Fig. 11.1
Malignant proliferating trichilemmal tumor. A single hard, slow-growing nodular swelling 3 × 3 cm on the scalp. The lesion relapsed one year after excision
Pathology
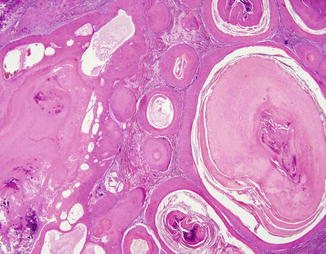
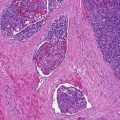
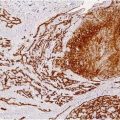
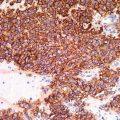
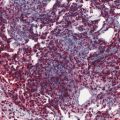
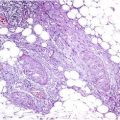
The diagnosis of malignancy in these tumors is based predominantly on histological features. Multiple lobulated masses of squamoid epithelium filled centrally with homogeneous acellular eosinophilic material representing amorphous debris and pilar keratin are seen throughout all the dermis (Figs. 11.2 and 11.3) separated by fibrous or myxoid stroma. Areas of calcification are often present (Fig. 11.3). Trichilemmal keratinization (abrupt transition of a nucleated epithelial cell to an anucleate, keratinized cell without the formation of a granular layer) is a typical diagnostic clue. Foci of single cell necrosis and mitotic figures are present. In addition, the squamous cells may show slight cytologic atypia or manifest large, hyperchromatic nuclei with irregular nuclear membranes surrounded by abundant eosinophilic cytoplasm with infiltrative pattern reminiscent of squamous cell carcinoma. A minimal to moderate infiltrate of mononuclear inflammatory cells was identified as well as foreign body giant cell reaction to keratin. No lymphovascular or perineural invasion is noted. The tumor usually shows loss of staining for CD34, positivity for p53, high proliferative activity with Ki67, and DNA aneuploidy.
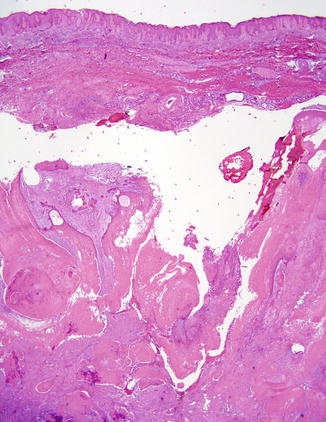
Fig. 11.2
Malignant proliferating trichilemmal tumor. Beneath the epidermis, multiple lobulated expansile masses of squamous cells with non-lamellated trichilemmal keratinization and patchy calcification are seen throughout the dermis and subcutis