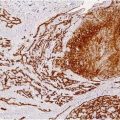
Fig. 20.1
Malignant cylindroma. The tumor is composed of dermal irregular cords and nests with an infiltrative pattern of growth, without connection to the epidermis
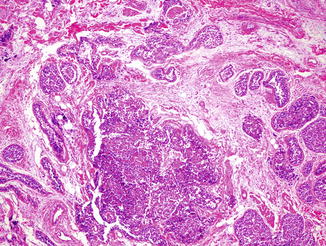
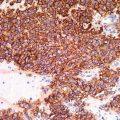
Fig. 20.2
The tumor forms expansile nodules, sometimes showing ductal differentiation
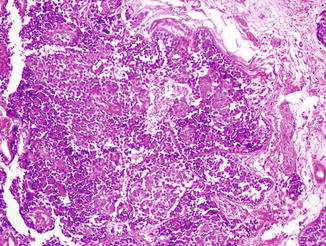
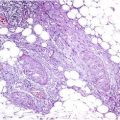
Fig. 20.4
The tumor reveals areas with atypical cells, loss of the dual population and necrosis
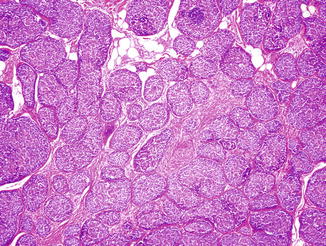
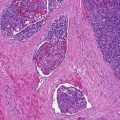
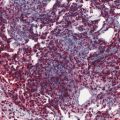
Fig. 20.3
Scattered throughout the tumor are residual benign cylindromatous foci, characterized by a dual cell population organized into basaloid islands, surrounded by a hyaline, thick, basal membrane with the typical “jigsaw” pattern
Differential Diagnosis
The diagnosis is a histological one and depends on the recognition of preexisting benign cylindromatous foci.
Prognosis
MC is a high-grade neoplasm, with a recurrence rate of 36 % and a metastasis rate of 46 %, with involvement mainly of the lymph nodes, liver, lung, and bones.
Treatment
Wide surgical excision with adequate margins has to be considered the treatment of choice, while high-dose radiation is an option suggested to treat inoperable tumors.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


