjunction with rhytidectomy.
1978: Connell – Contouring the neck in rhytidectomy by lipectomy and a muscle sling.
1979: Aston – Platysma muscle alterations in rhytidoplasty.
1983: Owsley Jr. – SMAS-platysma face lift: a bidirectional cervicofacial rhytidectomy.
1985: Courtiss – Suction lipectomy of the neck.
1985: Giampapa – Neck recontouring with suture suspension and liposuction.
1990: Feldman – Corset platysmaplasty.
1991: de Pina – Aesthetic resection of the submandibular gland.
2006: Sullivan – MRI study demonstrating increasing submandibular gland ptosis with age.
Physical evaluation
• Key features of the aged neck include platysmal banding, pre- and/or subplatysmal fat deposits, skin laxity, and submandibular gland ptosis.
• Indications include young patients with a prematurely aged neck, or older patients with the neck contour issues as a prominent aspect of facial aging.
• Signs of cervicofacial aging may initially manifest as faint vertical platysmal bands overlying the thyroid cartilage and hyoid.
• These progress to longer, more pronounced bands as more support is lost from the retaining ligaments and the platysma descends further.
• A cervical obliquity, which may be composed of pre- and subplatysmal fat deposits.
• Submental fullness may be addressed with conservative contouring of pre- and or subplatysmal fat, but one must be concerned that this does not unmask submandibular gland ptosis.
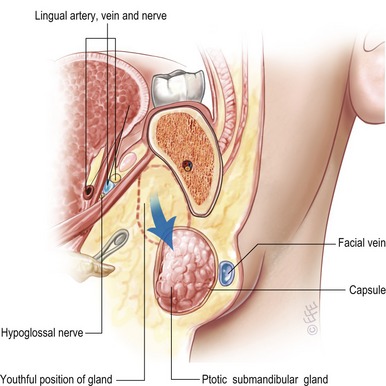
• Fullness laterally below the mandible, may be the result of the ptotic submandibular gland, and this may be addressed via gland resection or suspension.
• Patients undergoing other aesthetic facial surgical procedures may accentuate the appearance of untreated submandibular gland ptosis.
Technical steps
Ligaments in the neck, analogous to the retaining ligaments in the cheek, help suspend the soft-tissues. The mandibular ligaments affix the overlying skin to the inferior aspect of the mandible, and help to define the anterior aspect of the jowls in the aged face. The thin fascial support in the preauricular region is the platysma-auricular ligament, and attaches the posterosuperior platysma to the skin. Anteriorly, the skin is tethered to the superficial musculoaponeurotic system SMAS and platysma via the anterior platysma–cutaneous ligaments. These ligaments check the descent of the soft-tissues of the neck in aging, and are disrupted to allow for proper redraping of the skin during neck rejuvenation.
SMAS suspension/platysmal plication
The anterior platysma is approached through a transverse submental incision (Fig. 22.1). The submental skin and a smooth, consistent layer of adjoining fat are then undermined inferiorly to the level of the cricoid. To correct the platysmal bands, the muscle is freed on the edges from the deeper subplatysmal fat and anterior bellies of the digastric muscles. The platysmal edges are grasped with forceps and brought together in the midline. The excess tissue is then resected as described below, and the edges brought together with interrupted and then a running suture from inferior to superior.