Various methods are available for refining scars of the external nose and optimal scar revision frequently requires the utilization of multiple techniques. Differing anatomy of nasal subunits and their underlying structural framework limit surgical options in nasal scar revision compared with other areas of the face. An understanding of a variety of laser technologies and their specific applications can vastly aid in fine, controlled scar revision. Achieving optimal scar reduction regularly requires multiple stages of intervention, close follow-up, and repeat procedures.
Key points
- •
Various methods are available for refining scars of the external nose and optimal scar revision frequently requires the utilization of multiple techniques.
- •
Differing anatomy of nasal subunits and their underlying structural framework limit surgical options in nasal scar revision compared with other areas of the face.
- •
An understanding of a variety of laser technologies and their specific applications can vastly aid in fine, controlled scar revision.
- •
Achieving optimal scar reduction regularly requires multiple stages of intervention, close follow-up, and repeat procedures.
A main focus of facial aesthetic surgery is to draw attention to the eyes. Any imperfection in nasal contour that leads to asymmetry will be noticed, and this emphasizes the importance of treating nasal injury and scar formation aggressively. The flexible cartilaginous framework of the nose is enveloped by a skin soft tissue envelope (SSTE) of variable thickness. It is this framework particularly over the nasal tip that must counter the forces generated by wound healing and contracture. In contrast, over the superior nasal dorsum (supported by bone), and the middle vault (by the relatively firm fusion of the dorsal quadrangular and upper lateral cartilages) deformation of the SSTE is less dramatic after injury or defect closure. The varying thickness of the skin in combination with the varying stability of the structural framework (eg, tip vs dorsum) leads to differences in response in contrast to scar and injury management in most other regions of the face. This is amplified by the ability of the eye to discern even small changes in facial symmetry and structure. For example, the smallest amount of contracture at the alar rim or soft tissue triangle can result in asymmetry and thus noticeable deformation. In contrast, injury and subsequent scar formation over the osseous nasal framework can be treated conservatively, as the surface is firm and adjacent skin is linked to bone via periosteal attachments.
Finally, the nose is a functional organ that supports air flow and mechanically filters, warms, and humidifies inspired air. Significant scarring can lead to collapse of the internal and external nasal valves. All nasal surgeons must appreciate this when planning wound management or reconstruction and when deciding how to best treat nasal scars and defects.
Management and treatment
The Art of Doing Nothing
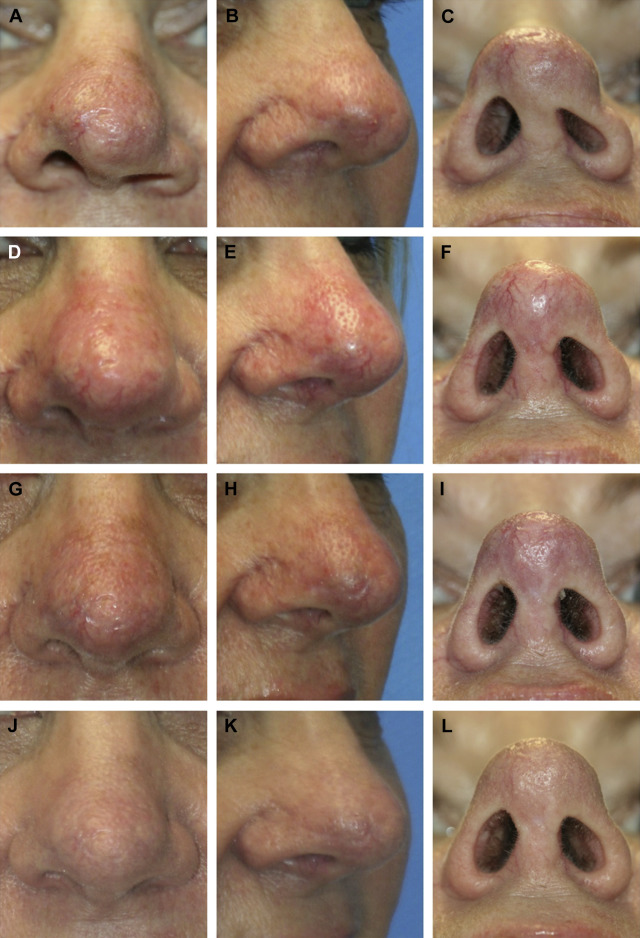
Healing by secondary intention can produce stable outcomes that are cosmetically acceptable, when applied in a measured and judicious manner. This is important to consider especially with early scars produced by thermal injury or ballistic trauma in which the true extent of injury evolves over time. Aggressive local wound care is important, and this can be time and labor intensive, requiring frequent office visits and constant patient reassurance. The key is to strike a balance between doing the least-invasive treatment possible and obtaining the best results ( Fig. 1 ). As no reconstructive surgery is performed, injury to normal adjacent tissue is minimized and other treatment options are preserved for future reconstruction if required. Adjunctive therapies, such as hyperbaric therapy, local steroid injections, silicone dressings, massage, pulsed dye laser, fractionated laser, and microneedling may have value for modulating the evolving scar process. This works best over a concave surface overlying a firm bony framework, such as in the nasal dorsum adjacent to the canthal region.
Laser and Resurfacing
In our practice, the laser has largely replaced dermabrasion. Although many surgeons achieve outstanding results with dermabrasion, we focus on laser resurfacing for this section. The risk of laser devices to both physician and patient must be appreciated, and proper eye protection is imperative. A comprehensive understanding of the physiology of laser treatments for scars is evolving as technology advancement exceeds the rate of clinical adoption and use. In our practice, laser technology is used both early and later in treatment protocols. We often start scar treatments with laser resurfacing and remodeling to varying degrees. This timing then allows us to better define the scar, to soften it, and to build the local collagen and tissues for any future reconstructions. If surgical scar revision is required, the reconstruction is followed again by more laser treatments to assist with tissue remodeling.
Laser fundamentals are beyond the scope of this article, but the advantage of laser therapy is that specific epidermal and dermal structures can be selectively targeted through precise selection of dosimetry, and as a noncontact technique there is no mechanical trauma to the skin. In contrast, one limitation of dermabrasion (using sandpaper or rotary burrs) is that force is exerted on the tissue, and this may distract wounds. Hence, dermabrasion is seldom used during the acute phases of wound healing, and frequently it is used at 8 weeks. Our laser treatment protocols begin on the day of suture removal, during the acute phase of wound healing. We then select the appropriate wavelength and dosimetry parameters depending on what each injury requires and how it is likely to respond to treatment. A typical approach would start with pulsed dye laser therapy at suture removal with consideration of fractional ablative resurfacing 2 weeks later. Pulsed dye lasers target the scar vasculature. The fractional ablative resurfacing can be every 4 weeks for up to 5 treatments. At approximately 5 to 6 weeks, nonablative lasers maybe used at 2-week to 4-week intervals to support collagen remodeling.
For early scar redness and erythema, a “vascular” laser, such as the 595-nm pulsed dye laser is used. Light from this laser is preferentially absorbed by hemoglobin. Being nonablative, it creates no eschar for the patients to care for following treatment. Scars will have many different-sized blood vessels and the laser settings can be adjusted to target each specifically. The pulse width can be set shorter for smaller vessels and longer for larger vessels. For general redness and erythema, we use settings similar to rosacea treatments: an energy density of 7.5 J/cm 2 with a 6-ms pulse width using a 10-mm spot size. We often make 2 passes to complete a single treatment. It is valuable to have a built-in cooling device or cooling technique to allow the epidermis to be cooled selectively. The laser we use is the V-Beam Perfecta (Syneron/Candela, Wayland, MA) with a 30/30 cooling setting (30 ms spurt of cryogen with a 30-ms delay until laser burst). For larger vessels and telangiectasias, the laser can be set to an energy density of 12.5 J/cm 2 , 20-ms pulse width, and 30/30 cooling using a 7-mm spot size. Often a specific scar will get different treatment protocols at the same time depending on what is causing the erythema. It is important to allow the tissue to cool and to not be overly aggressive, as burns and blisters can occur.
For dermal collagen remodeling, the nonablative fractional 1550-nm wavelength lasers can be used with multiple passes. This is often used in a fractional manner with multiple passes. Typically this laser is reserved for depressed scars that require multiple treatments to restore collagen over time. These lasers can generate significant temperature elevations, and without the traditional visual feedback of pinpoint bleeding seen with ablative lasers, burns and blisters are possible. It is important to wait at least 1 minute between each successive pass to allow the skin to thermally relax. A common setting used in our practice for nasal tip or dorsal scars is an energy of 45 mJ, treatment coverage area of 26% delivered with 6 passes. Again, it must be stressed to cool the superficial skin between each pass for extended periods (at least 1 minute with a cooling technique) to prevent burns and blistering.
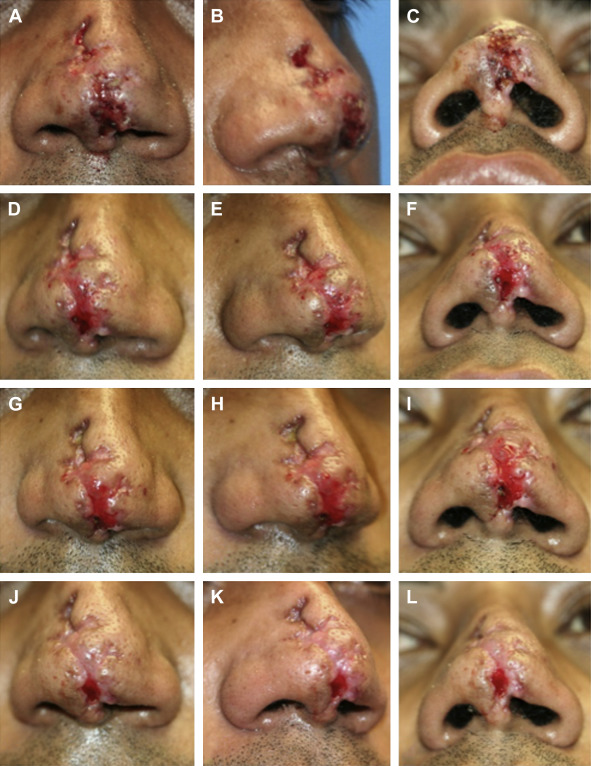
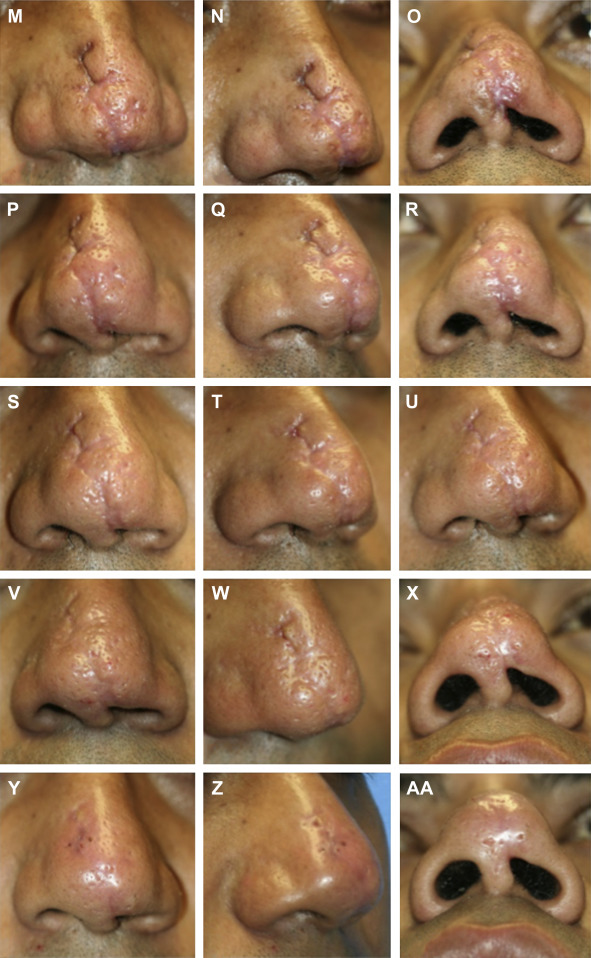
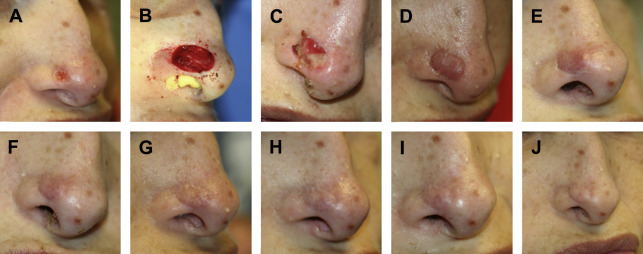
Ablative lasers have the highest water absorption peaks and thus lead to destruction and removal of the superficial epidermal and dermal tissue. In our practice, we use the 2940-nm wavelength Er:YAG laser with a tunable pulse duration. Er:YAG has high absorption in water, and thus a vertically shallow optical penetration depth. The 10,600-nm wavelength CO2 laser is also frequently used in this regard as well by many surgeons with excellent results, although thermal injury and depth of ablation are substantially deeper. These ablative lasers are used in a fractional pattern of 11% to 22% treatment coverage area with multiple passes as desired. A standard protocol for a hypertrophic nasal scar is 500 μm of depth of ablation, 11% of fractional treatment coverage area delivered with 3 passes. Pinpoint bleeding will be obtained similar to dermabrasion. This protocol will require posttreatment wound care and prophylaxis at the discretion of the surgeon ( Fig. 2 ).
Surgical Scar Revision
Surgical revision of nasal scars is indicated when the scar distorts the natural contours of the nose. A tight scar band can pull the ala medially for example. This can be released with a Z-plasty to reorient the scar and then followed by laser treatments as indicated to blend the incisions.
Depressed scars with resulting soft tissue defect can be replaced with a full-thickness skin graft (FTSG) to release the pull and straining created from contraction. Fig. 3 shows an example of when an FTSG can be used to fill the soft tissue defect. Grafting can be followed by laser as stated previously to blend the areas. This patient elected to have no further treatment beyond the FTSG.
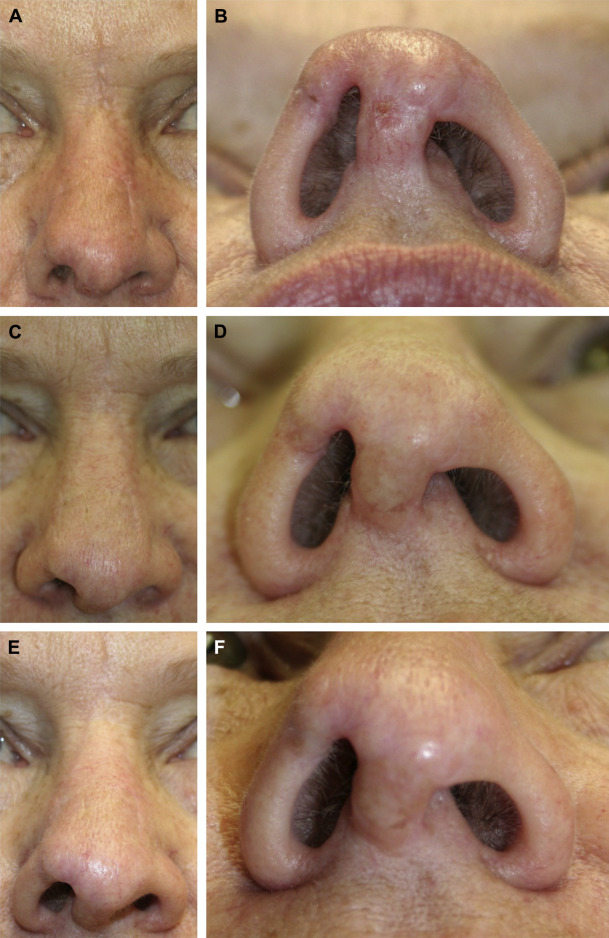
The soft tissue triangle area of the nose is a particular area of interest to the nasal surgeon. This web of tissue has the propensity to be easily distorted by scar. It is a classic scenario that the soft tissue triangle is scared leading to retraction and notching of the ala. This can be repaired with an auricular composite graft to supply the needed rigid framework in conjunction with soft tissue simultaneously. Alar retraction is a common consequence of nasal reconstruction and trauma as well, and can be treated with composite grafts to the vestibular inner lining or by using structural rhinoplasty techniques, as seen in Fig. 4 .