This article provides an overview of scar management within the forehead region. It addresses the unique challenges specific to the treatment of forehead wounds. A logical, stepwise approach is used. A subsite based treatment algorithm is provided along with a review of current best practices. Pertinent case examples are included for demonstration purposes.
Key points
- •
The homogenous topography of the forehead makes the creation of inconspicuous scars challenging.
- •
Careful preoperative planning, open communication, and setting realistic expectations are vital to any scar revision case.
- •
Use natural borders (hairline, brow, temporal line, facial rhytids) to disguise scars whenever possible. Hair transplant can help restore appearance when scars involve hair-bearing skin.
- •
Protection of function always takes priority over restoration of form.
- •
Convex, contracted scars may benefit from injection of filler, including fat transfer.
Introduction
Injuries to the forehead pose several challenges to the facial plastic and reconstructive surgeon. Some of these challenges are held in common with other facial regions, and others are unique. This article is designed to take the reader through an organized, stepwise approach to acute and chronic scar management of the forehead region. Forehead wounds may present for a variety of reasons, including facial trauma, defects remaining after excision of malignant or nonmalignant lesions, the result of congenital facial lesions, and from iatrogenic causes.
Reconstruction of forehead wounds can be approached using a standardized and complete methodology. Repair may range from local wound care, primary closure, local tissue rearrangement, regional flap reconstruction and complex free tissue transfer, or any combination thereof. In addition to optimizing the patient’s aesthetic appearance, goals of repair include protection of vital structures, prevention of infection, and avoidance of chronic wound complications.
Successful reconstruction depends on several synergistic factors. The nature of the wound, careful preoperative planning, surgical competence, and the global medical status of the patient all play a role. When one of these pillars of wound repair are lacking, the others become even more important. Patients who smoke, have vasculopathy, or are not medically stable to undergo an intensive procedure may have limited options for repair. The importance of this concept cannot be emphasized enough for the neophyte surgeon. Patients may require serial procedures (in the case of tissue expander use, for example), and the possibility of this should be discussed up front. Depending on the nature of their injury, patients may remain significantly disfigured, even after the best possible reconstructive effort has been executed well. It is vital for the surgeon to maintain open and honest communication with the patient throughout the reconstructive journey.
A scar is the final, unavoidable result of any wound, whether it is repaired masterfully or neglected in its entirety. Facial scarring can be particularly troublesome to patients because it is something the patient and those they encounter will see on a daily basis. Even if vital structures have been protected and function restored, an unappealing facial scar can cause persistent and significant emotional suffering in patients. Surgeons can minimize the impact of facial scarring on a patient through careful planning and the use of optimal reconstructive measures.
Scars are fluid, evolving over time. They change in color when healing and when exposed to various environmental factors such as sunlight or a chemical irritant. They change in shape when exposed to tension or movement during wound healing. Although the strength of a scar builds over time, it will never regain the full resilience of native tissue. Last, scars are subject to hereditary forces. Some patient’s wound healing may be burdened with the challenges of dyschromias, scar hypertrophy, or keloid reactions over time. The successful facial plastic surgeon uses a broad armamentarium to address the unique needs of each patient and optimize final outcomes.
Introduction
Injuries to the forehead pose several challenges to the facial plastic and reconstructive surgeon. Some of these challenges are held in common with other facial regions, and others are unique. This article is designed to take the reader through an organized, stepwise approach to acute and chronic scar management of the forehead region. Forehead wounds may present for a variety of reasons, including facial trauma, defects remaining after excision of malignant or nonmalignant lesions, the result of congenital facial lesions, and from iatrogenic causes.
Reconstruction of forehead wounds can be approached using a standardized and complete methodology. Repair may range from local wound care, primary closure, local tissue rearrangement, regional flap reconstruction and complex free tissue transfer, or any combination thereof. In addition to optimizing the patient’s aesthetic appearance, goals of repair include protection of vital structures, prevention of infection, and avoidance of chronic wound complications.
Successful reconstruction depends on several synergistic factors. The nature of the wound, careful preoperative planning, surgical competence, and the global medical status of the patient all play a role. When one of these pillars of wound repair are lacking, the others become even more important. Patients who smoke, have vasculopathy, or are not medically stable to undergo an intensive procedure may have limited options for repair. The importance of this concept cannot be emphasized enough for the neophyte surgeon. Patients may require serial procedures (in the case of tissue expander use, for example), and the possibility of this should be discussed up front. Depending on the nature of their injury, patients may remain significantly disfigured, even after the best possible reconstructive effort has been executed well. It is vital for the surgeon to maintain open and honest communication with the patient throughout the reconstructive journey.
A scar is the final, unavoidable result of any wound, whether it is repaired masterfully or neglected in its entirety. Facial scarring can be particularly troublesome to patients because it is something the patient and those they encounter will see on a daily basis. Even if vital structures have been protected and function restored, an unappealing facial scar can cause persistent and significant emotional suffering in patients. Surgeons can minimize the impact of facial scarring on a patient through careful planning and the use of optimal reconstructive measures.
Scars are fluid, evolving over time. They change in color when healing and when exposed to various environmental factors such as sunlight or a chemical irritant. They change in shape when exposed to tension or movement during wound healing. Although the strength of a scar builds over time, it will never regain the full resilience of native tissue. Last, scars are subject to hereditary forces. Some patient’s wound healing may be burdened with the challenges of dyschromias, scar hypertrophy, or keloid reactions over time. The successful facial plastic surgeon uses a broad armamentarium to address the unique needs of each patient and optimize final outcomes.
Management and treatment
Overview
Scar management begins at the time of cutaneous insult. Wounds should be cleaned, and copious irrigation used. Anesthesia (local, intravenous, or general) may be needed for adequate debridement and examination. Never allow treatable patient discomfort to limit one’s initial examination. Depending on the wound class, antibiotics may be indicated. In cases of polytrauma, where the facial wound is not a singular injury, cooperation with several other treatment teams may be necessary. When forehead wounds are the result of a surgical excision, these primary steps may have already occurred.
In comparison with other facial regions, the forehead is relatively devoid of geometric complexity. Any aberration of the symmetric, gentle contour, and homogenous appearance of the forehead readily stands out to the observer. A concave scar within the convex topography of the mid-forehead can cast shadows and distort light reflection patterns, making an otherwise innocuous scar readily stand out.
A complete understanding of facial anatomy as well as the biomechanical interactions that occur both acutely and over time within the face is a foundational principle in successful facial reconstruction. One of the first things a surgeon should become facile with is facial analysis. Facial analysis helps to define both aesthetic ideals, as well as aberrations. Facial analysis can be performed from many observer views (frontal, oblique, profile), but forehead analysis is often most helpful using the frontal view. One should be careful not to perseverate with exacting geometric definitions at the expense of patient preference and the pursuit of global facial harmony.
All forehead intervention must take into consideration the effects it will have on adjacent key anatomic structures. Forehead tissues are generally unforgiving, and distortion of adjacent subsites is a frequent challenge. It is also important to anticipate future changes, such as the effect of balding on hairline shape and location. A carefully placed scar line within a young male’s hairline may become painfully obvious several years later.
Facial Analysis
The facial frame can be divided into subunits both vertically and horizontally. Facial height can be divided into thirds, with the forehead comprising the superior third. The superior third (forehead) is defined as running from trichion to glabella ( Fig. 1 ). Although typically described as the superior third, variability in a patient’s hairline may result in the forehead subunit comprising significantly more or less than one-third of the overall vertical facial dimension.
The face can also be subdivided into vertical segments using the facial vertical fifths model. This results in 3 unique vertical subunits: mid-forehead, paramedian, and lateral (temporal; see Fig. 1 ). The lateral forehead subunit is concave in shape. It is bordered by the hairline posterosuperiorly and the temporal line and lateral orbital rim anteriorly. The paramedian forehead region is bordered superiorly by the hairline, and inferiorly by the superior orbital rim and overlying brow. The mid-forehead region is bound superiorly by the hairline (including the trichion), and inferiorly by the glabella and nasal root (nasion, sellion, and rhinion).
Mid-Forehead
When using the facial fifths model of facial analysis, the mid-fifth describes the mid-forehead region. It is the only nonpaired subunit of the forehead. Its topography is homogenous and it is the most projected subunit of the forehead. The surface anatomy is largely convex in nature. It contains the medial border of both frontalis muscles. The frontalis is the anterior muscle belly of the occipitofrontalis muscle. Owing to the lack of frontalis muscle in the midline, the mid-forehead region is amenable to either vertical or midline scars. This region contains both horizontal rhytids (frontalis, procerus) and vertical rhytids (corrugator supercilii).
Superior mid-forehead defects may be closed with advancement flaps. Trichophytic incisions, or those placed within the hairline (as would be done for a coronal approach), may be used to gain further tissue laxity. An example of this is an O-T rotational flap to close a superior mid-forehead defect adjacent to the hairline. Midline vertically oriented scars may be less likely to undergo scar widening owing to the lack of frontalis muscle activity during healing. Inverted V–Y advancement flaps may help to obviate eyebrow medialization with primary closure of glabellar wounds.
Paramedian Forehead
The paramedian forehead is bordered inferiorly by the superior orbital rim, laterally by the temporal line, and medially by the border of brow/canthus. Notable skeletal landmarks include the prominence of the supraorbital rim. The majority of sensory innervation of the forehead is provided via terminal branches of the ophthalmic division (V 1 ) of the trigeminal nerve. The supratrochlear neurovascular bundle lies medial to the supraorbital neurovascular bundle and runs beneath the corrugator supercilii and frontalis muscles. The supraorbital notch, which may be palpated along the superior orbital rim, lies approximately at the junction of the mid and medial thirds of brow. These nerves are paired with the supraorbital and supratrochlear vessels. In most patients, the supraorbital structures exit via a notch. However, in approximately 10% of the population, the neurovascular structures may exit slightly more superiorly via a true foramen. These patients are at increased risk for injury during dissection. Overlying this is the eyebrow. Although eyebrow hairs do not undergo balding patterns intrinsic to scalp hair, the surgeon should consult the patient regarding facial grooming patterns (shaving, plucking, waxing), because this may alter the brow shape and brow line. This area holds several key neurovascular structures, namely the supratrochlear artery and nerve, and the supraorbital artery and nerves. The inferior border of the paramedian region involves periorbital structures including the brow and upper eyelid.
The degree of bossing of an individual’s forehead varies, but the region from the midline to the midpupillary line is convex. The relaxed skin tension lines (RSTLs) in the forehead are horizontal. When possible, horizontally oriented incisions are preferred to allow maximal scar camouflage. Eyebrow elevation is of particular importance in this forehead region. When large defects (>3 cm) are closed primarily in a horizontally oriented plane, the result often yields excessive eyebrow elevation. Defects near the hairline in the paramedian forehead that are closed in a horizontal fashion impact the eyebrow much less compared with inferiorly based defects. When defects will effect eyebrow elevation, the surgeon can limit this by suturing the eyebrow dermis and the underlying muscle to the periosteum of the superior orbital rim.
To minimize scar for defects of the paramedian forehead near the hairline, a bipedicle advancement flap is used. Bipedicle flaps are recruited from tissue superior to the defect and the incision is carried full thickness to the galea. The bipedicled flap is well-vascularized by the subdermal plexus and provides a hidden scar. One of its drawbacks is lowering of the anterior hairline. Of note, the longer the releasing incision for the bipedicled flap, the greater mobility the flap has. Advancement flaps are used to close skin defects in the paramedian forehead, which are not amenable to primary closure. Incisions are made along the horizontal RSTLs. Flaps are made at a 4:1 ratio of length to width and are dissected in the subcutaneous tissue plane, superficial to the neurovascular bundle. Effective dissection in the correct plane, squaring of the defect borders, and removing standing cutaneous deformities is imperative to appropriate scar formation. An effective method to camouflage scar formation is to make the flap slightly wider than necessary to hide incisions in nearby skin creases.
Management of a scar in the paramedian forehead region can be challenging. Thus, attempts should be made by the surgeon to avoid vertical, curvilinear, and oblique incisions because they result in scars that are not in the RSTLs. The majority of defects should be repaired primarily in a horizontal orientation or reconstructed with horizontally oriented unilateral or bilateral advancement flaps. Further, vertically oriented primary repair should be avoided. Rotation and transposition flaps should also be avoided.
In paramedian forehead wounds, which include the brow, additional procedures such as lateral cantholysis may be required to address the integrity of the eyelid. Other options in the brow region include a pedicled forehead flap. If a significant amount of tissue loss occurs in the supraorbital region, reconstruction may result in a similar effect as a direct brow lift. In such cases, it is reasonable to consider addressing the contralateral face to maintain symmetry. Periorbital defects extending below the eyebrow are discussed in a different chapter of this text.
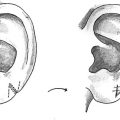
A good method for closure of moderate sized defects within the paramedian and temporal region is the hatchet or double hatchet flap ( Fig. 2 ). Gurunluoglu and colleagues describe its use within the region for primary closure of defects up to 3.5 cm in maximum diameter while maintaining neurovascular integrity of the region. This flap design allows for optimal rotation and wound coverage, while minimizing tension and distortion of adjacent subunits. The incisions should be designed in such a manner as to align with the hairline and facial rhytids if possible.